
Preserving the blood supply and minimizing soft-tissue damage is crucial when treating segmental femur fractures.
Dr. Sankalp Lal, Department of Orthopaedics, Sports Injury Centre, Vardhman Mahavir Medical College and Safdarjung Hospital, New Delhi, India. E-mail: sankalp26@live.com
Introduction: Segmental femur fractures, an uncommon injury pattern, are usually caused by high-energy trauma such as road traffic accidents. Despite their complexity, early intervention is essential for maximising recovery and reducing complications.
Case Report: A 34-year-old male presented with multiple fractures, including a triple-segmental shaft femur fracture, following a high-energy road traffic accident. An intramedullary nail was used for closed reduction and internal fixation of the femur fracture, which provided stable fixation while preserving the blood supply and minimising soft-tissue damage.
Conclusion: When treating complicated femur fractures, intramedullary nailing should be preferred because it minimises soft-tissue damage while offering stable fixation. It promotes early mobilisation and optimal healing, even with multiple fracture segments.
Keywords: Triple-segmental, shaft femur fracture, intramedullary nailing, road traffic accident, case report.
Femur fractures are among the most common long bone injuries treated by orthopaedic surgeons, frequently brought on by high-energy trauma from road traffic accidents, falls from height, or industrial accidents [1]. Segmental femur fractures, which comprise at least two separate fracture lines, are comparatively uncommon within this category and make up a small portion of all femoral fractures [2]. The discontinuity of the fracture segments, the possibility of devascularization of the fracture segments, and the difficulty of obtaining stable fixation make these injuries extremely difficult to manage. A rare injury pattern is the triple-segmental shaft femur fracture, in which the femur is broken into five distinct segments. Treatment options include intramedullary nailing, plating, external fixation, or a combination [3]. Intramedullary nailing is the preferred fixation method for segmental femur fractures because of its low soft-tissue disruption, excellent biomechanical stability and high union rates [4]. Multiple fracture segments, however, add to the procedure’s technical difficulty. The treatment is even more complicated when numerous fractures accompany such an injury, as was the case in this instance. We report the case of a 34-year-old man who suffered a triple-segmental shaft femur fracture after a high-energy road traffic accident. The patient underwent closed reduction and internal fixation (CRIF) with an intramedullary nail.
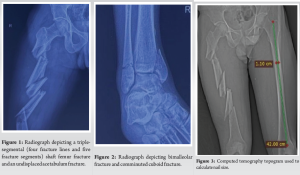
A 34-year-old male was brought to our emergency department following a high-energy road traffic accident. The patient’s complaints included severe pain, swelling, and an inability to bear weight on his left lower limb. Upon clinical examination, the left thigh had considerable soft tissue swelling and localised tenderness. Despite having stable vital signs, he appeared distressed due to the pain and swelling. X-rays of the left thigh revealed a triple-segmental shaft femur fracture (Fig. 1). This is an uncommon pattern–the femur is divided into five segments. Additional imaging revealed a bimalleolar fracture, a comminuted cuboid fracture, an undisplaced acetabulum fracture, and an undisplaced patella fracture (Fig. 2).
The number of fracture segments and the resulting soft-tissue damage complicated the femur fracture. The other fractures found in the imaging studies were comparatively more straightforward despite being significant.
In this case, a computed tomography (CT) topogram/scout view/scanogram was utilised to accurately assess the femoral anatomy and determine the appropriate size for the intramedullary nail [5-7]. We measured the diameter and length of the femoral canal, ensuring precise selection of the nail size (Fig. 3). A 3D CT reconstruction was also done to aid surgical planning (Fig. 4 and 5).

It was decided to use an intramedullary nail for closed reduction and internal fixation (CRIF) of the triple-segmental shaft femur fracture. Fixation of the bimalleolar fracture was done with antiglide plating and cannulated cancellous screws. The other fractures were managed conservatively.
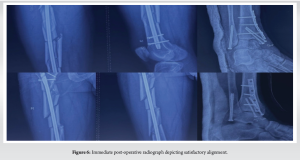
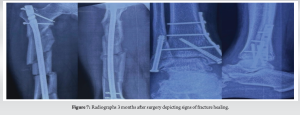
The patient had an uneventful post-operative course. An immediate post-operative radiograph depicted satisfactory alignment (Fig. 6). He was advised of early mobilisation with weight-bearing limitations . Radiographs 3 months after surgery showed signs of fracture healing and satisfactory alignment (Fig. 7). The patient continued physiotherapy to regain range of motion and strength in the injured limb. Radiographic evaluation 1 year after surgery confirmed complete fracture union (Fig. 8). The other fractures–the patella, acetabulum, cuboid, and bimalleolar–had also appropriately healed. The patient returned to his pre-injury activity level without limitations and reported no persistent pain.

