
The article’s learning point is that orthopedic surgeons must consider hip dysplasia in their differential diagnosis when treating Perthes-like lesions in pediatric patients.
Ariel D Dávila-Parrilla, Department of Orthopaedic Surgery, University of Puerto Rico, Medical Sciences Campus, San Juan, Puerto Rico, 00926, USA. E-mail: ariel.davila@upr.edu
Introduction: Osteochondritis dissecans (OCD) of the femoral head accounts for approximately 2% of all OCD cases. Most of the OCD lesions affecting the femoral head are secondary to pathologies concerning the femoral component of the hip joint, such as Legg-Calvé-Perthes (LCP) disease. Although there are reports of OCD secondary to hip dysplasia, to our knowledge, there is no report of bilateral OCD lesions being treated successfully with bilateral triple pelvic osteotomies (PAO) in a pediatric patient.
Case Report: In this report, we present the case of an 8-year-old Hispanic male who presented with bilateral hip pain unresponsive to conservative treatment and initially managed with the presumptive diagnosis of LCP disease. Due to his persistent hip pain and no improvement on follow-up X-rays and magnetic resonance imaging (MRI), the patient was referred to our hip preservation clinic for further work-up and management recommendations. MRI revealed bilateral OCD lesions of the femoral head secondary to developmental hip dysplasia. The patient underwent bilateral triple PAO for correction of the patient’s bilateral hip dysplasia, which resulted in the proper resolution of the femoral head lesions on imaging and eventually resolved the patient’s hip pain.
Conclusion: This report aims to recognize the association between untreated developmental hip dysplasia and femoral head Perthes-like lesions in the pediatric population. Orthopedic surgeons must consider developmental hip dysplasia when determining the etiology of Perthes-like lesions in pediatric patients.
Keywords: Case report, developmental dysplasia of the hip, femoral head lesions, osteochondral defects, Legg-Calvé-Perthes disease, pelvic osteotomies.
Developmental dysplasia of the hip (DDH) is the most common abnormality in skeletal development encountered in the pediatric population [1]. The prevalence of DDH among infants is approximately one in 100 and is on an upward trend [2]. The hallmark of this disorder is hip instability that arises secondary to improper congruence and constraint between the femoral head and acetabulum, with painful symptoms presenting after years of damage potentiated by altered biomechanics [3]. In addition, DDH can affect femoral head development due to the altered microenvironment produced at the hip joint [1]. However, the association between DDH and other pathologies that lead to aspherical lesions of the femoral head, such as Legg-Calvé-Perthes (LCP) disease and osteochondritis dissecans (OCD), is poorly understood. OCD is a condition that affects the articular surface of a joint and is characterized by the separation of an osteochondral fragment. Still, it is rarely confined to the hip joint [4]. While generally considered an idiopathic phenomenon, femoral head OCD can present as a complication of LCP disease [4-7]. Although its association with LCP is well documented, to our knowledge, only one case report in the literature presents an association between hip dysplasia and OCD [8]. The goal of this report is to emphasize the need to rule out DDH in pediatric patients presenting with Perthes-like lesions on imaging. To our knowledge, this is the first documented case of bilateral OCD of the femoral head secondary to DDH reported in the literature.
