
Structured stretching exercises provide more sustained, long-term pain relief and functional improvement in plantar fasciitis compared to corticosteroid injections. While steroids offer faster short-term symptom control, stretching should be considered the primary conservative treatment, especially for lasting recovery and minimizing recurrence or complications.
Dr. Divya Nand Pandey, Department of Orthopaedics, GSVM Medical College and associated LLR Hospital, Kanpur, Uttar Pradesh, India. E-mail: draanand29@gmail.com
Introduction: Plantar fasciitis is a prevalent cause of heel pain, especially in middle-aged and older adults. This study compares the short-term and long-term effectiveness of plantar fascia stretching exercises versus corticosteroid injections in improving pain and function.
Materials and Methods: This prospective clinical trial included 100 patients randomly assigned to two treatment groups: One undergoing plantar fascia-specific stretching exercises with anti anti-inflammatory medications , contrast bath and shoe insole and the other receiving a single corticosteroid injection (Triamcinolone acetonide 1 mL i.e. , 40 mg with 1 mL 2% lignocaine with 20 gauze needle) on medial to the heel pad on most tender point after local sensitivity followed by anti anti-inflammatory medications , contrast bath and shoe insole .Outcome measures included the visual Visual aAnalogue scale Scale (VAS) and the foot and ankle ability measure (FAAM), recorded at baseline, and at 2, 6, 12, and 16 weeks post-treatment.
Results: While the steroid group showed superior pain relief and functional improvement at 2 and 6 weeks, the stretching group demonstrated significantly better outcomes at 12 and 16 weeks. VAS and FAAM scores favored stretching in long-term analysis (P < 0.0001).
Discussion The mean age was 42.8 ± 3.82 years in the conservative group and 40.5 ± 3.48 years in the steroid group, with 76% aged 30–50 years. Gender distribution was nearly equal, and 14% had bilateral involvement. Most participants (64%) were overweight (body mass index [BMI] 25––30), a known risk factor. VAS scores were similar at baseline (7.24 vs. 7.50; P= 0.2428). The steroid group showed faster pain relief at 2 and 6 weeks (VAS: 4.86 and 2.64 vs. 6.62 and 3.86; P < 0.0001), but the conservative group had better outcomes by 12 and 16 weeks (VAS: 2.65 and 2.26 vs. 2.98 and 3.12; P = 0.0113 and < 0.0001). FAAM scores followed a similar pattern: early Early gains favored steroids (60.13 vs. 54.82 at 2 weeks; P < 0.0001), but long-term improvement was greater in the conservative group (70.13 vs. 63.86 at 16 weeks; P < 0.0001).Thus, while corticosteroids offer quick relief, stretching exercises yield superior long-term outcomes, supporting a combined treatment approach.
Conclusion: Structured stretching offers more durable relief and should be considered a primary intervention in plantar fasciitis.
Keywords Corticosteroid, 2% lignocaine, 20 gauze needle, planter stretching exercise, planter fasciitis, foot and ankle ability measure, Visual Analogue Scale
score.
Plantar fasciitis affects approximately 10% of the population at some point in their lives and is particularly common in individuals aged 40 to –60 [1]. The pathology is characterized by microtears and inflammation at the origin of plantar fascia. While corticosteroid injections offer prompt relief, they may be associated with risks, like such as fascia rupture, tendon rupture, skin depigmentation, and fat pad atrophy, and are often less effective in the long term [2,3]. This study investigates whether a structured stretching protocol offers superior long-term outcomes compared to corticosteroids.
A total number of 106 patients with clinical signs of plantar fasciitis were enrolled, in which 6 patients were lost to follow- up at outpatient Department of Orthopedics of GSVM Medical College and LLR Hospital , Kanpur.
Inclusion criteria- :
Clinically diagnosed 100 patients with age group (20-–70 year) with [1] complain of heel pain worsen at Ffirst step in morning hours and after prolonged duration of sitting for 1 month or more [2] with maximum tenderness at planter fascia attachment (on medial calcaneal tubercle) [3]. willing to participate in study and accept the treatment protocol as per consent.