Segmental femur fractures with four fracture lines and five fracture segments have been reported twice in the literature [8,9]. However, they included neck femur fractures or distal femur fractures. This case illustrates an exceedingly rare injury pattern: A triple-segmental shaft femur fracture, which has never been documented in the literature. The main challenges are ensuring stable fracture fixation, maintaining the blood supply to the fracture segments, and shielding the surrounding soft tissues from additional harm during fixation. In addition, when treating such complex femur fractures, complications like non-union, infection, or malunion are frequent. Intramedullary nailing was selected as the fixation technique because it minimises tissue disruption while offering stable fixation [10]. A speedier recovery was made possible by early mobilisation and rehabilitation. Furthermore, the patient’s concomitant fractures, including a bimalleolar fracture, were successfully managed, highlighting the necessity of an all-encompassing treatment plan. This case emphasises the significance of a customised approach in managing polytrauma patients.
The rarity of triple-segmental shaft femur fractures is highlighted in this case report, along with the significance of early surgical intervention and close follow-up. This case provides important insights into treating complex injuries and adds to the small data pool on such fractures.
Timely intervention and a personalised treatment plan are key to successful outcomes in complex fractures.
References
- 1. De Moraes FB, Da Silva LL, Ferreira FV, Ferro AM, Da Rocha VL, Teixeira KI. Epidemiological and radiological evaluation of femoral shaft fractures: Study of 200 cases. Rev Bras Ortop 2009;44:199-203. [Google Scholar] [PubMed]
- 2. Galanis A, Vavourakis M, Karampitianis S, Karampinas P, Sakellariou E, Tsalimas G, et al. Double segmental femoral fracture: A rare injury following high-energy trauma. J Med Cases 2024;15:297-303. [Google Scholar] [PubMed]
- 3. Adeel M, Zardad S, Jadoon SM, Younas M, Shah U. Outcome of open interlocking nailing in closed fracture shaft of femur. J Ayub Med Coll Abbottabad 2020;32:546-50. [Google Scholar] [PubMed]
- 4. Winquist RA, Hansen ST. Segmental fractures of the femur treated by closed intramedullary nailing. J Bone Joint Surg Am 1978;60:934-9. [Google Scholar] [PubMed]
- 5. Eurich J, Dwyer EP, Gibbs S, Erdman MK. Achieving limb-length equality in femoral shaft fractures. J Orthop Trauma 2024;38:S9-10. [Google Scholar] [PubMed]
- 6. Vaidya R, Anderson B, Elbanna A, Colen R, Hoard D, Sethi A. CT scanogram for limb length discrepancy in comminuted femoral shaft fractures following IM nailing. Injury 2012;43:1176-81. [Google Scholar] [PubMed]
- 7. Gheraibeh P, Vaidya R, Hudson I, Meehan R, Tonnos F, Sethi A. Minimizing leg length discrepancy after intramedullary nailing of comminuted femoral shaft fractures: A quality improvement initiative using the scout computed tomography scanogram. J Orthop Trauma 2018;32:256-62. [Google Scholar] [PubMed]
- 8. Kim BS, Cho JW, Yeo DH, Oh JK. Surgical treatment of ipsilateral multi-level femoral fracture treated using antegrade intramedullary nail. J Trauma Injury 2018;31:96-102. [Google Scholar] [PubMed]
- 9. Sessa P, Galluzzo M, Leone E, Antonio Maria S, Giannicola G. Multiple fractures of the femur: Case report, literature review, and proposal for a shared algorithm of treatment. SAGE Open Med Case Rep 2024;12. [Google Scholar] [PubMed]
- 10. Howe TS. Double level fractures of the femur treated with closed intramedullary nailing. Ann Acad Med Singap 1998;27:188-91. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Salvage of a Broken Magnetic Tibia Nail with Plate Fixation Without Nail Removal: A Case Report
March 1, 2026 Salvage of a Broken Magnetic Tibia Nail with Plate Fixation Without Nail Removal: A Case Report March 1, 2026 Clavicle Fracture Non-Union in a 3-Year-Old Child: A Case Report and Literature Review
March 1, 2026 Clavicle Fracture Non-Union in a 3-Year-Old Child: A Case Report and Literature Review March 1, 2026 Single Peg Patellar Component Fracture in Total Knee Replacement: A Case Report
March 1, 2026 Single Peg Patellar Component Fracture in Total Knee Replacement: A Case Report March 1, 2026 Management of a Missed Iatrogenic Fracture Neck of Femur in an Operated Case of Fracture Shaft Femur- Case Report
March 1, 2026 Management of a Missed Iatrogenic Fracture Neck of Femur in an Operated Case of Fracture Shaft Femur- Case Report