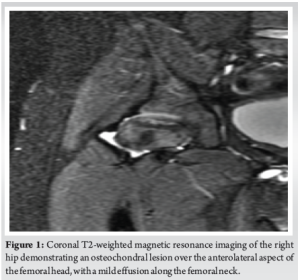
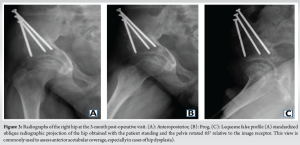
An 8-year-old Hispanic male with no significant medical history presented with bilateral hip pain of eight out of ten on the visual analog scale. He had been followed at a pediatric orthopedic clinic for nearly a year for magnetic resonance imaging (MRI) findings suggestive of bilateral LCP disease at the early fragmentation stage. Lesions were somewhat symmetrical, so a rule out of Meyer’s dysplasia and genetic counseling was done accordingly. Imaging showed 10–15% non-enhancement in the left hip and 10% in the right hip, with more severe avascular necrosis on the right. Scant effusions were noted, without signs of arthrosis or collapse. Given his age and benign diffusion-weighted MRI findings, he was managed conservatively with non-steroidal anti-inflammatory drugs, activity modification, and rest for over a year. Due to persistent pain and unchanged imaging findings, he was referred to our Hip Preservation Clinic. On examination, a functional waddling gait was noted. Bilateral hip flexion was 0–100°, with pain on pure flexion. Internal rotation with flexed hips measured 15° with pain, and external rotation was 40° bilaterally. Anterior impingement and apprehension tests were positive bilaterally. A mucopolysaccharidosis and Sickle Cell panel was ordered and returned negative. Given the benign clinical picture, conservative management continued, including close observation and a 2-month course of physical therapy. At a 4-month follow-up, the patient reported no improvement in pain, and his physical exam remained unchanged. Repeat MRI revealed an under-covered femoral head with a chondral defect partially covered by functional cartilage (Kerboul Grade II) (Fig. 1). A full radiographic workup showed findings consistent with borderline hip dysplasia (Fig. 2), prompting the recommendation for bilateral triple pelvic osteotomies (PAO).

The triple pelvic osteotomy is a procedure where the ischium, superior pubic ramus, and the ilium superior to the acetabulum are divided to allow repositioning of the acetabulum to achieve a concentric reduction of the dysplastic hip (15864035). It is typically performed in older children or younger adolescents with open triradiate cartilage and is indicated for the treatment of hip dysplasia, acetabular dysplasia, and LCP.
After obtaining parental consent, a right-sided triple pelvic osteotomy was performed 6 months after initial evaluation. The right hip had a full, painless passive range of motion 3 months post-operatively. Radiographs showed a well-healing osteotomy with abundant callus (Fig. 3). At 1-year post-operative, the patient remained pain-free on the right, with radiographs demonstrating a healed osteotomy and re-ossification of the femoral head. With improved sphericity and acetabular coverage, the femoroacetabular relationship is more adequate, and his waddle gait almost disappeared completely. However, he continued to experience activity-related pain in the left hip, particularly with deep flexion. At that time, a left-sided triple pelvic osteotomy was scheduled along with the removal of hardware from the right hip.
The left-sided procedure followed a similar course. At 1-year follow-up, the patient had full, painless bilateral hip motion. By 2 years post-operatively, final radiographs showed completely healed bilateral osteotomies and re-ossified femoral heads (Fig. 4).

Our case contributes to the limited literature describing an association between hip OCD and DDH. This case is particularly novel due to the bilateral presentation and the patient’s normal femoral neck-shaft angle, distinguishing it from previously reported cases. The most comparable case involved an early-adolescent boy with a unilateral OCD lesion of the left femoral head associated with acetabular dysplasia and coxa valga [8]. The diagnostic challenge related to our case, which included ruling out bilateral LCP and identifying borderline dysplasia, allows us to argue the importance of considering developmental hip dysplasia in the setting of Perthes-like lesions on imaging. Most OCD lesions of the femoral head occur as complications of LCP disease [4,5,9]. LCP is characterized by avascular necrosis of the femoral head, leading to subchondral bone resorption and potential detachment of osteochondral