
In the context of trauma to the elbow with a posterior defect of more than a quarter of the articular surface of the capitellum, filling the defect with bone graft and locking it with a posterior distal plate is advised to prevent radial engagement in the defect.
Dr. Mojahed Sakhnini, Department of Orthopaedic Surgery, Tzafon Medical Center, Tiberias, Israel. E-mail: mojahed.sakh@gmail.com
Introduction: Elbow dislocation is usually treated conservatively with a good outcome. When there is associated injury to the capitellum, “Osborne-Cotterill Lesion,” then the clinical course is less predictable and controversial. In this article, we attempt to define the critical point on the capitellum surface that, when breached, forebodes potential engagement of the radial head in the defect and imminent dislocation.
Case Report: We present two cases of fracture and fracture dislocation of the elbow with “Osborne-Cotterill lesion.” They were treated with fracture reduction and fixation. In the first case, a posterior plate was utilized for the olecranon, and in the second case, cannulated screws were employed for the capitellum fracture. In both cases, a posterior humeral plate was applied to counteract the “Osborne-Cotterill lesion” with bone grafting of the defect.
Conclusion: When the critical point of the capitellum is breached (roughly a quarter of the capitellar articular surface or less when the radial head is injured),we recommend bone grafting the defect and plating the posterior capitellum to impede potential dislocation.
Keywords: Elbow, Osborne-Cotterill lesion, dislocation, engagement, bone graft, critical point, instability, lateral ulnar collateral ligament.
In the literature, the “Osborne-Cotterill Lesion” is defined as a depression fracture in the capitellum caused by radial head dislocation impinging upon the capitellum, resulting in a crater [1,2]. The fragment is produced when the radial head dislocates laterally and posteriorly as it hits the capitellum at this specific location in a predicted manner [2,3]. The lesion could cause engagement of the radial head, and the radial head may become dislocated and remain stuck in that position, necessitating open reduction [4]. Surgical intervention that reanimates the lateral ulnar collateral ligament (LUCL) with reinsertion or reconstruction alone may potentially lead to instability, dislocation, or a limited range of motion [5,6]. We present a different approach to treat this enigmatic problem. We suggest bone grafting the “Osborne-Cotterill Lesion” and adding a posterior plate to secure the graft and further thicken the barrier against dislocation. We will discuss this strategy using two case studies and present a simple algorithm to help determine when to address the “Osborne-Cotterill Lesion surgically.”
Defining the critical point
The anatomy of the radiocapitellar joint is intriguing; there is a match between the radius of the radial head and the radius of the capitellum, as this joint performs a 3D motion: flexion-extension, pronation-supination, and translation. Extension could be accompanied by simultaneous supination movement and translation. For the radial head to dislocate, it must pass a critical point at the posterior edge of the capitellum. Passing that point, it could relocate back or engage a shallow depression in the capitellum. To decide where this critical point is, we hypothesize the following points:
- The diameter of the capitellum is the same as that of the radial head [7].
- The dislocation process entails a translation of the radial head and not only a pendulum movement of the radial head against the capitellum [8].
- The capitellum functional surface is inclined on average 45 degrees relative to the humerus [9].
- The hyaline cartilage of the capitellum-functioning surface, covers 180° (half of a full sphere).
- The radial head has an intrinsic translation movement of 1 radian up to the bisecting point of the capitellum when the posterior capsule is injured (following fracture or dislocation) [10,11].
These assumptions could be partly referred from literature and partly from observation and mechanical deduction [7,8,9,10,11]. Based on these assumptions, we can establish the safe zone, which indicates the distance the radial head travels before it passes the critical point.
In full extension, the posterior edge of the radial head passes this critical point (Fig. 1).

