
Dorsal distraction plating offers superior patient satisfaction and fewer complications compared to external fixation in comminuted intra-articular distal radius fractures. While both methods yield comparable long-term functional and radiological outcomes, bridge plating facilitates improved daily functioning and cosmetic acceptance in the early recovery phase.
Dr. Ismail Pandor, Department of Orthopaedic Surgery, Krishna Vishwa Vidhyapeeth, Karad - 415539, Maharahtra, India. E-mail: i.pandor07@gmail.com
Introduction: Fractures located in close proximity to the lower end of the radius bone, which make up around 16% of fractures requiring emergency treatment require careful treatment to regain mobility in the wrist joint and the fingers. Although classic external fixation (ExFix) methods are widely used, newer procedures such as dorsal distraction plating are showing potential . This study investigates the concepts, debates, and results of several methods so that to determine the most effective fracture treatment.
Materials and Methods: The experiment will recruit individuals with intricate fractures affecting the joint across the distal region of the radius. The patients will be randomly randomized to receive either dorsal distraction plating or ExFix. Pre-operative, post-operative, and follow-up assessments will involve clinical and radiographic examinations. Functional outcomes will be evaluated using standardized scoring systems . A comparative statistical analysis will be performed to assess the outcomes obtained from both groups.
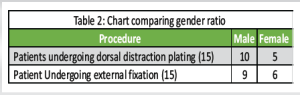
Results: The average ages across the bridge plate and ExFix sections were 40 and 43 years, respectively. The cohort of patients who had bridge plating exhibited a greater prevalence of male individuals (P = 0.011). The ExFix group had elevated infection rates, which can be ascribed to the occurrence of pin tract infections. Both the groups did not show any instances of nerve palsy. Patients who received dorsal distraction plating expressed higher levels of satisfaction with their post-operative results, both in terms of functionality and appearance .
Discussion: Patients treated with dorsal distraction reported fewer issues. Although a few difficulties were observed, the most of these patients expressed high levels of satisfaction with the results of their surgical procedures . The findings suggest that dorsal distraction may offer a more favorable balance between functional recovery and patient satisfaction, highlighting a potential advantage over ExFix. In the long run, however, the functional outcomes of both the techniques were found to be similar.
Conclusion: Dorsal bridge plating is a viable substitute for ExFix in treating distal radius fractures. The use of dorsal bridge plating demonstrated greater performance in daily activities, despite the fact that the functional and radiological findings at 6 months were found to be almost indistinguishable in both groups .
Keywords: Radiological and functional, radius fractures, external fixation, dorsal distraction plating.
Fractures at the far side of the radius bone, especially those that are broken into multiple pieces and shifted out of place, provide a difficult problem in orthopedic therapy. A crucial element in the healing process of these fractures is the restoration of articular congruity, aiming to provide functional and pain-free mobility of the wrist and fingers. Due to the substantial prevalence of these fractures, which comprise approximately 16% of all fractures seen in emergency departments [1], it is imperative to have treatment choices that are efficient and produce desired results. Although surgical intervention is usually only used for fractures that are displaced or unstable, there is still debate over the best technique to take[2]. Conventional techniques such as external fixation (ExFix), which involve reducing the fracture by closed or limited open approaches and applying a frame that spans the fracture, have been widely used for a long time [3]. Nevertheless, more recent methods like dorsal distraction plating are developing as encouraging alternatives [4].
Distraction plating involves the use of a plate as an internal stabilizer. It utilizes ligamentotaxis to realign and maintain the length of the bone, while also providing enough stability for the healing process. The device can be fastened to either the second or third metacarpal, with research investigating the anatomical and biomechanical consequences of either method. This surgical procedure yields favorable X-ray results and promotes functional restoration. After the fracture has fully healed, it is customary to remove the plate to regain normal wrist mobility. This study examines the fundamental principles, debates, and results related to these treatment methods in the therapy of distal radius fractures.
Aim
The aim of the present investigation is to evaluate and contrast the effectiveness of dorsal distraction plating and ExFix in managing comminuted terminal radius fractures, with the objective of identifying the most successful surgical approach.
