
A posterior approach for single-stage ORIF enables effective management of rare medial Hoffa fractures with PCL avulsion, ensuring precise reduction and excellent outcomes.
Dr. Kishor Munde, Department of Orthopaedics, Medicover Hospital, N6-CIDCO, Chhatrapati Sambhajinagar - 431001, Maharashtra, India. E-mail: drkishormunde@gmail.com
Introduction: Medial Hoffa fractures are rare intra-articular injuries of the femoral condyle, and their association with posterior cruciate ligament (PCL) avulsion fractures presents a highly uncommon and complex clinical scenario. This case report describes the successful surgical management of such a combination using a posterior open approach.
Case Report: A 48-year-old male sustained a medial Hoffa fracture with a PCL avulsion following a road traffic accident. Surgical intervention involved open reduction and internal fixation (ORIF) through a posterior approach, allowing direct access to both fracture sites. The PCL avulsion fragment was anatomically reduced and fixed with a cancellous screw, while the Hoffa fracture was stabilized using opposing Herbert screws. Postoperatively, the patient underwent structured rehabilitation with an early range of motion exercise. At 6 months, the patient achieved full knee function (0–130°), no instability, and high functional scores. Radiographs showed complete union, and follow-up at 18 months confirmed maintained function without complications.
Conclusion: This case highlights the effectiveness of a posterior approach for single-stage ORIF in managing rare medial Hoffa fractures with PCL avulsion. Early surgical intervention, anatomical fixation, and dedicated rehabilitation are key to achieving optimal outcomes in such complex knee injuries.
Keywords: Medial Hoffa, posterior cruciate ligament avulsion, posterior open reduction and internal fixation.
