
Pointers on achieving successful functional outcomes from the surgical management of a rare clinical entity-aneurysmal bone cyst of the clavicle.
Dr. Senthil Kumar, Institute of Orthopaedics and Traumatology, Madras Medical College, Chennai, Tamil Nadu, India. E-mail: senthilkumarortho@gmail.com
Introduction: Clavicle neoplasms account for only 1.01% of bone tumors and the possibility of it being a primary aneurysmal bone cyst is incidentally low. Although rare in incidence, most of the cases reported were treated with en bloc resection either as a primary procedure or during recurrence. The rarity of the disease and the lack of medical literature poses a diagnostic dilemma for the treating orthopedic surgeon, radiologist, and pathologist, that could potentially lead to the lesions being diagnosed at a stage when options to salvage the bone can no longer be considered. In our case, early meticulous work-up, prompt surgical intervention, and strict follow-up enabled us to salvage the bone and, more importantly, preserve the acromioclavicular joint; hence, offering better functional outcome for the patient.
Case Report: A 23-year-old female presented with complaints of pain in the left collarbone and restricted movement in the shoulder. Clinically, a bony irregularity was palpable over the left clavicle with associated tenderness. Patient was subjected to various radiological imaging and tissue sampling to aid in the establishment of a pre-operative diagnosis. A diagnostic dilemma arose as the investigations opened up a wide plethora of differentials. Considering the age of the patient and the provisional diagnosis of “giant cell lesion,” an attempt was made to salvage the bone and preserve shoulder function. The patient underwent extended curettage, cancellous bone grafting, and augmentation plating. Intraoperative samples were sent for histopathology and the lesion turned out to be one among the least likely on the list of possible differential diagnosis – a primary aneurysmal bone cyst. A meticulous follow-up protocol was devised during which functional outcome was found to be excellent and there was no recurrence at 15 months.
Conclusion: Through this case report, we would like to emphasize on the importance of broadening the spectrum of differential diagnosis while investigating tumors at a rare site. This was achieved by devising a meticulous pre-operative radiological and histopathological diagnostic protocol encompassing a spectrum of differential diagnosis. Establishing an early diagnosis gives us an option to opt for surgical interventions for bone salvage and, thus, achieve better functional outcome for the patient.
Keywords: Aneurysmal bone cyst, clavicle tumor, clavicle swelling.
Aneurysmal bone cysts are blood filled cavities in the bone that typically present as expansile, lytic lesions in the femur, tibia, and vertebrae and show high predilection for pathological fractures. The primary hypothesis regarding the origin of aneurysmal bone cysts points to localized circulatory disruptions that lead to a substantial rise in venous pressure and the emergence of an expanded vascular network within the affected bone region [1]. However, persistent chromosomal patterns observed in some studies suggest that these lesions could be neoplastic. The following theories have been postulated for their etiology [2].
- Primary aneurysmal bone cysts arise spontaneously without any preceding trauma or presence of co-existing tumors. 69% of these lesions have clonal t(16,17) translocation that cause upregulation of TRE17/USP6 oncogene that activates matrix metalloproteinases and nuclear factor-kappa which have a destructive effect on extracellular matrix leading to the formation of bone cyst [2].
- Secondary aneurysmal bone cysts occur as an accompanying bone lesion to a separate primary bone tumor such as giant cell tumor, fibromas, fibrous dysplasia, and osteosarcoma, among others; and from a site of prior trauma to the bone [2].
Majority of aneurysmal bone cysts occur in the metaphysis of long bones (67%) and spine (15%) and are almost unheard-of in other regions, such as the clavicle.
Chance of recurrence is highest 6 months post-intervention and unlikely after 2 years.
Through this case report, we present to you a rare case of clavicle neoplasm evaluated, operated, and followed-up at Institute of Orthopedics and Traumatology, Madras Medical College, Chennai.
A 23-year-old female, in the immediate post-partum period, presented to the orthopedics out-patient department with complaints of pain in the left collarbone and restricted movements in the left shoulder since 1 month. Her complaints began insidiously in the immediate post-partum period. Pain was initially dull-aching and poorly localized and it gradually increased in intensity, over a period of 1 month, from 6 to 8 on the visual analog scale (VAS). Patient also had complaints of inability to carry out activities of daily living that involved lifting her left arm above her head and carrying heavy objects.