Objectives
- The aim of the research is to assess and contrast the functional results of patients who underwent treatment for comminuted distal end radius fractures with intra-articular extension. The two treatment modalities being compared are dorsal distraction plating and ExFix
- To evaluate the radiographic parameters, such as fracture reduction and alignment, in both groups undergoing therapy
- To examine the complexities and negative consequences linked to each treatment option
- To assess the influence of these interventions on patients’ daily activities, occupation, and overall quality of life.
Approach
Criteria for inclusion
- Individuals suffering from closed comminuted intra-articular fractures at the lower end of the radius
- Patients of both sexes
- Age range: 20–50 years.
Criteria for exclusion
- Patients with multiple traumatic injuries
- Individuals suffering from compound fractures
- Individuals with a history of prior surgery for fractures in the distal radius or forearm
- Patients with concomitant tendon injury
- Patients with pre-existing neurological deficits
- Patients with pre-existing malformations.
Data collecting
The objective of this study is to enlist patients who have intricate fractures occurring at the lower portion of the radius, which encompass several bone pieces within the joint. These patients will be assigned randomly to either the dorsal distraction plating or ExFix group. Pre-operative, post-operative, and follow-up visits will include clinical and radiographic examinations. Standardized scoring systems will be used to measure functional results[4]. Statistical analysis, utilizing t-tests and Chi-square tests, will be utilized to compare the outcomes of the two therapy groups. The study will prioritize ethical considerations and ensure that informed permission is obtained from all participants. Patients will undergo evaluations immediately after the surgery, at a follow-up appointment 1.5 months later, and at another follow-up appointment 3 months later.
Research data
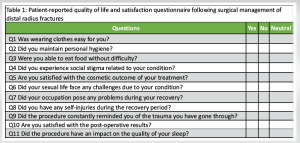
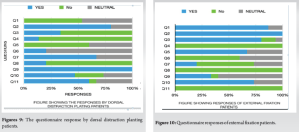
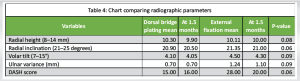
This study comprised a cohort of 30 patients who received a diagnosis of comminuted distal radius fractures. The purpose was to assess the treatment outcomes of two different methods: Dorsal bridge plate (used in 15 patients) and ExFix (used in 15 patients). The assessment included both radiological and clinical characteristics. The post-therapy anatomical alignment was evaluated by radiographically evaluating the radial inclination angle, radial height, and volar tilt. The clinical assessments consisted of measuring the range of motion in the wrist, grip strength, and pain levels. To assess the ability in carrying out daily tasks effortlessly. The individuals taking part were instructed to indicate their answers, which were later examined and displayed on a graph for comparative assessment as mentioned in Table 1.
Surgical procedures
Exfix: ExFix is a commonly used surgical technique to stabilize fractures at the distal end of the radius, particularly in cases where the fractures are fractured or involve the joint. The process commences by administering either regional or general anesthetic to assure the patient’s comfort. After the patient has been administered anesthesia, the surgical site is prepared and covered with sterile drapes.
The surgeon usually creates small incisions at predetermined locations to place the pins. These areas are often situated around the fracture site on the radius and metacarpal bones.
Fluoroscopic guiding is employed to percutaneously introduce Schanz pins into the bone. The positioning of these pins is done with great care to prevent any damage to neurovascular structures and to ensure the best possible stability. Subsequently, the pins are linked to an ExFix structure that can be modified to attain accurate alignment and reduction of the fracture.
After positioning the frame, the surgeon skillfully adjusts the broken pieces of the fracture to realign them with the body’s natural structure. This reduction is confirmed with the use of fluoroscopy. If necessary, more modifications are implemented to the fixator in order to attain the desired alignment. Subsequently, the fixator frame is firmly fastened to ensure the maintenance of the decrease.
Once the fracture alignment and stabilization have been successfully achieved, the surgical incisions are closed using sutures or sterile dressings. After surgery, the ExFix permits limited wrist joint mobility while ensuring the stability of the fracture, which facilitates early functional rehabilitation.
- B) Dorsal distraction plating is a surgical technique that involves the use of plates to distract and stabilize the dorsal aspect of a bone.
Dorsal distraction plating is a surgical technique employed to stabilize distal radius fractures, particularly those that are comminuted or intra-articular in origin. The injured limb is prepared and covered with sterile drapes under either regional or general anesthesia. A surgical cut is made down the back side of the forearm, specifically across the lower end of the radius bone. The extensor retinaculum, a band of tissue that holds the extensor tendons in place, is also cut to move the tendons aside and reveal the location of the fracture.
