
Concomitant neck of femur and greater trochanter fracture can be effectively managed with multiple cannulated screws with a favorable outcome.
Dr. Pratik Kotangale, Department of Orthopaedics, Government Medical College, Nagpur, Maharashtra, India. E-mail: pratik.kotangle@gmail.com
Introduction: Concomitant injury to the femoral neck and trochanteric area is very rare in younger patients; these are usually the result of a high-energy trauma, such as a motor vehicle accident or a fall from height. It is recommended to reduce and fix the fractures as early as possible to avoid complications, including avascular necrosis (AVN) of the femoral head, impaired functioning of the hip abductor muscles, malunion, and non-union.
Case Report: We report an extremely rare case of a 23-year-old male patient who sustained concomitant neck and greater trochanter (GT) of femur fracture, which was operated with closed reduction and internal fixation with percutaneous partially threaded cannulated cancellous (CC) screws.
Conclusion: Concomitant neck of femur and GT fracture in young adults is a rare and difficult fracture pattern presenting challenges as to optimum modality of fixation. Although mostly dynamic hip screw (DHS) has been used to treat this fracture, it can also be managed by multiple CC screws, avoiding the risk of lateral wall instability inherent with DHS fixation in this fracture pattern.
Keywords: Concomitant neck of femur and greater trochanter, multiple cannulated cancellous screws, non-union, avascular necrosis of the femoral head.
Fractures of the femoral neck are one of the most common orthopedic injuries, predominantly seen in elderly patients. In younger patients, these are usually the result of a high-energy trauma, such as a motor vehicle accident or fall from height, and there may be associated injuries, such as ipsilateral femoral shaft fractures, distal radius fractures, and proximal humerus fractures [1]. Concomitant injury to the femoral neck and trochanteric area is very rare and has mostly been reported in the elderly [2]. Unlike elderly patients, where arthroplasty is the treatment of choice, in younger patients, it is recommended to reduce and fix the fractures as early as possible. Concomitant neck of femur and greater trochanter (GT) carry a substantial risk of complications, including avascular necrosis (AVN) of the femoral head, impaired functioning of the hip abductor muscles, and malunion and non-union [3]. We, hereby, report an extremely rare case of a 23-year-old male patient who sustained concomitant neck and GT of femur fracture, which was operated with closed reduction and internal fixation with percutaneous partially threaded cannulated cancellous (CC) screws.
A 23-year-old male was admitted to our emergency department 2 h following a road traffic accident, sustaining injury to the right hip. On presentation, patient had pain in the right hip with inability to bear weight on the same side. Radiographs revealed the presence of neck of femur fracture accompanied with a fracture of the GT (Fig. 1).
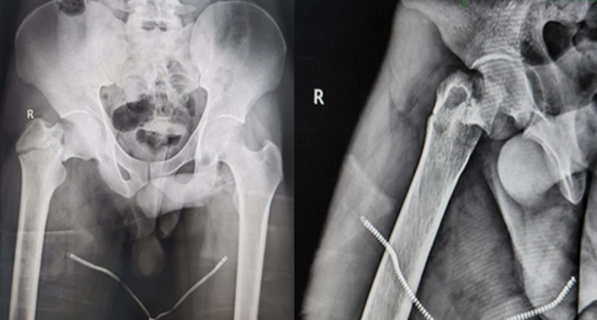
Figure 1: Pre-operative anteroposterior and lateral radiographs
(Pre- and post-operative computed tomography was not advised as the fracture pattern was adequately distinguished in X-rays and to avoid excessive radiation exposure). The patient was posted for surgery within 48 h of trauma. With the patient on the fracture table, gentle traction was given and a satisfactory closed reduction could be achieved. After confirming reduction under C-arm, we proceeded for percutaneous partially threaded CC screw fixation (Fig. 2).
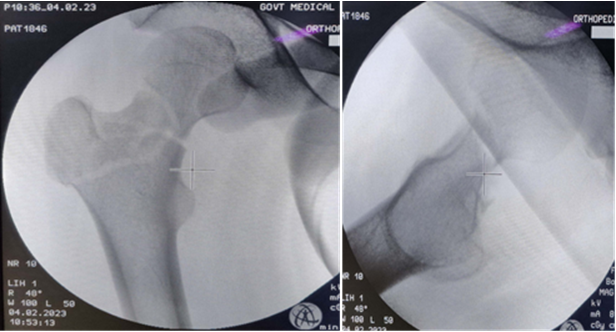
Figure 2: – C- arm images post- reduction.