fragments [10]. These changes are often subtle or delayed on radiographs, making MRI the preferred imaging modality to differentiate Perthes-like lesions. For instance, in avascular necrosis due to LCP, the overlying cartilage typically remains intact, whereas it is often disrupted in OCD [11,12]. Although MRI is not essential for diagnosing DDH, it plays a critical role in evaluating OCD, particularly in assessing lesion stability, which directly influences the choice between non-operative and surgical treatment. The pathogenesis of femoral head OCD remains debated, but the most widely accepted theory involves repetitive microtrauma, which is amplified in dysplastic hip joints [4,13]. DDH is commonly associated with increased femoral anteversion and coxa valga, which alter proximal femoral anatomy without directly affecting the femoral head [14]. Taking into consideration the recent literature, DDH may also impact femoral head anatomy through an association with OCD, yet further investigations are warranted to uncover whether the association is true. With this case, we hope to provide evidence that OCD secondary to DDH follows a different pathophysiological mechanism from that of OCD secondary to LCP and, thus, warrants a different surgical treatment approach. In cases where OCD of the femoral head occurs secondary to LCP, surgical options for symptomatic lesions include osteochondral autograft transfer, fresh osteochondral allograft, arthroscopic fragment resection, and surgical hip dislocation with ORIF [5,6,15]. However, when OCD occurs in the context of DDH, management strategies differ. To address the dysplasia, the surgeon must surgically fix either the femoral or acetabular side to offload the diseased joint and achieve a concentric hip. In a previously reported case, OCD associated with hip dysplasia was addressed using an isolated proximal femoral varus osteotomy to correct coxa valga [8]. To our knowledge, this is the first reported case of bilateral femoral head OCD secondary to DDH treated successfully with bilateral triple PAO. The triple pelvic osteotomy is indicated in skeletally immature patients with open triradiate cartilage and is a well-established treatment for both DDH and LCP [16,17]. Compared to other PAO, the advantages of this procedure are increased coverage of the femoral head by articular cartilage of the acetabulum, better hip joint stability for earlier weight bearing, and no need for spica cast immobilization (15864035) [18]. Other approaches, such as the Salter osteotomy and femoral varus osteotomies, are at increased risk of excessive varus deformity, which may increase pain post-operatively secondary to altered gait biomechanics [19]. In our case, the early weight-bearing (achieved by 10 weeks post-operatively), patient demographics, radiographic assessment of the femoral head lesions, and bilateral nature of the disease led to our decision to pursue triple PAO over other surgical treatment options.
Perthes-like lesions of the femoral head are often associated with proximal femoral pathologies, such as LCP. We describe a rare case of an 8-year-old boy with bilateral femoral head OCD lesions successfully treated with bilateral triple PAO. Although this association is infrequently reported, orthopedic surgeons should consider DDH in diagnosing aspherical femoral head lesions in pediatric patients.
Orthopedic specialists should consider developmental hip dysplasia as a potential treatable cause when evaluating femoral head osteochondral lesions in the pediatric population.
References
- 1.Sioutis S, Kolovos S, Papakonstantinou ME, Reppas L, Koulalis D, Mavrogenis AF. Developmental dysplasia of the hip: A review. J Long Term Eff Med Implants 2022;32:39-56. [Google Scholar | PubMed]
- 2.Tao Z, Wang J, Li Y, Zhou Y, Yan X, Yang J, et al. Prevalence of developmental dysplasia of the hip (DDH) in infants: A systematic review and meta-analysis. BMJ Paediatr Open 2023;7:e002080. [Google Scholar | PubMed]
- 3.Ganz R, Leunig M, Leunig-Ganz K, Harris WH. The etiology of osteoarthritis of the hip: An integrated mechanical concept. Clin Orthop Relat Res 2008;466:264-72. [Google Scholar | PubMed]
- 4.Chau MM, Klimstra MA, Wise KL, Ellermann JM, Tóth F, Carlson CS, et al. Osteochondritis dissecans: Current understanding of epidemiology, etiology, management, and outcomes. J Bone Joint Surg Am 2021;103:1132-51. [Google Scholar | PubMed]
