
This case demonstrates that total hip arthroplasty using the Restoration GAP II reinforcement ring can be a practical and effective solution for patients with severe acetabular bone defects, especially when conventional implants are unsuitable due to anatomical constraints and bone defects.
Dr. Hiroki Kobayashi, Department of Orthopedic Surgery, National Defense Medical College, Saitama, Japan. E-mail: supercova0205@gmail.com
Introduction: Total hip arthroplasty (THA) in patients with severe acetabular bone defects remains technically demanding. Although favorable outcomes have been reported with Kerboull-type acetabular plates, the clinical results of the Restoration GAP II reinforcement ring (GAP II ring) have been inconsistent. We report a case of hip osteoarthritis with severe acetabular bone defects following rotational acetabular osteotomy, successfully treated with THA using the GAP II ring.
Case Report: We report a case of an 80-year-old woman who underwent rotational acetabular osteotomy 20 years ago and subsequently developed hip osteoarthritis with severe acetabular bone defects that required acetabular reconstruction. Anatomical placement of the acetabular component and fixation with a cementless cup were deemed inapplicable due to the extent of the bone defects.
Conclusion: Therefore, the Restoration GAP II reinforcement ring, which has multiple screw insertion points and customizable hook bending, was selected for reinforcement. Given the poor bone quality, autologous bone grafting was considered unsuitable, and bone cement was used to fill the defects. Total hip arthroplasty was successfully performed using the reinforcement ring, and the patient was allowed full weight-bearing ambulation from post-operative day 1. At 18 months after surgery, she reported no recurrence of pain or difficulties in walking. This case suggests that satisfactory outcomes can be achieved in cases with severe acetabular bone defects through the appropriate application of a reinforcement ring.
Keywords: Total hip arthroplasty, acetabular bone defect, restoration GAP II reinforcement ring, acetabular reconstruction, hip osteoarthritis.
Total hip arthroplasty (THA) can be technically challenging in patients with severe acetabular bone defects. Various techniques have been developed to address this issue, including the use of reinforcement devices [1]. Although favorable outcomes have been reported with the Kerboull-type acetabular plate (KT plate) [2,3], clinical results with the Restoration GAP II reinforcement ring (GAP II ring) have been mixed [4,5]. Here, we present a case of hip osteoarthritis with severe acetabular bone defects following rotational acetabular osteotomy that was successfully managed by THA using the GAP II ring.
An 80-year-old woman underwent rotational acetabular osteotomy 20 years ago for right hip dysplasia and osteoarthritis. However, she experienced persistent post-operative hip pain and gradually developed severe joint contracture. At the time of presentation to our hospital, she required crutches for ambulation due to intense right hip pain. The affected limb was approximately 5 cm shorter than the contralateral side. The range of motion of the right hip was markedly restricted, with 20° flexion, 0° extension, 5° abduction, 10° adduction, 0° external rotation, and 30° internal rotation. Radiographs demonstrated that the right femoral head was deformed and dislocated proximally (Fig. 1).
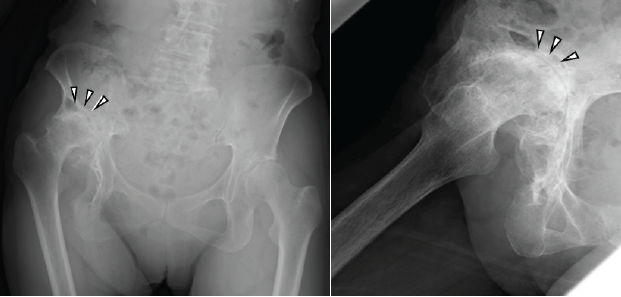
Figure 1: Radiographs at the first visit (left, anteroposterior view; right, lateral view). The images reveal high dislocation of the right hip, deformity of the femoral head, and severe narrowing of the joint space (arrowheads).
Computed tomography revealed a severely deformed acetabulum, manifested by excessive anterior over coverage, a posterior wall deficiency, and a bone defect in the superior weight-bearing region of the acetabulum (Fig. 2).
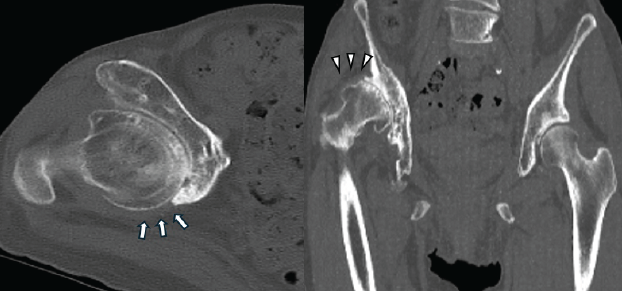
Figure 2: Pre-operative computed tomography images (left, axial view; right, horizontal view). The axial view shows excessive anterior acetabular coverage and a posterior wall defect (arrows). The horizontal view shows a severe bone defect in the superior aspect of the acetabulum, corresponding to the weight-bearing region (arrowheads).