Exclusion criteria- :[1] Previous surgery of ankle, [2]. Pain with neuropathic symptoms (tarsal tunnel syndromesyn , radiculopathy,, tarsi sinus syndrome) , [3]. with symptom of complex
regional pain syndrome, [4]. Achillis tendon pathology, [5]. Systemic diseases-rheumatoid arthritis, diabetes mellitus, Local /systemic infection, Clotting disorder, peripheral vascular disease, [6]. PregenantPregnant female
Breastfeeded, [7]. Dysfunction of knee, ankle, foot, [8]. Previous injection in lpast 6 months. Participants were randomly assigned in to two groups:
– Group A (n = 50): Received a plantar fascia-specific stretching program (3 times/day for 16 weeks) with anti-inflammatory medications , contrast bath and shoe insole .
– Group B (n = 50): Received a single corticosteroid injection (Triamcinolone acetonide 1 mL i.e., 40 mg with 1 mL 2% lignocaine with 20 gauze needle) on medial to the heel pad on most tender point after local sensitivity and consent. After injection patient asked to rest for 15 min and then allowed to walk and suggested anti- inflammatory medications , contrast bath and shoe insole.
Visual Analogue Scale (VAS) and foot and ankle ability measure (FAAM) scores were recorded at five intervals: Baseline, 2, 6, 12, and 16 weeks. Statistical significance was set at P < 0.05, and data were analyzed using t-tests and repeated measures analysis of variance.
Demographics
The mean age of participants was 41.65 years. The 40–50 year age group had the highest representation (42%). More than 60% were overweight (BMI > 25). Slight right-sided involvement was noted in both groups. (Tables 1, 2, 3 and Fig. 1a, b., c).
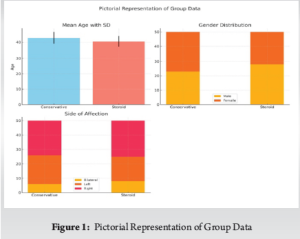
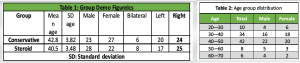
In the present study, the mean age of patients was 42.8 ± 3.82 years in the conservative group and 40.5 ± 3.48 years in the steroid group, with the majority of cases (76%) occurring between 30 and 50 years of age. (Tables 1, and 2 ). This is slightly younger than the populations reported in several Western studies, where the mean age typically ranges from 45 to 50 years. Riddle et al. [7] and Rome et al. [9], for instance, reported peak incidence between 45– and 64 years and a mean age of approximately 46 years, respectively. Regarding gender distribution, our study showed a nearly equal male-to-female ratio (51:49)
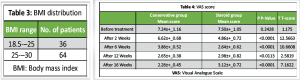
(Fig. 1b), Bilateral involvement was observed in 14% of cases in our study, which is in alignment with prior reports (Fig. 1c). Such as Cardinal et al. [10], who found bilateral symptoms in approximately 10–15% of patients. Laterality also revealed a predominance of right-sided involvement, which is commonly associated with limb dominance (Table- 1). In terms of body mass index (BMI), 64% of our patients fell within the overweight range (BMI 25–30), while 36% were in the normal BMI range (18.5–25) (Table- 3). This distribution is in line with prior studies that highlight overweight and obesity as significant risk factors associated with plantar fasciitis . Riddle et al. [7] reported that a BMI >30 nearly doubled the risk of developing the condition. Similarly, Wearing et al. [8] identified a strong association between elevated BMI and increased plantar pressures. These findings substantiate the mechanical overload hypothesis regarding the pathogenesis of plantar fasciitis and emphasize the significance of weight management in its prevention and therapeutic approach.
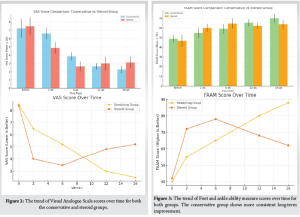
The (VAS) scores serve as a metric for evaluating pain intensity, showed that both the conservative and steroid treatment groups had comparable baseline pain levels before intervention (Table- 4), with mean scores of 7.24 ± 1.16 and 7.50 ± ± 1.05, respectively (P = = 0.2428), indicating no significant initial difference. However, by the 2nd week, the steroid group exhibited a marked reduction in pain, with the VAS score dropping to 4.86 ± 0.72, compared to a more modest reduction to 6.62 ± ± 0.68 in the conservative group (P < 0.0001). This significant early pain relief in the steroid group persisted at 6 weeks, where their VAS score further decreased to 2.64 ± ± 0.62, significantly lower than the conservative group’s score of 3.86 ± ± 0.52 (P < < 0.0001). Interestingly, by the 12th week, this trend began to reverse. Although the steroid group had a VAS score of 2.98 ± ± 0.82, the conservative group showed a slightly better improvement with a score of 2.65 ± ± 0.38 (P = 0.0113). This reversal became more pronounced by the 16th week, as the conservative group’s VAS score continued to decline to 2.26 ± 0.45, indicating better long- term pain relief compared to the steroid group, which had a higher score of 3.12 ± 0.72 (P < 0.0001) (Fig. 2). These results suggest (Fig. 1) that while steroid therapy is highly effective in achieving rapid short-term pain control, conservative treatment provides more sustained pain improvement over time.
