
An interference screw sinking during core decompression for avascular necrosis of the hip is a dreaded complication during surgery and this time, it was successfully retrieved using Schanz pins in a minimally invasive manner.
Dr. Darshan Temker, Department of Orthopaedics, All India Institute of Medical Sciences, Raipur - 492099, Chhattisgarh, India. E-mail: temker1997@gmail.com
Introduction: Interference screws are commonly used implants, particularly in arthroscopic cruciate ligament reconstruction, where they achieve fixation by compression and friction rather than by threads. We report a case of a sunken interference screw, used as a stopper and centralizer during core decompression and autologous adult live-cultured osteoblast (AALCO) injection for avascular necrosis (AVN) of the hip, which was successfully managed using a minimally invasive instrument-assisted retrieval technique.
Case Report: A 67-year-old male with bilateral hip AVN was posted for bilateral core decompression and AALCO injection. After track preparation and drilling of the necrotic area in the femoral head with an 8 mm reamer, an 8 mm interference screw was inserted before injection of the AALCO. The screw migrated into the femoral neck and became sunken, complicating retrieval. Using a combination of standard orthopedic operating room instruments, i.e., without specialised instruments for retained implant removal, the screw was retrieved without additional morbidity. The AALCO was injected as planned, and the patient had an uneventful post-operative recovery.
Conclusion: A sunken interference screw in the proximal femur is a rare but challenging intraoperative complication. Our retrieval method using readily available instruments offers a safe and reproducible solution in such scenarios.
Keywords: Avascular necrosis, interference screw, sunken screw, implant retrieval.
Avascular necrosis (AVN) of the femoral head is a progressive disorder that, when left untreated, leads to collapse of the femoral head and hip arthritis. Core decompression is a well-established joint-preserving modality of treatment in Ficat and Arlet Stage I and II AVN [1]. Recently, with the advent of biological augmentation methods, autologous adult live-cultured osteoblast (AALCO) has shown promise in improving outcomes by promoting bone regeneration [2,3]. The procedure involves two stages, the first being aspiration of 12 mL of bone marrow from the iliac crest and cultivation of mesenchymal stem cells with induction towards osteoblastic lineage at Regrow Biosciences Pvt Ltd, Mumbai, India. The second stage involves injecting the cultivated 48 million osteoblasts, 3–4 weeks later after a core decompression under fluoroscopic guidance.
To prevent backflow of the injected material following the decompression, an interference screw can be temporarily inserted at the mouth of the track in the lateral cortex of the proximal femur. Interference screws are widely used in arthroscopic knee surgeries, but complications such as breakage, migration, or burial are uncommon and almost never reported in the setting of hip surgery [4]. Interference screws have also evolved from metal screws to bioabsorbable screws [5].
We present a case in which a metal interference screw became sunken within the femoral neck during bilateral hip core decompression and AALCO injection, as shown in Fig. 1.
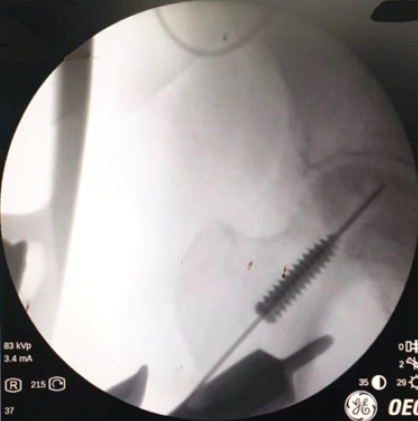
Figure 1: Interference screw sunken in the femoral neck.
We describe our technique for minimally invasive retrieval using standard operating room instruments found in an orthopedic operating room, thereby avoiding extensive exposure, need for specialised instruments and bone loss, allowing completion of the planned procedure.
A 67-year-old male presented with bilateral hip pain and restriction of daily activities for a duration of 12 months. There was no history of trauma, corticosteroid intake, alcohol abuse, or systemic illness. Clinical examination revealed pain during the hip range of motion and minimally restricted flexion, abduction, and internal rotation bilaterally. There were no fixed deformities and no limb length discrepancy.