Figure 1: (a) Sagittal magnetic resonance imaging (MRI) cut for the capitellum and the radial head in extension. “α” angle represents 2 radians, and the orange arrow crosses at the critical point. “β” is the angle between the bisecting blue arrow and the orange arrow. (b) Sagittal MRI cut that demonstrates the safe zone, which is roughly equivalent to a quarter of the functional capitellar surface.
This is because the capitellum, being a half sphere, is anteriorly sloped. Due to the slope of the capitellum, the critical point forms a 45° angle between the center of the capitellum and a vertical line parallel to the humerus or a horizontal line parallel to the radial head in neutral full extension.
We define “a” angle as 2 radians (114.6°) of the capitellar sphere equal to the diameter of the radial head, which is the distance the anterior edge of the radius needs to pass before dislocating when it is in full extension. From “a,” we must take out “b” which represents the point where the shallow edge of the capitellum starts. To infer “b,” we make a basic geometric calculation based on the above assumptions, and we deduce that “b” is equal to 12°. Now, we calculate the residual distance the radial head must make to reach the critical point. 12° is 0.2 radians, leaving 1.8 radians for the radius to make from the original 2 radians. If we take the translation potential of the radial head following injury to the posterior capsule, this leaves us with 0.8 radians (“g” angle) up to the critical point. 0.8 radian is the safe zone. This distance equals roughly a quarter of the functioning capitellum surface (Fig. 2). Measuring the critical point should be done with a full profile of the radial bone, as this defines the middle of the radio-capitellar joint (Fig. 3).

Figure 2: A simple 2D model for radiocapitellar joint motion. (a) 90° of elbow flexion. (b) The elbow is in neutral extension. (c) One radian translation of the radial head following injury. (d) Following the “Osborne-Cotterill Lesion” of more than 0.8 radian, the radial head engages the lesion.

Figure 3: Consequential CT cut of intact radio-capitellar joint from lateral to medial (left to right). Critical point is defined with a full profile of the radius (c).
This safe zone could be breached in several scenarios as follows:
- Fracture of the anterior articular surface of the radial head, which leaves a less safe zone.
- Classic “Osborne-Cotterill Lesion” with encroachment of the depression in the capitellum more anteriorly up to or passing the critical point. This could potentially lead to a large “b” angle. If “b” is equal to 57°, then there is no safe zone, and full extension with 1 radian translation will cause an engagement of the radial head on the capitellar depression.
- A combination of radial head fracture and “Osborne-Cotterill Lesion.” If we lose a third of the anterior radial head (0.66 radian), then this will only leave little room for engagement (0.14 radian) [12,13].
- Posterior comminution fracture of the capitellum.
- Shear fracture of the capitellum (Fig.4).

Figure 4: X-ray that demonstrates a capitellar fracture. (Bryan and Morrey Type I). The radial head is engaged in the fracture site.
Case one
An 18-year-old patient fell from a bicycle and injured his right elbow. He was diagnosed with a fracture dislocation of the elbow (Fig. 5a). The elbow was reduced in the emergency room (ER), and a cast was applied (Fig. 5b). A subsequent computed tomography (CT) with 3D reconstruction revealed olecranon fracture with avulsion fracture of the LUCL and a posterior depression of the capitellum involving approximately a quarter of the articular surface – “Osborne-Cotterill Lesion” (Fig. 5c). The patient was offered surgery to fix the fracture and stabilize the elbow joint.

Figure 5: (a) X-ray of fracture dislocation of the right elbow. (b) X-ray of reduced elbow with posterior splint. (c) 3D reconstruction of the injury following reduction.
A posterior approach was utilized first, and the olecranon fracture was reduced and stabilized with a locked plate. Following this, a second lateral elbow approach with Kocher extension was utilized. LUCL was avulsed from its origin, and there was a depression fracture on the posterior edge of the capitellum. At this stage, we feared that mere ligament stabilization would not be enough to prevent radial head engagement; thus, we proceeded to fill the depression with bone allograft, and a plate was contoured and utilized to stabilize the construct. Two anchors were used to reattach the LUCL.
Following the surgery, the elbow was splinted for 1 week and then replaced with a dynamic elbow splint to allow for early range of motion (Fig. 6). Eight weeks following the surgery, the patient had a full range of motion and was able to return to their prior level of activities (Fig. 7).

Figure 6: X-ray images 1 week following the surgery. (a) AP X-ray showing the posterior plate at the distal lateral part of the humerus. b. Lateral X-ray demonstrating the distal edge of the plate increasing the safe zone.

Figure 7: The patient after a few weeks with a full range of motion. (a) Full stable extension with supination. (b) Full flexion.
Case two
A 45-year-old patient who fell from a ladder and injured his left elbow. In the ER, he was diagnosed with a fracture of the capitellum and trochlea. A CT scan with 3D reconstruction was performed to elucidate further the fracture and plan intervention (Fig. 8). The 3D reconstruction revealed posterior capitellar comminution (Fig. 9).

Figure 8: Computed tomography of the left elbow of the 2nd patient. (a) The cut demonstrates the posterior lesion in the capitellum laterally. (b) A more medial cut shows the trochlear fracture.