- 5.Lamplot JD, Schoenecker PL, Pascual-Garrido C, Nepple JJ, Clohisy JC. Open reduction and internal fixation for the treatment of symptomatic osteochondritis dissecans of the femoral head in patients with sequelae of legg-calve-perthes disease. J Pediatr Orthop 2020;40:120-8. [Google Scholar | PubMed]
- 6.De Angeli LR, Serafim BL, Cordeiro FG, Bessa FS, Maranho DA. Osteochondritis dissecans of the hip in legg-calve-perthes disease: Case report and review. Acta Ortop Bras 2024;32:e277177. [Google Scholar | PubMed]
- 7.Lee MC, Kelly DM, Sucato DJ, Herring JA. Familial bilateral osteochondritis dissecans of the femoral head. A case series. J Bone Joint Surg Am 2009;91:2700-7. [Google Scholar | PubMed]
- 8.Hernandez SG, McQueen RG, Erickson JB. Femoral head osteochondritis dissecans in a child. BMJ Case Rep 2023;16:e253375. [Google Scholar | PubMed]
- 9.Siebenrock KA, Powell JN, Ganz R. Osteochondritis dissecans of the femoral head. Hip Int 2010;20:489-96. [Google Scholar | PubMed]
- 10.Ibrahim T, Little DG. The pathogenesis and treatment of legg-calve-perthes disease. JBJS Rev 2016;4:e4. [Google Scholar | PubMed]
- 11.Edwards DJ, Lomas D, Villar RN. Diagnosis of the painful hip by magnetic resonance imaging and arthroscopy. J Bone Joint Surg Br 1995;77:374-6. [Google Scholar | PubMed]
- 12.Lee JE, Ryu KN, Park JS, Cho YJ, Yoon SH, Park SY, et al. Osteochondral lesion of the bilateral femoral heads in a young athletic patient. Korean J Radiol 2014;15:792-6. [Google Scholar | PubMed]
- 13.Wells J, Nepple JJ, Crook K, Ross JR, Bedi A, Schoenecker P, et al. Femoral morphology in the dysplastic hip: Three-dimensional characterizations with CT. Clin Orthop Relat Res 2017;475:1045-54. [Google Scholar | PubMed]
- 14.Sankar WN, Neubuerger CO, Moseley CF. Femoral anteversion in developmental dysplasia of the hip. J Pediatr Orthop 2009;29:885-8. [Google Scholar | PubMed]
- 15.Khanna V, Tushinski DM, Drexler M, Backstein DB, Gross AE, Safir OA, et al. Cartilage restoration of the hip using fresh osteochondral allograft: Resurfacing the potholes. Bone Joint J 2014;96-B:11-6. [Google Scholar | PubMed]
- 16.Conroy E, Sheehan E, O’ Connor P, Connolly P, McCormack D. Triple pelvic osteotomy in legg-calve-perthes disease using a single anterolateral incision: A 4-year review. J Pediatr Orthop B 2010;19:323-6. [Google Scholar | PubMed]
- 17.Vukasinovic Z, Spasovski D, Vucetic C, Cobeljic G, Zivkovic Z, Matanovic D. Triple pelvic osteotomy in the treatment of legg-calve-perthes disease. Int Orthop 2009;33:1377-83. [Google Scholar | PubMed]
- 18.Kamath AF. Bernese periacetabular osteotomy for hip dysplasia: Surgical technique and indications. World J Orthop 2016;7:280-6. [Google Scholar | PubMed]
- 19.Wenger DR, Pandya NK. Advanced containment methods for the treatment of perthes disease: Salter plus varus osteotomy and triple pelvic osteotomy. J Pediatr Orthop 2011;31:S198-205. [Google Scholar | PubMed]
Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Intraoperative Diagnosis and Management of Testicular Dislocation During Pelvic Fracture Fixation: A Report of Two Cases and Literature Review
February 1, 2026 Intraoperative Diagnosis and Management of Testicular Dislocation During Pelvic Fracture Fixation: A Report of Two Cases and Literature Review February 1, 2026 Symptomatic Ventromedial Scapular Osteochondroma Presenting with Restriction of Shoulder Movements: A Case Report
February 1, 2026 Symptomatic Ventromedial Scapular Osteochondroma Presenting with Restriction of Shoulder Movements: A Case Report February 1, 2026 A Novel Technique of Rerouting Semitendinosus Graft for Medial Collateral Ligament and Medial Patellofemoral Ligament Reconstruction – In a Polytrauma Patient with Multiligament Injury: Kakran et al. Technique
February 1, 2026 A Novel Technique of Rerouting Semitendinosus Graft for Medial Collateral Ligament and Medial Patellofemoral Ligament Reconstruction – In a Polytrauma Patient with Multiligament Injury: Kakran et al. Technique January 1, 2026 Primary Synovial Chondromatosis of the Elbow Joint Presenting with Ulnar Nerve Compression and Restricted Range of Motion: A Case Report
January 1, 2026 Primary Synovial Chondromatosis of the Elbow Joint Presenting with Ulnar Nerve Compression and Restricted Range of Motion: A Case Report