Radiographs demonstrated sclerosis and cystic changes in both femoral heads. Magnetic resonance imaging confirmed AVN of bilateral femoral heads and was staged as Ficat and Arlet Stage II. The patient was counseled, and core decompression with AALCO injection was planned. One month before the procedure, bone marrow was harvested from the iliac crest, and osteoblasts were cultured.
Operative procedure
Through a lateral approach, a guide wire was placed under fluoroscopy into the necrotic area of the femoral head. An 8 mm reamer was used to drill over the guide wire. To prevent backflow of the injected material, an 8 mm metallic interference screw was introduced at the track opening. During insertion, the screw migrated into the femoral neck, and the full length of the screw was sunk.
Management
Direct attempts to grasp the screw risked enlarging the core tract. As shown in Fig. 2, gentle retrieval using the screwdriver over the guide wire was initially attempted.

Figure 2: Attempting removal with gentle counterclockwise screwing with a screwdriver.
This did not work as force is required to mate the screwdriver tip to the screw head, which would lead to further burial of the screw. Subsequently, a guide wire was bent to create a hook at the end and insertion across the interference was attempted (Fig. 3).

Figure 3: Attempting removal with a hooked guide wire.
This proved to be challenging as a large hook would not go across the screw and a small hook would not be able to get adequate purchase at the screw tip to be able to pull it back [6,7].
The next method that was attempted, as shown in Fig. 4 was to thread a thin 2.5 mm Schanz pin into the canal of the interference screw and pull it back.

Figure 4: Attempting removal with a Schanz pin.
This proved to be partially successful, and the screw was pulled back a certain distance. Following this, the Schanz pin was passed into the screw head and the threads of the Schanz pin engaged with the head of the screw and thus, the screw could be pulled out without the need for additional exposure, enlargement of the reaming track, or creation of a bone window (Fig. 5) [8]. The procedure was then completed and repeated on the contralateral side without complications.
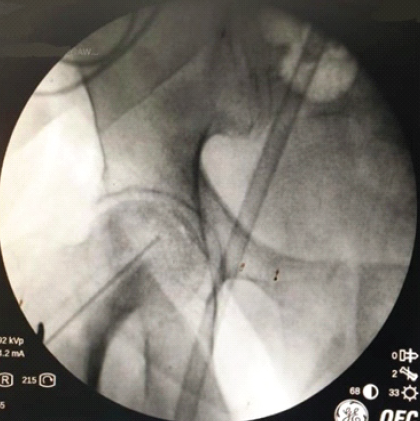
Figure 5: Screw successfully removed.
Outcome
Post-operative radiographs confirmed removal of the screw and satisfactory decompression tracts.
Interference screws are designed to provide secure fixation in ligament reconstruction by frictional engagement within bone tunnels. While complications such as migration, breakage, or intra-articular placement are described in knee and shoulder surgery, they are exceedingly rare in hip-preserving surgery [4].
In this case, the screw became sunken within the femoral neck during core decompression, posing a unique intraoperative challenge. Conventional options, such as enlarging the track or creating a cortical window, would compromise bone stock and potentially affect the efficacy of the decompression and grafting procedure [9]. Using a Schanz pin for removal has been described by Ebrahimpour et al., but not for an interference screw [8]. Other methods, such as inserting multiple guide wires, risked pushing the screw further as the interference screw has a narrow canal [10].
Our technique demonstrates that sunken screws can be retrieved using only standard orthopedic instruments in a minimally invasive manner, preserving bone and avoiding further morbidity. To the best of our knowledge, this is the first reported case of an interference screw complication during core decompression and AALCO injection managed successfully with such a method.
Limitations of this report include a single case and short-term follow-up. However, the technical relevance makes this report valuable for surgeons encountering similar intraoperative difficulties.
A sunken interference screw during hip core decompression is a rare but challenging intraoperative complication. Our retrieval method using standard instruments is safe, reproducible, and preserves femoral head integrity.