Figure 9: 3D reconstruction of the fracture involving the capitellum and trochlea with posterior comminution of trochlea inducing “Osborne-Cotterill-like Lesion”.
A temporary splint was used for pain control, and the patient was admitted for surgical intervention. The next day, the patient underwent surgery with a lateral elbow approach and distal Kocher extension. The proximal incision with partial brachioradialis release facilitated a deeper window for the trochlea. The trochlea was addressed first, followed by the capitellum, with reduction and provisional fixation using Kirchner wires, and then with canulated screws in the sagittal and coronal planes to maximize purchase and stability. A posterior fracture of the capitellar wall with comminution distally led us to add a posterior humeral plate advanced distally as close to the critical point as possible to add stability and counteract the potential engagement (Fig. 10). The patient was allowed early supervised range of motion 3 days following surgery. Post-operative X-rays taken before discharge showed a good reduction and a stable construct (Fig. 11). The patient was discharged after 5 days to ambulatory rehabilitation and was subsequently lost to follow-up.

Figure 10: Fluoroscopic images of the patient’s left elbow following reduction and fixation with cannulated screws. A posterior plate was utilized and advanced distally as far as possible to counteract engagement.

Figure 11: X-ray images of the patient’s left elbow at follow-up show a good outcome.
We present a new approach to “Osborne-Cotterill Lesion,” analyzing its impact and describing the best way to address it to minimize complications and optimize outcome. The radial head can translate posteriorly up to a critical point. We figure the distance to the critical point to be 1.8 times the radius of the capitellum. We assign the radial head a freedom of one radius translation in the extreme position of extension and supination in the context of injury to the posterior capsule, leaving a mere 0.8 radius, which is the safe zone. Based on our assumptions, the critical area can move further anteriorly, encroaching on the safe zone up to a point that the radial head is inherently unstable in functional positions. We suggest that when the capitellum loses 0.25 of its posterior cartilage, then an osseous reconstruction is mandatory. When an additional fracture occurs in the anterior radial head or the patient has joint laxity, a more liberal approach is warranted to address the “Osborne-Cotterill Lesion.” While several authors introduced variant approaches to enhance osseus stability in the context of posterolateral instability, including reduction [14], bone grafting [4], osteochondral allograft transplantation [15], and even prosthetic resurfacing [16], here we suggest a simple practical approach that helps reach stability with filling the defect with bone graft and utilizing a posterior plate to the capitellum to countereffect engagement. Our concept aligns with other biomechanical studies that refer to radial head translation following posterolateral capsule injury, which state approximately 11 mm of translation following injury to the LUCL and posterior capsule. This, in fact, is half of the mean radial head diameter (one radian) in accordance with our assumption [17].
The plate not only protects the reduction and locks the bone graft, but its bulk and position prevent the engagement, and the radial head must translate further to skip the plate, which increases the safe zone. This step should be contemplated whenever “Osborne-Cotterill Lesion” is found in the context of lateral elbow dislocation, fracture dislocation, or complex elbow fractures. Other elements of the injury should be addressed, including fractures and ligament avulsions. This will minimize the freedom of posterior translation of the radial head.
Our theory resembles the “On-Track/Off-Track” paradigm introduced by Itoi and associates [18,19], which discusses the stability concept of the shoulder in the context of an osseous defect in the glenoid and a Hill-Sachs lesion in the humeral head. Abduction and external rotation in the shoulder, parallel extension and supination in the elbow, and engagement happens easily with bipolar injury to the glenoid and the humerus, as is the case when the radial head loses its anterior lip, and the critical point of the capitellum moves anteriorly, leading to engagement. While off-track lesions are treated with remplissage to the humeral head or Latarjet procedure to the glenoid [20], the “Osborne-Cotterill Lesion” leading to the engagement is best treated with bone graft and plating, and the radial head fracture is either reduced and fixated or replaced. Interestingly, loss of more than 25% of the glenoid is typically treated with a bony procedure, such as the Latarjet procedure.
Another scenario where we would encounter radial engagement that needs to be addressed is capitellar fracture with posterior comminution. This could happen in the context of shear fractures of the capitellum elucidated through Dubberley’s classification of capitellar and/or trochlear fractures, specifically Type B [21]. The posterior comminution, even with articular reduction, could potentially lead to posterior engagement eventually, and it is addressed with bone grafting [22]. Furthermore, outcomes are inferior to Type A without posterior commination [23]. This is why it is better treated with an additional posterior locked plate [24]. Another interesting option is a shear capitellar fracture that leaves the radius engaged in without dislocation (Fig. 4).