The fracture pieces are precisely aligned using direct vision and fluoroscopic assistance. A pre-contoured dorsal plate, usually with a low-profile design, is placed dorsally on the lower end radius. The plate extends across the fracture, offering firm stabilization by means of several locking and non-locking screws put into the proximal and distal fragments. Efforts are made to prevent any interference with the extensor tendons. Fluoroscopic imaging verifies the ideal placement of the plate and the proper alignment of the fracture. The surgical incision is flushed with a sterile saline solution and then sealed using many layers, with subcuticular sutures employed specifically for the skin.
After the surgery, the wrist is placed in a splint or cast to prevent movement and support the initial healing process. Follow-up involves the use of sequential radiographs to evaluate the healing of the fracture and the correct positioning of any surgical implants. Dorsal distraction plating provides strong stabilization, allowing for prompt movement and restoration of function. Physical therapy is started once X-ray imaging confirms that the wrist has healed enough to regain its range of motion and strength. Subsequently, after the removal of the implant, adhesiolysis is carried out during the surgery to regain the mobility of the wrist joint. Dorsal distraction plating X-rays (Fig. 1, 2, 3, 4). ExFix X-rays (Fig. 5, 6, 7, 8, 9).



The average ages for the bridge plating and ExFix categories were 40 and 43 years, respectively. The group of patients who underwent bridge plating had a significantly larger proportion of male patients (P = 0.011). Both groups demonstrated similar rates of union.
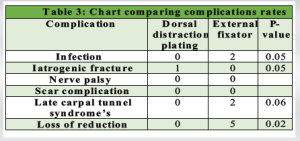
The ExFix group exhibited elevated infection rates, which can be ascribed to the presence of pin tract infections [5].
Neither group reported any cases of nerve palsy.
Patients who received dorsal distraction plating expressed higher levels of satisfaction [6] over their post-operative results, both in terms of functionality and appearance. They experienced more ease in carrying out daily tasks such as eating and reported improved sleep quality. On the other hand, patients who underwent ExFix treatment expressed dissatisfaction with the esthetic aspect of the protruding rods. These rods served as a continual reminder of their traumatic experience and were also a cause of social shame.
Although the initial radiological outcomes were similar in both groups, the ExFix group experienced a subsequent deterioration in alignment, leading to varied radiological outcomes as the study continued, particularly after 1.5 months. Nevertheless, this discrepancy did not reach statistical significance (P = 0.06).
Nevertheless, the functional outcomes were stable throughout the research. Patients in the dorsal distraction plating group experienced a considerable improvement in the ease of completing daily activities compared to other groups.
One patient in the dorsal distraction plating group experienced a fracture in the shaft of their third metacarpal, but declined any more treatment (Table 2, 3, 4) Figs. 10
Analysis
ExFix is a highly effective technique for repairing fractures situated at the far end of the radius. Bridge plating is a novel technique that improves the idea of spanning and stabilizing a reduced and distracting distal radius fracture. The use of this technology offers several potential advantages, including reducing the chances of visible hardware issues, enabling the hardware to stay in place for a longer period of time, and facilitating quick bearing weight on a broken distally radius. Both approaches are highly advantageous for an upper-arm surgeon to possess.
Bridge plating had a decreased incidence of infection in comparison to ExFix. The elevated incidence of infection is unsurprising, as pin tract infections are a well-known drawback of ExFix and a significant factor in the duration of hardware removal. Although there were no notable disparities in the prevalence of complications related to infection, there were discernible variations in the daily activities observed among the two groups.
The examination of our survey unveiled that patients who underwent ExFix encountered various complications.[7] These encompassed issues with routine tasks such as eating, disruptions in sleep, and obstacles in maintaining their employment. Moreover, these patients reported encountering significant social stigma and expressed dissatisfaction with the cosmetic results and overall post-operative outcomes.
In contrast, patients operated with dorsal distraction reported fewer issues. While some challenges were noted, these patients were generally very satisfied with the outcomes of their surgery. The findings suggest that dorsal distraction may offer a more favorable balance between functional recovery and patient satisfaction, highlighting a potential advantage over ExFix. In the long run, however, the functional outcomes of both the techniques were found to be similar[8-10].