Initially, two parallel guide wires for 6.5 mm CC screws were passed to stabilize the femoral neck fracture. This was followed by one guide wire fixing the GT to the femoral head and another guide wire from the tip of GT directed toward the lesser trochanter. The femoral neck screws were passed first and compression was achieved across the fracture site. Then, the screws fixing the GT fragment were passed. Care was taken to ensure that all the screw threads crossed the fracture lines. Due to the complexity of the fracture pattern, we delayed post-operative mobilization. Non-weight-bearing walking with axillary crutches was started at 6 weeks, progressing to full weight-bearing once radiological union at the fracture site was confirmed at 12 weeks postoperatively (Fig. 3 and 4).
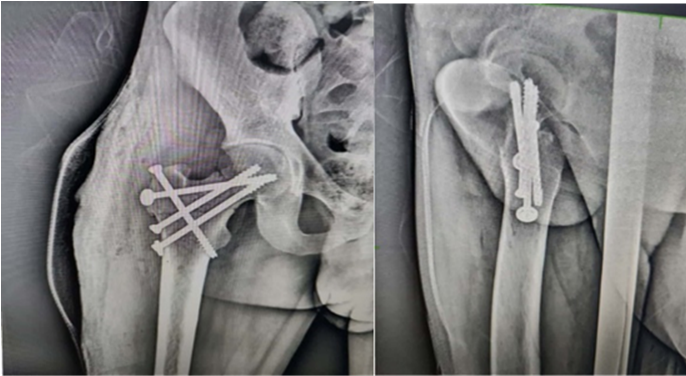
Figure 3: – Immediate post-operative X-rays.

Figure 4- : 18 months post post-operative anteroposterior AP and lateral X-rays.
At 4 months post-operative, the patient had achieved an excellent, painless range of motion of the affected hip, allowing him to resume his job. At the latest follow-up at 18 months, there was no radiological evidence of AVN (Fig. 5).

Figure 5- : Clinical photograph of the patient at four4-month follow-up showing the range of motion.
Magnetic resonance imaging (MRI) was not done for this patient as the patient had painless and full hip range of motion and could carry out his daily activities without any issues. Hence, we opted against conducting an MRI, given the absence of both clinical and radiological evidence of involvement.
Concomitant fracture of the neck of the femur and GT is extremely rare and has mostly been reported in the elderly, with only a few case reports in young patients [2,4,5,6]. At present, there is no classification for combined fractures involving both the neck and trochanter of the femur and there is a dearth of literature regarding guidelines for treatment of such fractures. Concomitant neck and trochanter fracture is inherently unstable due to multiple fracture fragments, rotational instability of the neck fragment, and the possibility of concealed lateral wall fracture [7]. In the elderly, these have been treated by various methods, including fixation and replacement [7]. In young adults, the main goals are to preserve the femoral head, to reduce iatrogenic insult and pseudoarthrosis to avoid total hip replacement [7].
Such a complex fracture pattern presents several dilemmas concerning the choice between open reduction internal fixation and closed reduction internal fixation (CRIF) procedures, as well as the choice of implants. While most reports mention CRIF to treat these injuries, Dhar et al., and Sayegh et al., resorted to open reduction [4,5,6,8,9]. In our case, we were able to achieve a satisfactory reduction after giving gentle traction on a fracture table. Most authors have recommended dynamic hip screw (DHS) and derotation screw as the modality of choice for fixing these fracture patterns [4,5,9]; however, in our case, we opted not to use the DHS due to the risk of the entry site of the Richard screw coinciding with the fracture site, which could potentially result in a deficient lateral femoral wall resulting in implant failure. We used two 6.5 mm CC screws to stabilize and achieve compression across the femoral neck fracture and then used one 6.5 mm CC screw to lag the GT to the femoral head. This screw also acted like a Pauwel screw used for fixation of unstable femoral neck fractures [10]. A 4th screw was passed from the GT toward the lesser trochanter. Thus, we could achieve good fixation of both the femoral neck as well as the trochanteric fragment using screws that were passed percutaneously under image intensifier guidance. There was no loss of reduction in the post-operative period and the construct held the fractures well with union of both fractures by 3 months. The patient also had a good range of motion with no pain and there were no radiological changes of AVN till the latest follow-up at 1 and ½ years post-operative.