Clinical examination revealed supraclavicular fullness on the left side. An irregularity was palpable over the left clavicle in the middle third with associated tenderness. Range of movements at the left shoulder was restricted due to pain- with an Oxford Shoulder Score of 38.
X-ray of the left shoulder revealed an osteolytic lesion in the middle third of the clavicle (Fig. 1).

Figure 1: Zero magnification X-ray of the left shoulder – anteroposterior view shows a 3 × 1 cm lytic lesion with surrounding areas of sclerosis.
Computed tomography scans were consistent with features of “giant cell tumor” and magnetic resonance imaging reported the possibility of “metastasis” or “multiple myeloma” (Figs. 2 and 3).
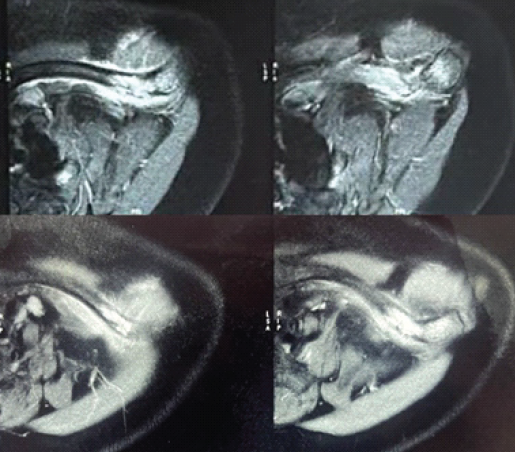
Figure 2: T2-weighted magnetic resonance imaging left shoulder: showing an expansile, fluid-filled, and lytic lesion in the mid-shaft of the clavicle with pathological fracture and surrounding soft-tissue edema.
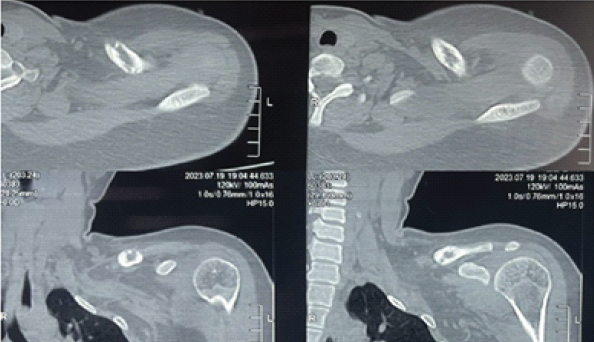
Figure 3: Computed tomography left shoulder showing 3 × 1.2 cm expansile lesion with scalloped inner margins and sclerosis – consistent with giant cell tumor.
Tissue diagnosis with ultrasound-guided biopsy of the lesion reported the lesion to be “a giant cell lesion.” Further radiological and histopathological evaluation failed to establish a conclusive pre-operative diagnosis.
The diagnostic conundrum was exacerbated by the various differentials it drew up, right from giant cell tumor, metastasis from occult primary, multiple myeloma, non-ossifying fibroma, fibrous dysplasia, primary or secondary aneurysmal bone cyst, osteoblastoma, chondroblastoma, giant cell rich or telangiectatic osteosarcoma, tuberculosis, eosinophilic granuloma, and subacute sclerosing osteomyelitis [3]. Further screening with blood tests was done with no reported significant abnormality (Table 1).
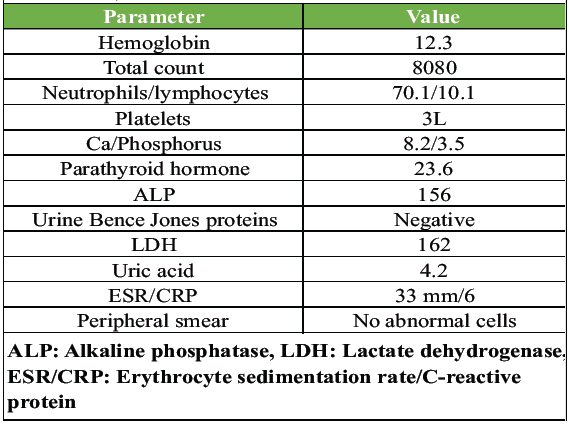
Table 1: Blood investigations: showing no significant abnormality
Considering the young age of the patient, the aim of our treatment plan was to salvage the clavicle and preserve the acromioclavicular joint function – which was achieved through extended mechanical and chemical curettage with high speed burr and hydrogen peroxide respectively, cancellous autograft placement from iliac crest, and augmentation plating (Figs. 4, 5, 6, 7).