Dorsal bridge plating is a viable substitute for ExFix in treating distal radius fractures. The use of dorsal bridge plating demonstrated greater performance in daily activities, despite the fact that the functional and radiological results at 6 months were found to be almost indistinguishable in both groups
Dorsal distraction plating is a reliable alternative to ExFix for managing comminuted intra-articular distal radius fractures. It offers better patient comfort, fewer complications, and improved satisfaction with daily activities and cosmetic outcomes, while maintaining comparable functional and radiological results.
References
- 1.O’Neill TW, Cooper C, Finn JD, Lunt M, Reid DM, Purdie D, et al. Incidence of distal forearm fracture in British men and women. Osteoporos Int 2001;12:555-8. [Google Scholar | PubMed]
- 2.Jupiter JB, Fernandez DL. Comparative classification for fractures of the distal end of the radius. J Hand Surg Am 1997;22:563-71. [Google Scholar | PubMed]
- 3.Rozental TD, Beredjiklian PK. Complications of external fixation of distal radius fractures. J Hand Surg 2009;29:267-72 [Google Scholar | PubMed]
- 4.Wolfe SW, Swigart CR, Grauer J, Slade JF 3rd. Augmented external fixation of distal radius fractures: A comparative study. J Hand Surg 2006;31:543-51. [Google Scholar | PubMed]
- 5.Orbay JL, Fernandez DL. Volar fixed-angle plate fixation for unstable distal radius fractures in the elderly patient. J Hand Surg Am 2002;27:825-832Chung KC, Watt AJ, Kotsis SV, Margaliot Z, Haase SC, Kim HM. Treatment of unstable distal radial fractures with the volar locking plating system. J Bone Joint Surg 2006;88:2687-94. [Google Scholar | PubMed]
- 6.Mehling I, Müller LP, Burkhart KJ. Complications of plating in distal radius fractures. Hand Clin 2009;26:131-42. [Google Scholar | PubMed]
- 7.Orbay JL, Fernandez DL. Volar fixed-angle plate fixation for unstable distal radius fractures in the elderly patient. J Hand Surg Am 2002;27:825-832. [Google Scholar | PubMed]
- 8.Chung KC, Watt AJ, Kotsis SV, Margaliot Z, Haase SC, Kim HM. Treatment of unstable distal radial fractures with the volar locking plating system. J Bone Joint Surg 2006;88:2687-94. [Google Scholar | PubMed]
- 9.Margaliot Z, Chung KC. Outcomes of external fixation versus plate osteosynthesis for unstable distal radius fractures. J Hand Surg 2005;30:1185-99. [Google Scholar | PubMed]
- 10.Wichlas F, Haas NP, Machó D, Disch AC, Tsitsilonis S. Dorsal bridge plating versus external fixation for comminuted intra-articular fractures of the distal radius: A prospective randomized trial. J Hand Surg 2014;39:1254-60. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2025 Limb Reconstruction System for Infected Nonunion: A Retrospective Study
April 1, 2025 Limb Reconstruction System for Infected Nonunion: A Retrospective Study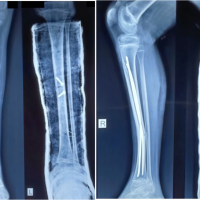 January 10, 2023 Agricultural Rotavator Induced Polytrauma in a 11-years-old Child – A Case Report
January 10, 2023 Agricultural Rotavator Induced Polytrauma in a 11-years-old Child – A Case Report April 10, 2021 External Fixator as a Saviour in the Management of Aneurysmal Bone Cyst with Physeal Extension in Pathological Fracture of the Proximal Femur: A Case Report with a Review of Literature
April 10, 2021 External Fixator as a Saviour in the Management of Aneurysmal Bone Cyst with Physeal Extension in Pathological Fracture of the Proximal Femur: A Case Report with a Review of Literature September 10, 2021 Conversion of Neer Type II Closed Distal Clavicle Fracture to an Open Fracture Following Surgery Delay: A Case Report
September 10, 2021 Conversion of Neer Type II Closed Distal Clavicle Fracture to an Open Fracture Following Surgery Delay: A Case Report