Hoffa fractures are an uncommon type of supracondylar femur fractures characterized by an intra-articular fracture of the femoral condyle in the coronal plane. Among these, medial Hoffa fractures are even less common and present unique challenges due to their anatomical location and the complex biomechanics involved [1,2]. In addition, concurrent posterior cruciate ligament (PCL) avulsion fractures further complicate management and can impact functional outcomes. This case report presents a 48-year-old male patient who sustained a medial Hoffa femur fracture along with a PCL avulsion fracture and was successfully treated with single-stage open reduction and internal fixation (ORIF) through posterior approach. To the best of our knowledge, only one case of a Medial Hoffa fracture associated with PCL avulsion fracture has been reported previously in English literature [3].
A 48-year-old male presented to the emergency department following a motor vehicle accident with complaints of severe pain, swelling, and inability to bear weight on his left lower limb. On examination, there was significant swelling around the knee joint with marked tenderness over the medial femoral condyle. The patient was unable to perform active knee flexion or extension. Distal neurovascularity was intact. Initial radiographs revealed a coronal plane fracture of the medial femoral condyle, consistent with a Hoffa fracture. In addition, a displaced PCL avulsion fracture was seen (Fig. 1).
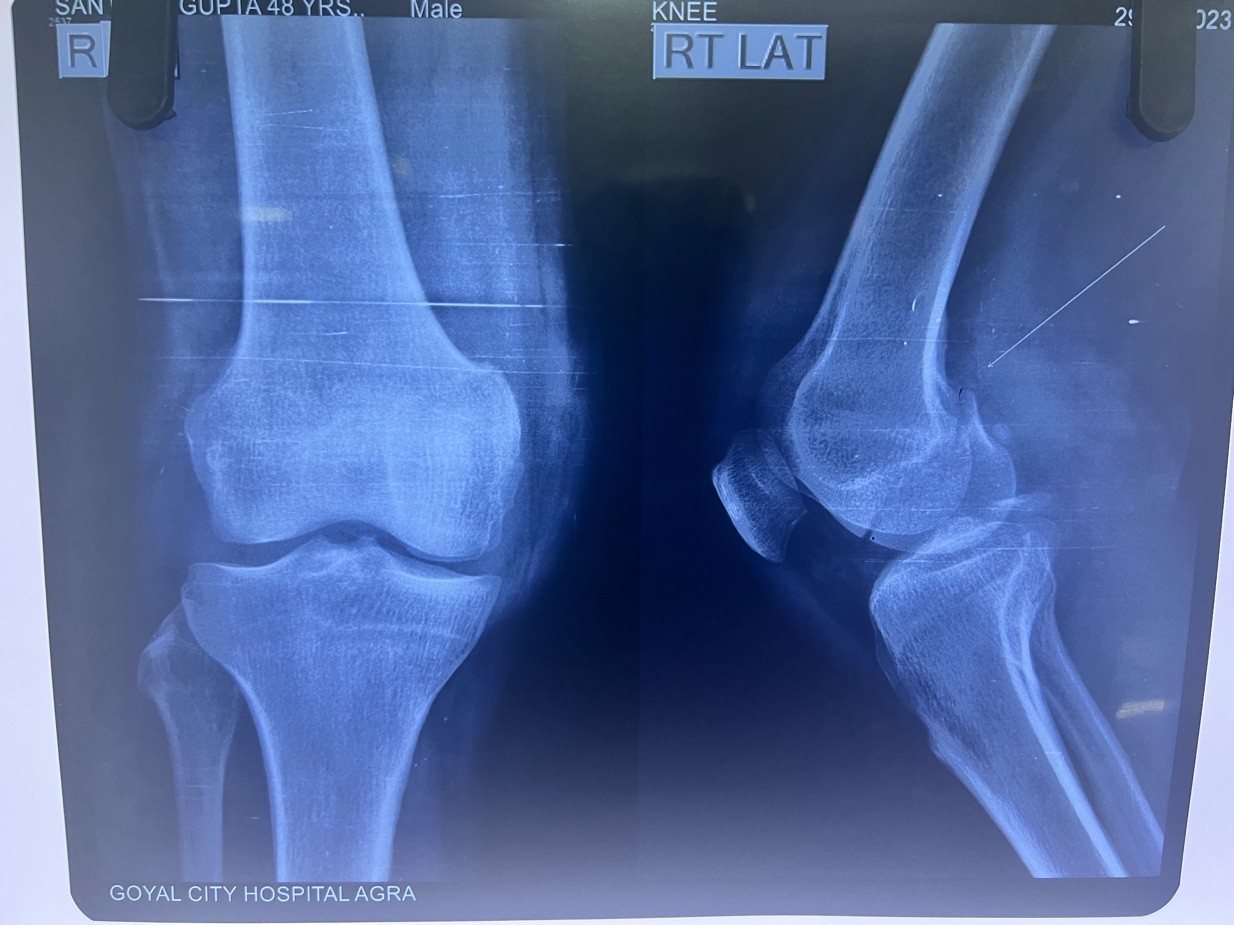
Figure 1: Pre-operative X-rays showing a medial Hoffa fracture with the posterior cruciate ligament avulsion fracture.
Magnetic resonance imaging (MRI) scan was performed to better delineate the associated other ligaments and chondral injuries (Fig. 2).
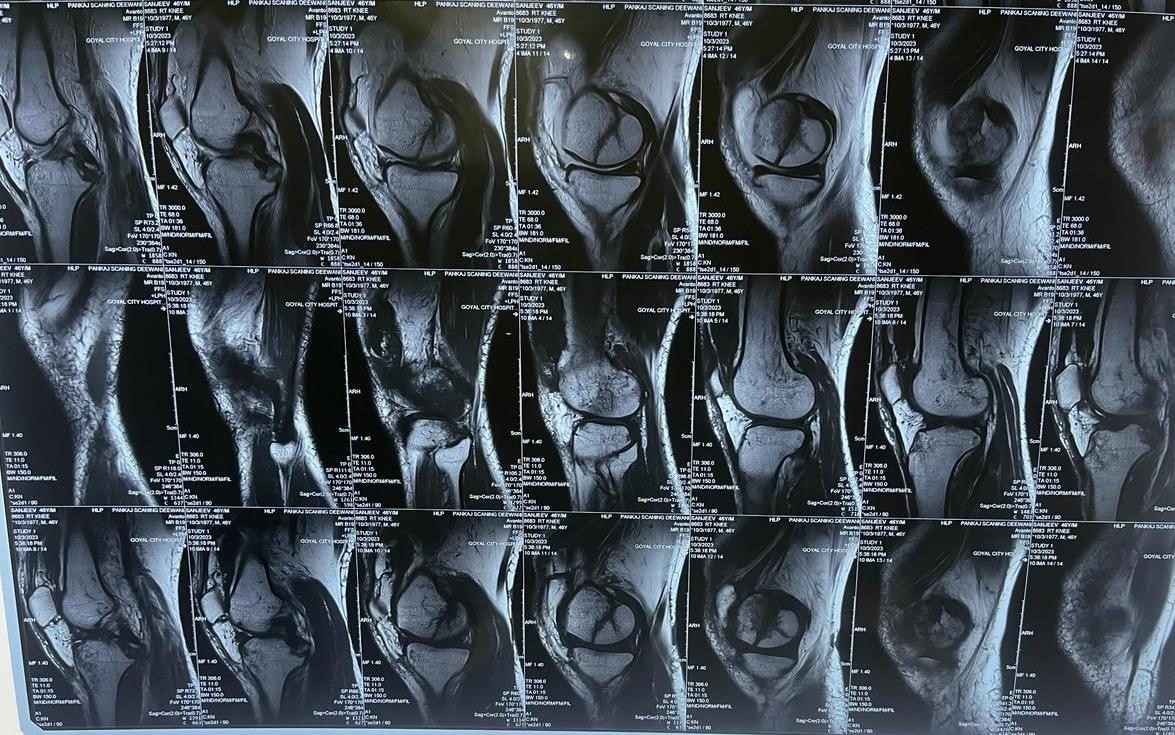
Figure 2: Pre-operative magnetic resonance imaging sagittal images showing posterior cruciate ligament avulsion fracture with Hoffa fracture.