Based on these observations, the case was classified as Crowe grade 3 osteoarthritis. Due to the severe high dislocation of the femoral head and joint contracture, anatomical reduction of the hip joint was considered infeasible. In addition, the extent of posterior and superior bone defects precluded secure fixation using a press-fit cementless cup. Therefore, the use of a reinforcement ring was deemed necessary, and the GAP II ring was selected for its capacity to accommodate multiple screw fixations and flexible hook bending. The procedure was performed through the ALS approach. Due to excessive anterior wall coverage, removal of the femoral head necessitated partial excision of the anterior wall. Osteophytes that could cause joint impingement were also removed (Fig. 3).
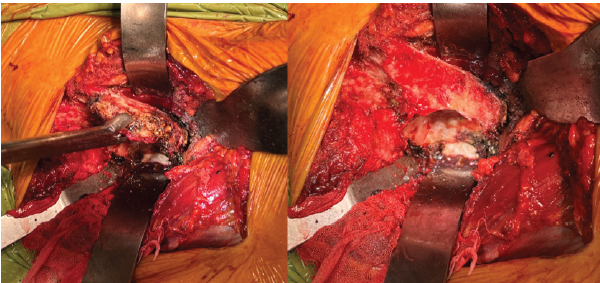
Figure 3: Intraoperative findings. Excessive anterior wall coverage and extensive osteophyte formation surrounding the acetabulum are observed (left panel). The anterior over coverage is removed and the acetabular is exposed (right panel).
As anticipated, soft-tissue contracture obstructed the reduction of the femoral head component into the original acetabular socket. Because the hook of the reinforcement ring could not reach the obturator foramen, the acetabular floor was excavated, and the reinforcement ring was positioned more superiorly within the ilium. Due to bone fragility, bone grafting was deemed unsuitable; thus, the gap between the reinforcement ring and the acetabulum was filled with bone cement. Fifteen screws were placed into the acetabulum in all directions except the defective posterior region (Fig. 4 and 5).

Figure 4: Placement of the GAP II ring. The hook is inserted into the acetabular floor, and the reinforcement ring is securely fixed using multiple screws.
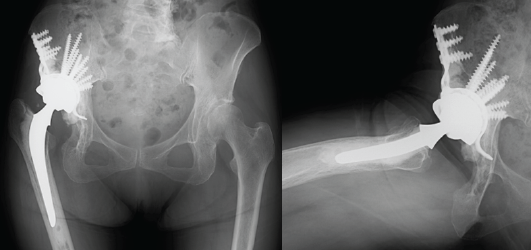
Figure 5: Post-operative radiographs (left, anteroposterior view; right, lateral view).
Posterior soft tissues were preserved to ensure joint stability. She was allowed full weight-bearing from the 1st post-operative day and was able to walk outdoors with a cane by post-operative day 19. The range of hip flexion improved from 20° to approximately 100° after surgery. At the 18-month follow-up, she reported no hip dislocation or recurrence of pain.
Osteotomies for patients with hip dysplasia, including rotational acetabular osteotomy, have demonstrated favorable long-term outcomes [6,7,8,9]. However, for patients who developed osteoarthritis following osteotomy, THA often requires acetabular reconstruction with a reinforcement ring [10]. For this purpose, the Müller Ring, Ganz Ring, and Burch–Schneider reinforcement cage (BS Cage) are commonly used worldwide B11]. In Japan, the KT plate and BS Cage are often used and generally yield favorable outcomes [2,3]. While the GAP II ring has shown promising short-term results (≤5 years) [4], mid- to long-term outcomes (>5 years) have raised concerns due to implant loosening [5]. In the present case, we initially considered the KT plate, BS Cage, and GAP II ring as potential options. The KT plate was excluded due to its relatively short hook, lack of malleability, and the limited number of screw holes (four), which provided insufficient fixation strength in our case. The BS Cage has 8–10 screw holes and a malleable flange; however, because its flange is relatively short and cannot be inserted into the ischium, it was considered not suitable for our case. The GAP II ring has 15–20 screw holes and a malleable hook, which allows secure placement into the acetabular floor, even though the hook does not reach the obturator foramen. Although the long-term outcomes of the GAP II ring are not uniformly favorable, it was considered acceptable in this case, given the patient’s advanced age. Custom triflange cups may also be suitable for our case; however, the use of those implants is currently not approved in Japan. Another important consideration in acetabular reconstruction is the management of bone defects. Since the use of structural allografts around the acetabulum has been associated with poor outcomes [12], and our patients had highly fragile bone, we opted for complete cement interposition instead of grafting. We believe this approach also contributed to the favorable short-term outcomes in our case.