We introduce an intuitive system to analyze the safe zone and help build a practical plan when the “Osborne-Cotterill Lesion” is recognized. If the safe zone is compromised and there is an accompanying fracture in the radial head, further minimizing the room for maneuver, then moving back the critical zone is recommended, employing grafting and plating, rather than just ligament stabilization or reconstruction. We assign a 25% safe zone, and if it is violated, then a bony procedure, including plating, is recommended. Our recommendations are based on multiple hypotheses that require further exploration in laboratory conditions and clinical settings. More evidence is needed to corroborate our assumptions. However, considering the rarity of this injury and the limited literature based on case reports and small series, we strongly advise re-evaluating the approach to treating “Osborne-Cotterill Lesion” and adopting our concept when treating similar injuries.
When encountering “Osborne-Cotterill Lesion” in the context of acute trauma to the elbow, a decision should be made regarding treating this defect when appropriate to prevent residual instability. We suggest grafting the defect and utilizing a posterior plate, along with reconstructing or re-attaching the LUCL to help stabilize the elbow.
References
- 1. Osborne G, Cotterill P. Recurrent dislocation of the elbow. J Bone Joint Surg Br 1966;48:340-6. [Google Scholar] [PubMed]
- 2. Somford MP, Van Den Bekerom MP, Gosens T, IJpma FF. The Osborne-Cotterill lesion: How an eponymous term arose and evolved. J Bone Joint Surg Am 2019;101:e81. [Google Scholar] [PubMed]
- 3. Jeon IH, Micic ID, Yamamoto N, Morrey BF. Osborne-cotterill lesion: An osseous defect of the capitellum associated with instability of the elbow. AJR Am J Roentgenol 2008;191:727-9. [Google Scholar] [PubMed]
- 4. Shekhbihi A, Reichert W. Engaging Osborne-Cotterill lesion as a cause of irreducible posterior dislocation of the radiocapitellar and ulnohumeral joints: A case report. J Orthop Rep 2022;1:100066. [Google Scholar] [PubMed]
- 5. Jeon IH, Min WK, Micic ID, Cho HS, Kim PT. Surgical treatment and clinical implication for posterolateral rotatory instability of the elbow: Osborne-Cotterill lesion of the elbow. J Trauma 2011;71:E45-9. [Google Scholar] [PubMed]
- 6. Alcid JG, Ahmad CS, Lee TQ. Elbow anatomy and structural biomechanics. Clin Sports Med 2004;23:503-17, vii. [Google Scholar] [PubMed]
- 7. Griswold BG, Steflik MJ, Adams BG, Hebert-Davies J, Tokish JM, Parada SA, et al. Radius of curvature of the radial head matches the capitellum: A magnetic resonance imaging analysis. JSES Int 2023;7:668-72. [Google Scholar] [PubMed]
- 8. Dunning CE, Duck TR, King GJ, Johnson JA. Quantifying translations in the radiohumeral joint: Application of a floating axis analysis. J Biomech 2003;36:1219-23. [Google Scholar] [PubMed]
- 9. Kang CN, Choi CH. The normal humero-capitellar angle in children; baumann angle and lateral humero-capitellar angle. Ewha Med J 1994;17:383-90. [Google Scholar] [PubMed]
- 10. Edwards DS, Arshad MS, Luokkala T, Kedgley AE, Watts AC. The contribution of the posterolateral capsule to elbow joint stability: A cadaveric biomechanical investigation. J Shoulder Elbow Surg 2018;27:1178-84. [Google Scholar] [PubMed]
- 11. Rotman D, Bokhari N, Wright A, Watts AC. The posterolateral ligament of the elbow: Anatomy and clinical relevance. J Shoulder Elbow Surg 2024;33:573-82. [Google Scholar] [PubMed]
- 12. Nalbantoglu U, Gereli A, Kocaoglu B, Aktas S, Turkmen M. Capitellar cartilage injuries concomitant with radial head fractures. J Hand Surg Am 2008;33:1602-7. [Google Scholar] [PubMed]
- 13. Claessen FM, Kachooei AR, Verheij KK, Kolovich GP, Mudgal CS. Outcomes of concomitant fractures of the radial head and capitellum: The “kissing lesion”. J Hand Microsurg 2016;8:100-5. [Google Scholar] [PubMed]
- 14. Vargas DG, Woodcock S, Porto GF, Gonzalez JC. Osborne-Cotterill lesion a forgotten injury: Review article and case report. Clin Shoulder Elb 2020;23:27-30. [Google Scholar] [PubMed]
- 15. Lee SJ, Bedford BB, Kim AH, Rahman OF, Zbeda RM. Elbow osteochondral allograft transplantation and lateral ulnar collateral ligament repair with internal brace: A case report. JBJS Case Connect 2022;12:e21. [Google Scholar] [PubMed]
- 16. Rotman D, Lievano JR, O’Driscoll SW. Prosthetic resurfacing of engaging posterior capitellar defects in recurrent posterolateral rotatory instability of the elbow. Clin Shoulder Elb 2023;26:287-95. [Google Scholar] [PubMed]
- 17. Guitton TG, Van Der Werf HJ, Ring D. Quantitative measurements of the volume and surface area of the radial head. J Hand Surg Am 2010;35:457-63. [Google Scholar] [PubMed]
- 18. Yamamoto N, Itoi E, Abe H, Minagawa H, Seki N, Shimada Y, et al. Contact between the glenoid and the humeral head in abduction, external rotation, and horizontal extension: A new concept of glenoid track. J Shoulder Elb Surg 2007;16:649-56. [Google Scholar] [PubMed]
- 19. Di Giacomo G, Itoi E, Burkhart SS. Evolving concept of bipolar bone loss and the Hill-Sachs lesion: From “engaging/non-engaging” lesion to “on-track/off-track” lesion. Arthroscopy 2014;30:90-8. [Google Scholar] [PubMed]
- 20. Itoi E. ‘On-track’and ‘off-track’shoulder lesions. EFORT Open Rev 2017;2:343-51. [Google Scholar] [PubMed]
- 21. Teng L, Zhong G. Surgical treatment of comminuted coronal shear fracture of distal humerus. Orthop Surg 2020;12:1439-47. [Google Scholar] [PubMed]
- 22. Tarallo L, Novi M, Porcellini G, Giorgini A, Micheloni G, Catani F. Surgical tips and tricks for coronal shear fractures of the elbow. Arch Orthop Trauma Surg 2021;141:261-70. [Google Scholar] [PubMed]
- 23. Marinelli A, Cavallo M, Guerra E, Ritali A, Bettelli G, Rotini R. Does the presence of posterior comminution modify the treatment and prognosis in capitellar and trochlear fractures? Study performed on 45 consecutive patients. Injury 2018;49:S84-93. [Google Scholar] [PubMed]
- 24. Gao X, Li H, Xue D, Pan Z, Zhang Y. Clinical outcomes of capitellar fractures with posterior comminution treated with Herbert screws combined with metacarpal locking plates. BMC Musculoskelet Disord 2023;24:937. [Google Scholar] [PubMed]