A sunken interference screw during hip core decompression can be retrieved safely through the same tract using a thin Schanz pin to engage the screw’s head and back it out under fluoroscopy—avoiding cortical windows, preserving bone stock, and allowing the planned AALCO injection to proceed.
References
- 1. Rajagopal M, Balch Samora J, Ellis TJ. Efficacy of core decompression as treatment for osteonecrosis of the hip: A systematic review. Hip Int 2012;22:489-93. [Google Scholar] [PubMed]
- 2. Palekar G, Bhalodiya H, Archik S, Trivedi K. Retrospective study on implantation of autologous-cultured osteoblasts for the treatment of patients with osteonecrosis of the femoral head. Orthop Res Rev 2021;13:15-23. [Google Scholar] [PubMed]
- 3. Patro BP, Jeyaraman N, Jeyaraman T, Das G, Nallakumarasamy A, Jeyaraman M. Efficacy of autologous adult live-cultured osteoblast (AALCO) implantation in avascular necrosis of the femoral head: A mid-term outcome analysis. Indian J Orthop 2024;58:1053-63. [Google Scholar] [PubMed]
- 4. Kramer DE, Kalish LA, Kocher MS, Yen YM, Micheli LJ, Heyworth BE. Complications of bioabsorbable tibial interference screws after anterior cruciate ligament reconstruction in adolescents. Orthop J Sports Med 2020;8:2325967120904010. [Google Scholar] [PubMed]
- 5. McGuire DA, Barber FA, Elrod BF, Paulos LE. Bioabsorbable interference screws for graft fixation in anterior cruciate ligament reconstruction. Arthroscopy 1999;15:463-73. [Google Scholar] [PubMed]
- 6. Tomar L, Govil G, Dhawan P. Incarcerated cannulated cancellous screw removal during total hip arthroplasty with a novel trick: A case report. Malays Orthop J 2021;15:128-31. [Google Scholar] [PubMed]
- 7. Hak DJ, McElvany M. Removal of broken hardware. J Am Acad Orthop Surg 2008;16:113-20. [Google Scholar] [PubMed]
- 8. Ebrahimpour A, Biglari F, Sadighi M, Pesántez R. How to extract a broken cephalomedullary nail safely? A case presentation and review of the literature. Acta Orthop Traumatol Turc 2021;55:362-6. [Google Scholar] [PubMed]
- 9. Kyung MG, Park C. Removal of broken syndesmotic screw with minimal bone defects in Korea: A case report. J Trauma Inj 2023;36:265-8. [Google Scholar] [PubMed]
- 10. Middleton RG, McNab IS, Hashemi-Nejad A, Noordeen MH. Multiple guide wire technique for removal of the short distal fragment of a fractured intramedullary nail. Injury 1995;26:531-2. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Total Hip Arthroplasty in Lubumbashi (DR Congo), Outcomes in a Resource-Limited Setting
March 1, 2026 Total Hip Arthroplasty in Lubumbashi (DR Congo), Outcomes in a Resource-Limited Setting March 1, 2026 Day-Care Direct Anterior Total Hip Arthroplasty in Urban India: Patient Education, Apprehensions, and Outcomes
March 1, 2026 Day-Care Direct Anterior Total Hip Arthroplasty in Urban India: Patient Education, Apprehensions, and Outcomes March 1, 2026 Clinical and Radiological Outcomes of Pediatric Femoral Neck Fractures Treated with Surgical Internal Fixation: A Retrospective Case Series
March 1, 2026 Clinical and Radiological Outcomes of Pediatric Femoral Neck Fractures Treated with Surgical Internal Fixation: A Retrospective Case Series January 1, 2026 Early Outcomes of Screwless Press-fit Acetabular Cups in Uncemented Total Hip Arthroplasty: A Prospective Study from Eastern India
January 1, 2026 Early Outcomes of Screwless Press-fit Acetabular Cups in Uncemented Total Hip Arthroplasty: A Prospective Study from Eastern India