
When planning surgical fixation for a sternal body fracture, the incorporation of thoracoscopic assistance can be advantageous. A low-profile yet robust titanium locking plate can be utilized in a railroad technique for the fixation of transverse fractures. The novel technique of fixation.
Dr. Deepak D Chitragar, Department of Orthopaedics, Devadoss Multi-Speciality Hospital, Madurai, Tamil Nadu, India. Email: drdeeppak@gmail.com
Introduction: Sternal fracture is a common complication of chest trauma but has a low incidence. Various treatments have been developed to reconstruct sternal fractures. Among these approaches, analgesia, corset fixation, and open reduction with wiring or plate internal fixation have been suggested. The use of newly developed minimally invasive plate osteosynthesis is a feasible method. In this study, we report a case involving a 31-year-old young man with a sternal fracture accompanied by a small amount of lung contusion. All procedures including retro-sternal dissection and fracture reduction with placement of the dual plate as railroad technique were performed using video-assisted thoracoscopic surgery. The minimally invasive thoracoscopic technique provided effective repair and rigid fixation with immediate relief from intractable chest pain that had persisted before surgery. The postoperative recovery was good. No pneumothorax or complications such as chest pain, paresthesia, or wound infection were observed at the 6-month follow-up visit. This case describes a novel method for internal fixation of sternal fractures under thoracoscopic assistance.
Case Report: A 31-year-old male sustained injuries from a road traffic accident on May 16, 2024, and initially received treatment at a nearby government hospital. Two days later, he presented to our facility with chest pain and injuries to his right leg, wrists, and forearm. Physical examination revealed sutured wounds on the right wrist and elbow, along with external fixation on the right leg. Due to the persistence of chest pain, a computed tomography scan was performed, which revealed a displaced sternal body fracture. The cardiothoracic vascular surgery team recommended surgical fixation because of the displacement and ongoing chest pain. On May 20, surgery was conducted by an orthopedic surgeon using a minimally invasive technique with video-assisted thoracoscopic assistance to ensure proper visualization and protection of vital structures during fixation with two long 3.5 mm pre-bent titanium locking plates using the railroad technique. Care was taken to ensure that the screws did not excessively penetrate the posterior cortex, which was confirmed through thoracoscopy. The post-operative recovery was uneventful, with significant improvement in chest pain noted at the 6-week follow-up.
Conclusion: This case suggests that minimally invasive fixation with video-assisted thoracoscopy offers faster recovery, shorter hospitalization, and reduced tissue damage, ensuring proper reduction in sternal fractures. The low-profile 3.5 mm titanium locking plate using the railroad technique is an effective option for managing transverse sternal fractures.
Keywords: Sternal fracture, thoracoscopically assisted osteosynthesis, locking plate.
Sternal fractures are rare, making up <0.5% of all fractures and occurring in 3–8% of blunt trauma cases, mainly from motor vehicle accidents. Most are transverse, with manubrial and xiphoid fractures being less common [1]. Morbidity and mortality depend on concurrent internal thoracic organ injuries, with mortality rates between 4% and 45% [1]. Associated injuries are frequent: Rib (up to 72%), thoracic vertebra (32%), scapula (16%), clavicle (10%), pulmonary contusion (up to 54%), and cardiac injury (up to 25%) [2].
Most isolated sternal fractures have a favorable prognosis and over 95% are managed conservatively. Surgical intervention is reserved for unstable patterns, displacement, persistent deformity or pain, thoracic instability, respiratory compromise, or non-union [3].
Various fixation methods for sternal fractures are documented, with wiring and plating being the most common. Steel wire fixation remains simple and commonly used but can suffer from loss of tensile strength and wire cut-out, especially in transverse fractures. Several sources document these limitations, noting that wire techniques may lead to pseudoarthrosis and sometimes require removal due to discomfort or complications [4].