Related Articles in Journal of Orthopaedic Case Reports
 November 1, 2025 Surgical Treatment of Neglected Elbow Dislocation with the Box-loop Technique: A Case Report
November 1, 2025 Surgical Treatment of Neglected Elbow Dislocation with the Box-loop Technique: A Case Report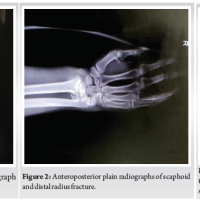 April 10, 2024 Terrible Triad of the Elbow with Ipsilateral Complete Triceps Tearing, Distal Radius and Scaphoid Waist Fracture: A Case Report
April 10, 2024 Terrible Triad of the Elbow with Ipsilateral Complete Triceps Tearing, Distal Radius and Scaphoid Waist Fracture: A Case Report December 10, 2023 Neglected Elbow Dislocation leading to Ankylosis of Elbow: A Case Report
December 10, 2023 Neglected Elbow Dislocation leading to Ankylosis of Elbow: A Case Report February 1, 2026 Closed Traumatic Dislocation of 2nd–4th Metatarsophalangeal Joints with Associated 5th Metatarsal Base Fracture: A Rare Case Report
February 1, 2026 Closed Traumatic Dislocation of 2nd–4th Metatarsophalangeal Joints with Associated 5th Metatarsal Base Fracture: A Rare Case Report