Surgical management
Given the complexity of the fracture and the associated PCL avulsion, the decision was made to proceed with ORIF through a posterior approach to address both injuries. Under spinal anesthesia and additional sedation, the patient was placed prone on the operating table. In order to maximize access to the posterior aspect of the knee, the affected limb was placed on a padded bolster. This arrangement minimized strain on the neurovascular structures while enabling direct visualization of the fractures. A reverse L-shaped incision was taken by the posterior approach, starting above the popliteal crease and running vertically down the midline before curving medially (Fig. 3).

Figure 3: Intraoperative reverse L-shaped skin incision in the prone position.
Careful dissection was performed to protect the popliteal neurovascular bundle, including the tibial nerve and popliteal vessels, which were gently retracted throughout the procedure. The PCL avulsion fracture was identified, and the fragment was cleared of soft-tissue interposition to ensure an optimal reduction. Under fluoroscopic guidance PCL fragment was reduced anatomically and temporarily stabilized using Kirschner wires. A definitive fixation was achieved using a partially threaded cancellous compression screw with a washer from the avulsed fragment to the tibia.
The medial Hoffa fracture was also addressed during the same procedure. The fracture was anatomically reduced and temporarily stabilized with Kirschner wires. Two Herbert screws were then inserted, one in an anterior–posterior direction and the other in a posterior–anterior direction, ensuring compression and stabilization of the fracture plane (Fig. 4a and b).
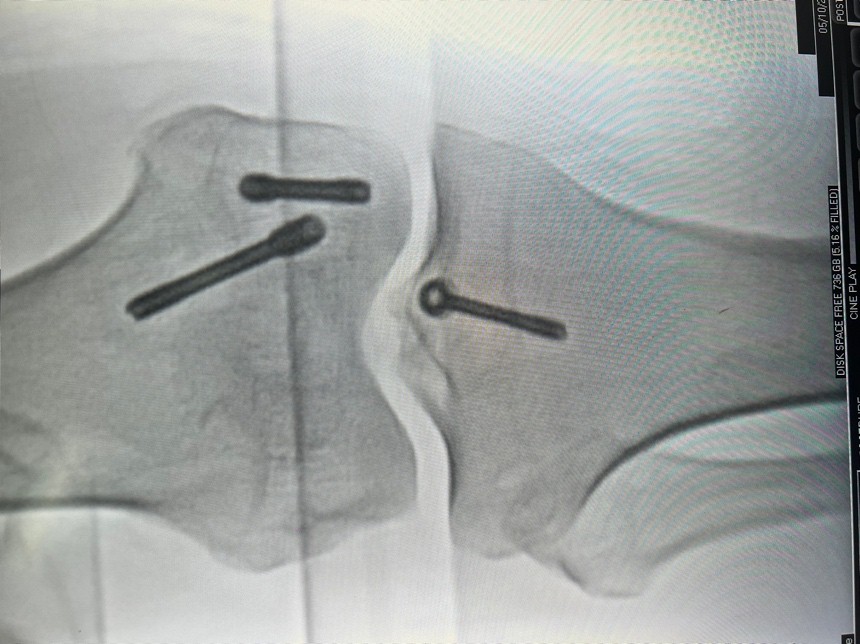
Figure 4: (a and b) Intraoperative fracture fixation anteroposterior and lateral images.
This opposing screw configuration provided robust fixation, and intraoperative fluoroscopy was used to ensure accurate alignment and the adequacy of fracture reduction.