Operative stabilization using double 3.5 mm locking compression plates (LCP) offers excellent long-term outcomes and rigid fixation with minimal sternum exposure, resulting in low postoperative complications. However, 27% of patients required a second procedure for implant removal. Locking plates enhance stability and preserve periosteal blood supply, which is crucial for healing [5].
Biomechanical and clinical studies, including recent case reports and reviews, confirm that plating (especially with locking plates) leads to superior stability, better functional recovery, less post-operative pain, and fewer complications versus wire-only fixation [6].
Thoracoscopy is crucial for minimally invasive repair of sternal fractures, allowing surgeons to visualize the fracture site through a small incision. This technique enables precise placement of fixation devices, stabilizing the sternum while minimizing tissue damage and promoting faster recovery compared to open surgery [7,8].
These reports emphasize the technique’s effectiveness in managing difficult cases of posteriorly displaced or unstable fractures including non-union [7].
The technique improves visualization of the fracture site and adjacent structures, allowing for careful dissection, precise implant placement, and efficient management of complex injury. It also helps avoid iatrogenic injury to vital thoracic structures and supports faster patient recovery [9].
To date, no documented cases exist of sternal fracture fixation using thoracoscopic assistance by orthopedic surgeons. This case report addresses a significant gap in the literature on surgical techniques for these rare injuries, which are typically treated conservatively. We present a 31-year-old male with a transverse sternal body fracture and minor lung contusion, successfully treated with minimally invasive plate osteosynthesis under thoracoscopic guidance. The procedure involved retrosternal dissection and dual plate placement using the railroad technique, providing effective repair and immediate relief from chest pain. The patient’s recovery was smooth, with no complications. This case highlights the benefits of thoracoscopic assistance and a low-profile 3.5 mm titanium locking plate system in managing sternal fractures, contributing valuable insights to the field.
We present a case of 31-year-old male who sustained injury in Road Traffic Accident on May 16, 2024; the patient was initially received and treated in nearby district hospital for complains of chest pain, injury over right leg, B/L wrist, forearm, no history of loss of consciousness, ear, nose, and throat bleed, vomiting noted, Glasgow Coma Scale was 15/15, wound debridement and external fixator applied for comminuted fracture both bone lower one third in right leg, suturing of contused lacerated wound after proper wound wash. After 2 days, the patient came to our hospital for further management; on examination, we found sutured wound with external fixator over the right leg, other sutured wound over the body, patient complained of pain over chest, he had tenderness over sternum with normal breathing pattern; hence, we suspected of chest injury and took computed tomography scan; surprisingly, we found fracture in the upper part of sternal body with displacement, with no other rib fracture nor vertebral fracture with minimal lung contusion (Fig. 1), we also noted undisplaced fracture of right radial styloid process and segmental fibula fracture with comminuted distal third tibia fracture.
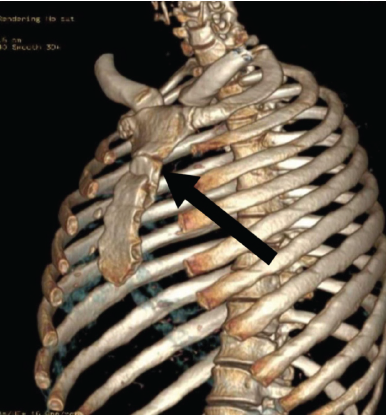
Figure 1: Computed tomography scan of the chest showing the displaced upper third of the body of sternum.
This type of injury is rare and is typically managed conservatively; however, due to the patient’s persistent chest pain, we sought the opinion of the cardiothoracic vascular surgery (CTVS) team. They recommended surgical fixation because the fracture was displaced and associated with ongoing chest pain. The CTVS team advised using thoracoscopic-assisted fixation to enhance visualization of the underlying vital structures and ensure proper reduction of the fracture.
Surgery was scheduled for May 20, 2024. The patient was positioned supine on the operating table under general anesthesia, utilizing a fluoroscopy-compatible table with support beneath the shoulder blades (Fig. 2).