Figure 4: Intraoperative image of the defect in the left clavicle post-extended curettage – 5 × 1 cm.
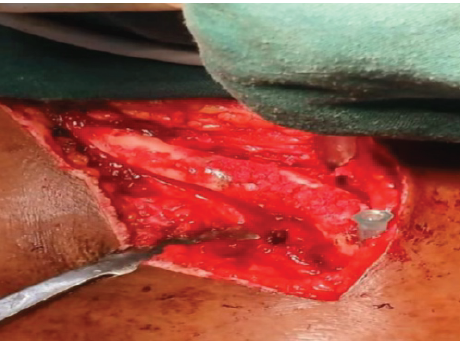
Figure 5: Packing of defect post curettage with cancellous bone autograft from ipsilateral iliac crest.

Figure 6: Augmentation plating with anatomical clavicle plate.
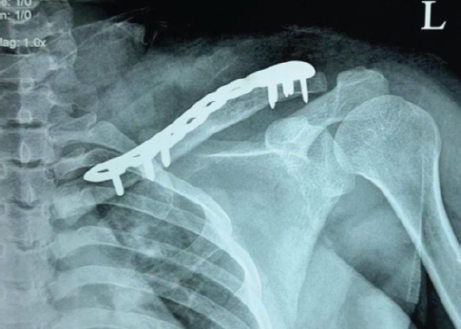
Figure 7: X-ray left shoulder anteroposterior view – immediate post-operative.
Curettage samples were sent for histopathological examination. Post-operative period was uneventful and shoulder mobilization exercises were initiated from the day of suture removal (post-operative day 12). The intraoperative samples provided us the least anticipated diagnosis – a primary aneurysmal bone cyst. Since, aneurysmal bone cysts do not typically occur in the clavicle and can occur secondary to other bone tumors, a repeat histopathological analysis of the intraoperative specimens was done to rule out the possibility of secondary aneurysmal bone cyst with unknown primary bone tumor and giant cell reparative granuloma – neither of which were reported after histopathological review.
At the time of discharge, patient’s surgical scar had healed by primary intention and her post-operative Oxford Shoulder Score was 29 (38 preoperatively; where a lower score denotes better function); signifying an improvement in shoulder function. Patient received a single dose of intravenous zoledronic acid.
According to available literature on aneurysmal bone cysts of the clavicle as well as aneurysmal bone cysts in other bones of the body, the highest chance of recurrence is within 6 months of intervention and highly unlikely after 2 years of surgery. Hence, the following follow-up protocol was devised with a primary aim to monitor recurrence – periodic reviews with X-rays, once a month for 6 months; followed by once every 3 months until 1 year, followed by once in 6 months until 2 years post-procedure.
During the first 6 months of follow-up, the patient had no clinical symptoms or evidence of recurrence on X-rays done at monthly intervals and there was consolidation of the defect with no evidence of implant loosening or breakage (Fig. 8). Patient could perform all day-to-day functions with ease. Oxford Shoulder Score at 15 months post-procedure was 13 (minimum score 12).
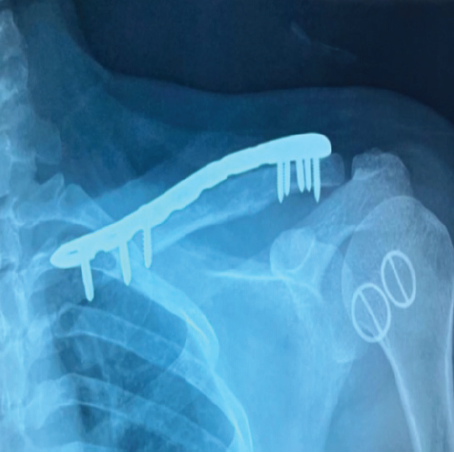
Figure 8: X-ray left shoulder anteroposterior view – at 6 months follow-up.