Concomitant neck of femur and GT fracture in young adults is a rare and difficult fracture pattern presenting challenges as to the optimum modality of fixation. Although mostly DHS has been used to treat this fracture, it can also be managed by multiple CC screws, avoiding the risk of lateral wall instability inherent with DHS fixation in this fracture pattern.
To ensure successful surgical outcomes and prevent procedure failure, meticulous pre-operative planning is essential when deciding between closed reduction internal fixation and open reduction internal fixation, as well as when choosing the most suitable implant. In addition, adequate reduction is of paramount importance.
References
- 1. Li ZY, Cheng WD, Qi L, Yu SS, Jing JH. Complex proximal femoral fracture in a young patient followed up for 3 years: A case report. World J Clin Cases 2022;10:283-8. [Google Scholar] [PubMed]
- 2. Neogi DS, Ajay Kumar KV, Trikha V, Yadav CS. Ipsilateral femoral neck and trochanter fracture. Indian J Orthop 2011;45:82-6. [Google Scholar] [PubMed]
- 3. Biesemans S. Segmental fractures of the neck of femur: Fix or replace? Arthroplast Today 2021;8:247-52. [Google Scholar] [PubMed]
- 4. Dhar SA, Mir MR, Butt MF, Farooq M, Ali MF. Osteosynthesis for a T-shaped fracture of the femoral neck and trochanter: A case report. J Orthop Surg (Hong Kong) 2008;16:257-9. [Google Scholar] [PubMed]
- 5. Loupasis G, Ntagiopoulos PG, Asimakopoulos A. Concomitant ipsilateral subcapital and intertrochanteric fractures of the femur: A case report. J Med Case Reports 2010;4:363. [Google Scholar] [PubMed]
- 6. Butt MF, Dhar S, Hussain A, Gani N, Kangoo K, Farooq M. Femoral neck fracture with ipsilateral trochanteric fracture: Is there room for osteosynthesis. Internet J Orthop Surg 2007;5:1. [Google Scholar] [PubMed]
- 7. Tahir M, Lakkol S, Naique S. Segmental neck of femur fractures: A unique case report of an ipsilateral subcapital, greater trochanteric and intertrochanteric fracture and proposed management algorithm. Int J Surg Case Rep 2014;5:277-81. [Google Scholar] [PubMed]
- 8. Sayegh FE, Karataglis D, Trapotsis SJ, Christoforides JE, Pournaras JD. Concomitant ipsilateral pertrochanteric and subcapital fracture of the proximal femur. Eur J Trauma 2005;31:64-7. [Google Scholar] [PubMed]
- 9. Saleeb H, Kanvinde R, Rahman T. Literature review and case report: Current concepts for concomitant intra and extracapsular fractures of neck of femur in elderly patients. Trauma Case Rep 2017;8:24-31. [Google Scholar] [PubMed]
- 10. Xue G, Chen S, Zhou M, Wang Z, Wan L, Xie J, et al. Pauwels screw combined inverted triangle cannulated screws for the treatment of Pauwels type-III femoral neck fracture: A new surgical method based on the morphology of the fracture. 2020. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Proximal Hamate Autograft in Non-union Proximal Scaphoid Fractures, A Novel Technique – A Case Report
February 1, 2026 Proximal Hamate Autograft in Non-union Proximal Scaphoid Fractures, A Novel Technique – A Case Report January 1, 2026 Extra-Articular Distal Tibia Non-Union Treated With Ipsilateral Fibular Strut Graft with Implants In Situ – A Case Report
January 1, 2026 Extra-Articular Distal Tibia Non-Union Treated With Ipsilateral Fibular Strut Graft with Implants In Situ – A Case Report January 1, 2026 Successful Management of a 40-Year-Old Non-union of the Humeral Shaft with Pseudoarthrosis with Plate Fixation and Bone Grafting: A Case Report
January 1, 2026 Successful Management of a 40-Year-Old Non-union of the Humeral Shaft with Pseudoarthrosis with Plate Fixation and Bone Grafting: A Case Report November 1, 2025 Complications and Functional Outcomes in Open Tibia-Fibula Fractures: A Retrospective Analysis from a Tertiary Care Centre
November 1, 2025 Complications and Functional Outcomes in Open Tibia-Fibula Fractures: A Retrospective Analysis from a Tertiary Care Centre