Postoperatively, the patient was immobilized in a knee brace for the initial period to allow for adequate healing of the fracture and PCL fixation. Early passive range of motion exercises were initiated after 2 weeks, followed by a gradual progression to active range of motion and strengthening exercises. The patient was non-weight-bearing for the first 6 weeks and then transitioned to partial weight-bearing as tolerated. The patient was followed up at regular intervals postoperatively. At 6 months, the patient demonstrated excellent functional outcomes. He achieved a knee range of motion from 0 to 130° with no significant pain or instability (Fig. 5a, b, c). Radiographs confirmed satisfactory fracture union (Fig. 6a and b).

Figure 5: (a, b, c) Clinical follow-up showing knee range of motion, no posterior sag, and cross-leg sitting.
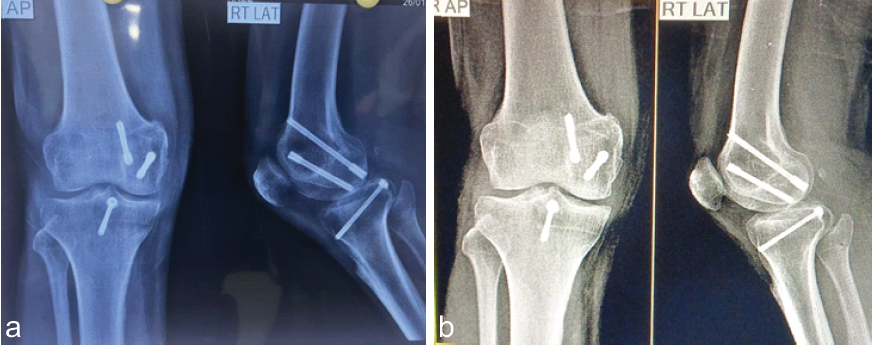
Figure 6: (a and b) Radiographic follow-up at 6 months and 18 months showing healed fracture.
Functional assessment using the knee injury and osteoarthritis outcome score and the Lysholm knee scoring scale revealed high scores, indicating excellent knee function and patient satisfaction. The patient was further followed up for 18 months, revealing no functional deficit or pain.
Hoffa fractures are often associated with various distal femoral injuries, such as supracondylar, bicondylar, and unicondylar fractures, as well as ligamentous injuries, meniscal tears, and neurovascular damage [1,4]. Medial Hoffa fractures alone are uncommon, representing a minority of all Hoffa fractures, which themselves account for only 0.65% of all femur fractures [5]. The presented case of a medial Hoffa fracture combined with a PCL avulsion is a rare and complex injury pattern. Medial Hoffa fractures are particularly challenging due to the load-bearing nature of the medial femoral condyle, increasing the risk of displacement. The concurrent PCL avulsion adds further complexity, as improper treatment may lead to long-term knee instability and functional impairment. Given their intra-articular nature, Hoffa fractures require surgical intervention for optimal outcomes. In this case, a posterior approach for ORIF was chosen, offering direct access to both the medial femoral condyle and the PCL fragment. Although less commonly used than the anterior approach, the posterior approach provides superior visualization of the posterior knee structures and allows for precise anatomical reduction, which is essential to restoring function and minimizing complications such as post-traumatic arthritis [6,7]. When comparing arthroscopic versus open fixation for these types of fractures, each technique has its advantages. Arthroscopic fixation offers the benefit of minimal invasiveness, potentially reducing soft-tissue damage and post-operative recovery time. It provides good visualization for certain intra-articular fractures, particularly in lateral Hoffa fractures, and can be useful for treating concurrent ligament injuries such as PCL avulsions [8]. However, for complex fractures involving the medial condyle, such as the present case, the open posterior approach is often favored due to its superior direct access to the fracture site, allowing for more precise reduction and fixation. Arthroscopic techniques may also be limited by the technical difficulty of addressing larger fragments or severely displaced fractures. Single-stage ORIF is the gold standard for displaced Hoffa fractures and PCL avulsion injuries, as it allows for stable fixation of both bony and ligamentous structures, facilitating early mobilization and reducing the risk of stiffness. Previous studies on Hoffa fractures have shown that early complications such as joint stiffness and infection are relatively uncommon when anatomical reduction and stable fixation are achieved. A similar case report documented a comparable injury treated using a similar approach, with good outcomes in terms of knee function and stability [3]. Another recent case report describes the treatment of a lateral Hoffa fracture combined with a PCL avulsion fracture using a posteromedial approach [9]. The determination of an appropriate fixation strategy for Hoffa fractures is contingent on several critical determinants, including fracture configuration, bone quality, chosen surgical approach, and the patient’s physiological status and pre-injury functional capacity [10]. This case highlights the effectiveness of the posterior approach in managing complex medial Hoffa fractures with associated PCL avulsion fractures. The excellent functional outcomes in this patient emphasize the importance of meticulous surgical technique and comprehensive post-operative rehabilitation.