A meticulous post-operative protocol with vigorous post-operative rehabilitation ensured an excellent post-operative outcome at 15 months follow-up (Fig. 9).
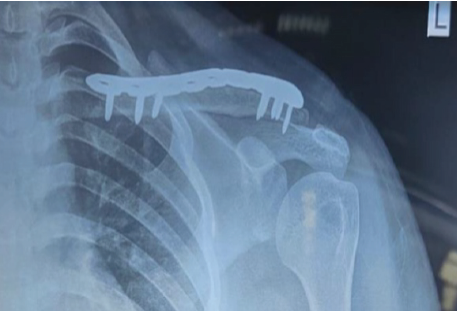
Figure 9: X-ray left shoulder anteroposterior view – at 15 months follow-up.
The incidence of aneurysmal bone cysts is 0.14/10 people, and eight out of ten patients are children and adolescents under 20 years of age. Clavicle neoplasms account for 1.01% of bone tumors, of which there exists no established incidence of aneurysmal bone cysts of clavicle in literature.
In a study conducted by Kaiser et al., patients with aneurysmal bone cysts of the clavicle were studied retrospectively. About 77% had aneurysmal bone cysts at the acromial end and presented with non-specific symptoms such as pain, swelling, and restricted shoulder mobility. Twelve patients were initially managed by curettage (with or without bone grafting) and one underwent resection. Seven patients who were managed with curettage presented with one or more instances of recurrence at an average of 6 months, of which two patients were managed with partial resection [4]. In a case report by Manish Chadha and Singh, an aneurysmal bone cyst of the lateral end of the clavicle was managed with total excision due to the size of the lesion at presentation that rendered the bone unsalvageable [5]. Rarely, aneurysmal bone cysts can occur in the medial end of the clavicle. Chitrangada Singh et al., reported one such case in a 14-year-old male child that was managed with extended curettage and hydroxyapatite allograft. Patient showed no recurrence in 2 years of follow-up [6]. In various other published case reports and series on aneurysmal bone cysts of the clavicle, management with excision was found to be the trend; as the rarity of the disease precluded early diagnosis [7,8,10]. Our case of aneurysmal bone cyst of the clavicle presented with non-specific symptoms and radiological findings that posed a diagnostic dilemma. Ultrasound-guided biopsy revealed it to be a “giant cell lesion” that, though specific, was inadequate to assume a definitive diagnosis. In an attempt to salvage the bone; and at the same time prevent any residual disease that could possibly lead to recurrence and repeated surgical interventions, we performed extended curettage with a high speed burr and chemical curettage with hydrogen peroxide. To augment healing of the defect, iliac autograft placement was done, along with plate augmentation using anatomical clavicle plate. Despite multiple imaging modalities and biopsy, a definitive diagnosis was established only postoperatively. This highlights the diagnostic limitations of current imaging and cytological tools in rare clavicular lesions.
For lesions treated with curettage, we also recommend the use of bisphosphonates (zoledronic acid in our case) postoperatively as their anti-inflammatory and anti-resorptive effect (osteoclast inhibition) aids in rapid radiological consolidation and, hence, early rehabilitation [10]. A strict and meticulous follow-up is necessary due to high recurrence rate to help in the early detection and prompt treatment. Our case was followed up with X-rays, VAS score, and OXFORD score [11] once a month for 6 months, once in 3 months till 1 year, and once in 6 months till 2 years. There was no evidence of recurrence and a significant improvement in VAS score and Oxford Shoulder Scores.
Rarity of the disease incidence at an uncommon location, excellent radiological and functional outcome, and meticulous follow-up plan along with the paucity of literature makes our case report a relevant document in orthopedic oncology; as it guides surgeons in the evaluation of lytic lesions of the clavicle. The possibility of aneurysmal bone cyst must be considered during the evaluation of lytic lesions of the clavicle so as to allow early detection and prompt treatment that will enable salvage of the bone. All possible efforts should be made to ensure no residual disease remains and patient should be followed up strictly; as the incidence of recurrence is fairly high and could potentially lead to partial or total excision of the bone, thus negating our initial attempts to salvage it.