We achieved favorable short-term outcomes using the GAP II ring to treat a hip osteoarthritis patient with severe acetabular bone defects. Although further clinical studies are warranted, with careful patient selection and pre-operative planning, the GAP II ring may represent a viable option for complex and challenging hip osteoarthritis cases requiring acetabular reconstruction.
Total hip arthroplasty using the Restoration GAP II reinforcement ring can be a viable option for patients with severe acetabular bone defects, especially when conventional implants are unsuitable due to anatomical or structural limitations.
References
- 1. Han W, Zhang H. Application of acetabulum reinforcement ring for reconstructing acetabular defects in artificial hip replacement. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2009;23:201-4. [Google Scholar] [PubMed]
- 2. Kamada T, Imai H, Mahima N, Takeba J, Miyawaki J, Miura H. Acetabular reconstruction with the Kerboull-type plate at mid-term follow-up: Survivorship analysis and prognostic factors for loosening. Eur J Orthop Surg Traumatol 2018;28:485-91. [Google Scholar] [PubMed]
- 3. Inoue D, Kabata T, Maeda T, Kajino Y, Yamamoto T, Takagi T, et al. The value of bulk femoral head allograft in acetabular reconstruction using Kerboull-type plate. Int Orthop 2015;39:1839-44. [Google Scholar] [PubMed]
- 4. Taheriazam A, Saeidinia A. Evaluation results of using GAP II acetabular cage for acetabulum in revision total hip arthroplasty. Medicine (Baltimore) 2022;101:e32056. [Google Scholar] [PubMed]
- 5. Buttaro MA, De La Rosa DM, Comba F, Piccaluga F. High failure rate with the GAP II ring and impacted allograft bone in severe acetabular defects. Clin Orthop Relat Res 2012;470:3148-55. [Google Scholar] [PubMed]
- 6. Willemsen K, Niemeyer MJ, Harlianto NI, Sadiqi S, Seevinck PR, Sakkers RJ, et al. Good long-term outcomes of the hip Chiari osteotomy in adolescents and adults with hip dysplasia: A systematic review. Acta Orthop 2022;93:296-302. [Google Scholar] [PubMed]
- 7. Cho YJ, Kim KI, Kwak SJ, Ramteke A, Yoo MC. Long-term results of periacetabular rotational osteotomy concomitantly with arthroscopy in adult acetabular dysplasia. J Arthroplasty 2020;35:2807-12. [Google Scholar] [PubMed]
- 8. Chiari C, Schneider E, Stamm T, Peloschek P, Kotz R, Windhager R. Ultra-long-term results of the Chiari pelvic osteotomy in hip dysplasia patients: A minimum of thirty-five years follow-up. Int Orthop 2024;48:291-9. [Google Scholar] [PubMed]
- 9. Yasunaga Y, Ochi M, Yamasaki T, Shoji T, Izumi S. Rotational acetabular osteotomy for pre- and early osteoarthritis secondary to dysplasia provides durable results at 20 years. Clin Orthop Relat Res 2016;474:2145-53. [Google Scholar] [PubMed]
- 10. Yuasa T, Maezawa K, Nozawa M, Kaneko K. Total hip arthroplasty after previous rotational acetabular osteotomy. Eur J Orthop Surg Traumatol 2015;25:1057-60. [Google Scholar] [PubMed]
- 11. Aprato A, Olivero M, Branca Vergano L, Massè A. Outcome of cages in revision arthroplasty of the acetabulum: A systematic review. Acta Biomed 2019;90:24-31. [Google Scholar] [PubMed]
- 12. Duffy GP, O’Connor MI, Brodersen MP. Fatigue failure of the GAP ring. J Arthroplasty 2007;22:711-4. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Irreducible Periprosthetic Hip Dislocation Due to Muscular Entrapment with Concomitant Sciatic Nerve Involvement
February 1, 2026 Irreducible Periprosthetic Hip Dislocation Due to Muscular Entrapment with Concomitant Sciatic Nerve Involvement January 1, 2026 A Rare Case of Metabolic Disorder of Bilateral Fracture Neck Femur Treated with Bilateral Total Hip Arthroplasty
January 1, 2026 A Rare Case of Metabolic Disorder of Bilateral Fracture Neck Femur Treated with Bilateral Total Hip Arthroplasty January 1, 2026 Candida albicans Periprosthetic Hip Infection Complicated by Recurrent Dislocations Following Revision Total Hip Arthroplasty: A Case Report
January 1, 2026 Candida albicans Periprosthetic Hip Infection Complicated by Recurrent Dislocations Following Revision Total Hip Arthroplasty: A Case Report January 1, 2026 Effect of Routes of Administration of Tranexamic Acid in Peri-Operative Blood Loss in Total Hip Arthroplasty: A Prospective Comparative Study
January 1, 2026 Effect of Routes of Administration of Tranexamic Acid in Peri-Operative Blood Loss in Total Hip Arthroplasty: A Prospective Comparative Study