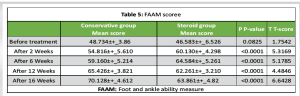
The (FAAM) scores, which assess functional capacity, followed a similar pattern. (Table- 5). Initially, both groups exhibited comparable functional limitations, with the conservative group scoring 48.73 ± ± 3.86 and the steroid group 46.58 ± 6.53 (P ꞊ 0.0825), showing no significant difference before treatment. After 2 weeks, the steroid group experienced a greater improvement in function, with a FAAM score of 60.13 ± 4.30 versus 54.82 ± 5.61 in the conservative group (P < 0.0001). This early advantage continued through the 6th week, where the steroid group scored 64.58 ± 5.26 and the conservative group scored 59.16 ± 5.21 (P < 0.0001). However, at 12 weeks, the conservative group demonstrated superior improvement, with a mean FAAM score of 65.43 ± 3.82 compared to 62.26 ± 3.21 in the steroid group (P < 0.0001). This functional superiority was further confirmed at 16 weeks, where the conservative group achieved a significantly higher score of 70.13 ± 4.61, while the steroid group’s score plateaued at 63.86 ± 4.82 (P < 0.0001) (Fig. 3). These findings indicate that although steroid therapy provides rapid functional recovery in the early phase, conservative treatment ensures better long-term outcomes in terms of both functional ability and pain relief (Fig. 2).
In summary, steroid injections offer rapid and effective short-term improvements in pain and functional status, making them valuable for acute management. However, conservative treatment methods– likely involving physiotherapy, exercise, and lifestyle modifications– demonstrate superior long-term benefits. Thus, an integrated treatment strategy that combines the early benefits of steroid therapy with the sustained gains of conservative management may provide the most comprehensive and lasting outcomes for patients.
The findings from our study, which indicate that steroid injections provide prompt alleviation of pain and significant functional enhancement in the short term, while conservative treatments yield superior long-term outcomes, are consistent with existing literature on the management of plantar fasciitis and similar musculoskeletal conditions.
In a randomized clinical trial comparing dry needling and steroid injections for plantar fasciitis, steroid injections provided significant pain relief at three weeks post-treatment (VAS score: 0.32 ± 0.71) compared to dry needling (VAS score: 3.47 ± 1.32; P < 0.001). However, at the 1-year follow-up, patients treated with dry needling reported lower VAS scores (0.69 ± 0.93) than those who received steroid injections (2.09 ± 1.58; P = 0.004), suggesting better long-term pain control with dry needling [11].
Similarly, a study comparing conservative management and steroid injections found that while the steroid group experienced a rapid decrease in VAS scores within the first 2
weeks, the conservative group showed a gradual decline over 8 weeks. By the 8th week, there was no appreciable difference in VAS scores between the two groups. indicating that conservative treatments can be as effective as steroid injections in the longer term [12].
In terms of functional outcomes assessed by the (FAAM), a study juxtaposing platelet-rich plasma (PRP) injections with corticosteroid interventions revealed significant insights that the steroid group showed significant improvement in FAAM scores up to 12 weeks. However, at 24 weeks, the PRP group had higher FAAM scores (84.2) compared to the steroid group (68.3), indicating better long-term functional outcomes with PRP [12].
Another study observed that while the steroid group demonstrated significant functional improvement up to 12 weeks, there was a decline in FAAM scores at 24 weeks. In contrast, the PRP group showed continuous improvement in FAAM scores up to 24 weeks, further supporting the notion that conservative or alternative treatments may offer better long-term functional benefits
The study’s strengths include its prospective design and objective scoring. However, limitations include a relatively short follow-up period and absence of a placebo control group.