To summarize, early detection by broadening the spectrum of differentials and successful surgical management of clavicle neoplasms can help salvage the shoulder joint.
Aneurysmal bone cysts of the clavicle are a rare clinical entity and warrant surgery at the earliest to achieve the best post-operative outcome. If detected early, aneurysmal bone cysts of the middle third of the clavicle can be managed successfully by extended curettage, bone grafting for the defect and augmentation plating.
Limitations
The report does not include comparison with other treatment modalities such as en bloc resection or embolization, making it difficult to assess the relative efficacy of the chosen surgical approach. A case series or an experimental study is needed to establish concrete evidence of the surgical and follow-up protocol.
References
- 1. Sciot R, Dorfman H, Brys P, Dal Cin P, De Wever I, Fletcher CD, et al. Cytogenetic-morphologic correlations in aneurysmal bone cyst, giant cell tumor of bone and combined lesions. A report from the champ study group. Mod Pathol 2000;13:1206-10. [Google Scholar] [PubMed]
- 2. Deventer N, Schulze M, Gosheger G, De Vaal M, Deventer N. Primary aneurysmal bone cyst and its recent treatment options: A comparative review of 74 cases. Cancers (Basel) 2021;13:2362. [Google Scholar] [PubMed]
- 3. Hartmann W, Harder D, Baumhoer D. Giant cell-rich tumors of bone. Surg Pathol Clin 2021;14:695-706. [Google Scholar] [PubMed]
- 4. Kaiser CL, Yeung CM, Raskin KA, Lozano-Calderon SA. Aneurysmal bone cyst of the clavicle: A series of 13 cases. J Shoulder Elb Surg 2019;28:71-6. [Google Scholar] [PubMed]
- 5. Chadha M, Singh AP. Aneurysmal bone cyst of the clavicle. Can J Surg 2008;51:E32-3. [Google Scholar] [PubMed]
- 6. Available from: https://www.researchgate.net/publication/339288897_aneurysmal_bone_cyst_of_medial_end_of_clavicle_a_rare_case_report [Last accessed on 2024 Nov 12]. [Google Scholar] [PubMed]
- 7. Dayma R, Sharma A, Gautam D, Ramachandran S. Aneurysmal bone cyst of the lateral end of clavicle in an eight year old child. Internet J Orthop Surg 2009;17:107 [Google Scholar] [PubMed]
- 8. Korkoman AJ, AlQahtani AA. Aneurysmal bone cyst of the clavicle: A case report. Int J Surg Case Rep 2023;110:108755. [Google Scholar] [PubMed]
- 9. Case Series: How to Recognize, Treat Aneurysmal Bone Cyst of Clavicle. Available from: https://advances.massgeneral.org/ortho/journal.aspx?id=1208 [Last accessed on 2024 Nov 12]. [Google Scholar] [PubMed]
- 10. Simm PJ, O’Sullivan M, Zacharin MR. Successful treatment of a sacral aneurysmal bone cyst with zoledronic acid. J Pediatr Orthop 2013;33:e61-4. [Google Scholar] [PubMed]
- 11. Oxford shoulder score (OSS). J Orthop Trauma 2006;20:S130-31. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Aneurysmal Bone Cyst-cloaked Codman’s Tumor in the Patella: Case Report of an Easily Misdiagnosed Entity
January 1, 2026 Aneurysmal Bone Cyst-cloaked Codman’s Tumor in the Patella: Case Report of an Easily Misdiagnosed Entity January 1, 2026 Aneurysmal Bone Cyst of Talus: Case Report of a Rare Presentation
January 1, 2026 Aneurysmal Bone Cyst of Talus: Case Report of a Rare Presentation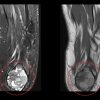 October 1, 2025 Young Female with Calcaneal Chondroblastoma & Secondary Aneurysmal Bone Cyst: Case Report
October 1, 2025 Young Female with Calcaneal Chondroblastoma & Secondary Aneurysmal Bone Cyst: Case Report September 1, 2025 Aneurysmal Bone Cyst of Talus: A Case Report
September 1, 2025 Aneurysmal Bone Cyst of Talus: A Case Report