Single-stage posterior ORIF facilitates anatomical reduction and stable fixation in complex knee injuries, including medial Hoffa fracture associated with PCL avulsion, ensuring restoration of biomechanics and better functional outcomes.
Medial Hoffa fractures with associated PCL avulsion, though rare and complex, can be successfully managed with a single-stage posterior approach ORIF, where early anatomical fixation combined with structured rehabilitation leads to excellent functional recovery and joint stability.
References
- 1. Pathak S, Salunke A, Karn S, Ratna HV, Thivari PS, Sharma S, et al. Hoffa’s fracture with associated injuries around the knee joint: An approach to a rare injury. Cureus 2020;12:e7865. [Google Scholar] [PubMed]
- 2. Zhou Y, Pan Y, Wang Q, Hou Z, Chen W. Hoffa fracture of the femoral condyle: Injury mechanism, classification, diagnosis, and treatment. Medicine ((Baltimore) 2019;98:e14633. [Google Scholar] [PubMed]
- 3. Lu Y, Hsu L, Yeh S, Hsu Y, Chen Y. Concomitant hoffa and posterior cruciate ligament avulsion fractures: A rare case report. Formos J Musculoskelet Disord 2022;13:e14633. [Google Scholar] [PubMed]
- 4. Bandebuche A, Munde K, Sharan S. Open lateral condyle Hoffa’s fracture with intra-articular patella dislocation, quadriceps tendon rupture and PCL avulsion. BMJ Case Rep 2024;17:e258433. [Google Scholar] [PubMed]
- 5. Patel PB, Tejwani NC. The Hoffa fracture: Coronal fracture of the femoral condyle a review of literature. J Orthop 2018;15:726-31. [Google Scholar] [PubMed]
- 6. Liu Q, Wang W, Fan W, Zhu W. Hoffa fracture associated with tibial shaft fracture and multiple ligament avulsion fractures: A case report. Trauma Case Rep 2020;26:100277. [Google Scholar] [PubMed]
- 7. Hooper PO, Bevan PJ, Silko C, Farrow LD. A posterior approach to open reduction and internal fixation of displaced posterior cruciate ligament tibial osseous avulsions. JBJS Essent Surg Tech 2018;8:e6. [Google Scholar] [PubMed]
- 8. Souto CS, Bicas Machado D, Rodrigues N, Tavares N. All arthroscopic management of an Hoffa fracture of the medial femoral condyle: Case report. J Orthop Rep 2025;4:100335. [Google Scholar] [PubMed]
- 9. Salman LA, Shujauddin M, Babikir E, Alkhayarin M. Complex PCL avulsion and hoffa fractures with a unique posteromedial approach: A case report. Biomed J Sci Techn Res 2022;43:34221-6. [Google Scholar] [PubMed]
- 10. Akel A, Sarhan MY, Abu-Jeyyab M, Daradkeh ST, Moseley S, Dawoud MS. Medial Hoffa fracture: A case report and literature review of approach and management. Am J Case Rep 2024;25:e943136. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2025 A Rare Case Report: Managing PCL Avulsion Fracture with a Fracture of the Proximal Tibial Shaft
January 1, 2025 A Rare Case Report: Managing PCL Avulsion Fracture with a Fracture of the Proximal Tibial Shaft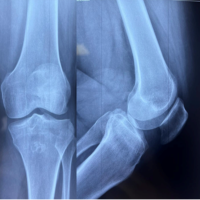 October 10, 2023 Posterior Cruciate Ligament Avulsion with Posterior Tibial Rim Fracture: A Case Report
October 10, 2023 Posterior Cruciate Ligament Avulsion with Posterior Tibial Rim Fracture: A Case Report April 15, 2012 JOCR Acknowledges the Reviewers
April 15, 2012 JOCR Acknowledges the Reviewers October 14, 2014 Osteomyelitis of Myositis Ossificans in Arm – First Case Report
October 14, 2014 Osteomyelitis of Myositis Ossificans in Arm – First Case Report