These studies emphasizing that while steroid injections may offer prompt alleviation of pain and enhance functionality in the short term, conservative therapies tend to provide more enduring benefits over an extended period. Therefore, a treatment strategy that combines the immediate effects of steroid injections with the long-term advantages of conservative therapies could be the most effective approach for managing conditions, such as plantar fasciitis.
Stretching exercises engender more enduring enhancements in the management of plantar fasciitis compared to corticosteroid injections. They ought to be advocated as the primary conservative intervention, particularly for long-term alleviation.
Combine early corticosteroid intervention (if deemed necessary) with a sustained regimen of stretching exercises to achieve optimal and enduring therapeutic outcomes in the management of plantar fasciitis.
References
- 1.Buchbinder R. Clinical practice. Plantar fasciitis. N Engl J Med 2004;350:2159-66. [Google Scholar | PubMed]
- 2.Crawford F, Thomson C. Interventions for treating plantar heel pain. Cochrane Database Syst Rev 2003;3:CD000416. [Google Scholar | PubMed]
- 3.Tsai WC, Wang CL, Tang FT, Hsu TC, Hsu KH, Wong MK. Treatment of proximal plantar fasciitis with ultrasound-guided steroid injection. Arch Phys Med Rehabil 2000;81:1416-21. [Google Scholar | PubMed]
- 4.Goff JD, Crawford R. Diagnosis and treatment of plantar fasciitis. Am Fam Physician 2011;84:676-82. [Google Scholar | PubMed]
- 5.Roxas M. Plantar fasciitis: Diagnosis and therapeutic considerations. Altern Med Rev 2005;10:83-93. [Google Scholar | PubMed]
- 6.DiGiovanni BF, Nawoczenski DA, Lintal ME, Moore EA, Murray JC, Wilding GE, et al. Tissue-specific plantar fasciastretching exercise enhances outcomes in patients with chronic heel pain. A prospective, randomized study. J Bone Joint Surg Am 2003;85:1270-7. [Google Scholar | PubMed]
- 7.Riddle DL, Pulisic M, Pidcoe P, Johnson RE. Risk factors for plantar fasciitis: A matched case-control study. J Bone Joint Surg Am 2003;85:872-7. [Google Scholar | PubMed]
- 8.Wearing SC, Smeathers JE, Urry SR, Hennig EM, Hills AP. The pathomechanics of plantar fasciitis. Sports Med 2006;36:585-611. [Google Scholar | PubMed]
- 9.Rome K, Howe T, Haslock I. Risk factors associated with the development of plantar heel pain in athletes. Foot 2001;11:119-25. [Google Scholar | PubMed]
- 10.Cardinal M, Chatterjee A, Rhoades D. Clinical outcome of bilateral plantar fasciitis. Foot Ankle Int 1997;18:567-72. [Google Scholar | PubMed]
- 11.Mahindra P, Singh D, Kooner S. Comparison of corticosteroid injection and dry needling in plantar fasciitis: A randomized trial. J Foot Ankle Surg 2020;59:455-60. [Google Scholar | PubMed]
- 12.Joshi A. Comparative study of PRP versus corticosteroids in plantar fasciitis. Orthop J 2018;10:211-7. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2025 Therapeutic Effect of Intralesional Corticosteroids in Comparison with Multiple Puncture Technique in Treatment of Bilateral Plantar Fasciitis
December 1, 2025 Therapeutic Effect of Intralesional Corticosteroids in Comparison with Multiple Puncture Technique in Treatment of Bilateral Plantar Fasciitis June 10, 2024 Osteonecrosis of the Humeral Head 3 Years Following Fracture Fixation of a 4-Part Proximal Humerus Fracture: A Case Report
June 10, 2024 Osteonecrosis of the Humeral Head 3 Years Following Fracture Fixation of a 4-Part Proximal Humerus Fracture: A Case Report November 23, 2017 Arthroscopic Fixation of Tibial Spine Avulsion in Skeletally Immature: The Technique
November 23, 2017 Arthroscopic Fixation of Tibial Spine Avulsion in Skeletally Immature: The Technique May 1, 2025 Short-Segment Fixation in the Management of Thoracolumbar Burst Fractures – A Meta -analysis
May 1, 2025 Short-Segment Fixation in the Management of Thoracolumbar Burst Fractures – A Meta -analysis