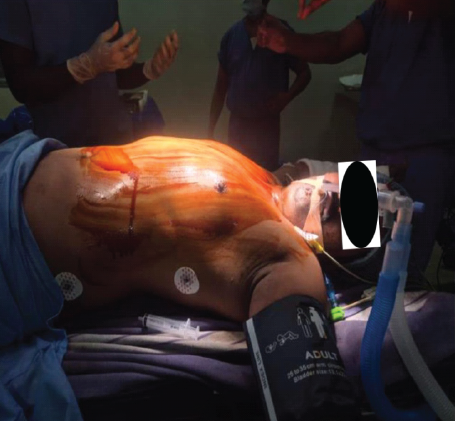
Figure 2: Positioning of the patient on operating table.
After the surgical site was prepared and draped, the CTVS team performed thoracoscopy through three portals to visualize the displaced fracture and any adhesions (Fig. 3).
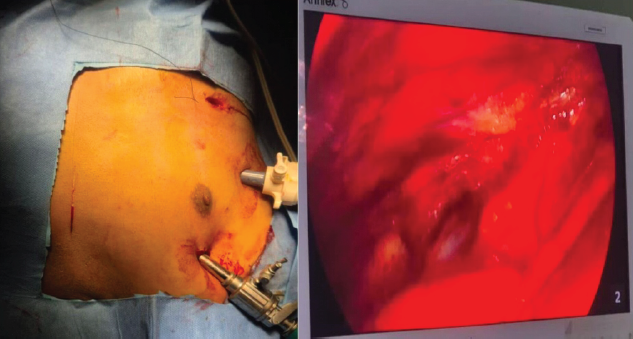
Figure 3: Video-assisted thoracoscopy through 3 portals.
They meticulously removed the adhesions while protecting the underlying vital structures (Vid). A 6–-8 cm straight incision was made over the fracture site, which was opened in layers to access the fracture. After cleaning the fracture ends, we encountered difficulty in reducing the fracture due to the inability to use forceps or retractors. Consequently, we opted to place a 3.5 mm Schanz screw in the proximal fragment and applied traction with a periosteal elevator to facilitate reduction under thoracoscopic guidance (Fig. 4).
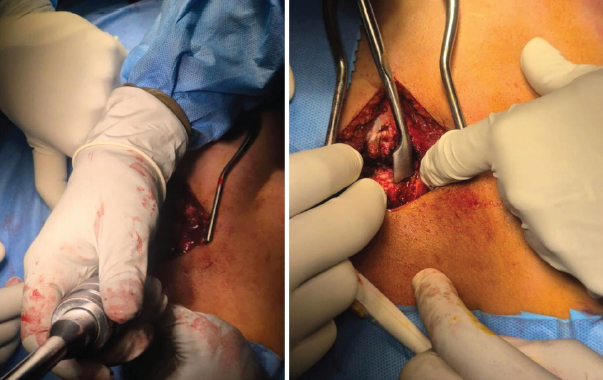
Figure 4: Reduction of fracture by Schanz screw and periosteal elevator.
The reduction was stabilized with K-wires. We then decided to use two low-profile 3.5 mm titanium locking plates in a railroad technique, pre-bending them to match the contour of the sternum (Fig. 5).
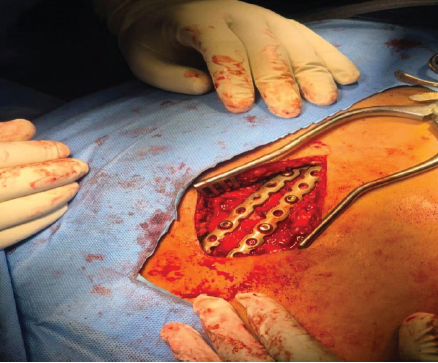
Figure 5: Railroad technique using prebent 2 low-profile 3.5 mm titanium locking plate fixation of transverse fracture of sternum.
The plates were initially secured with cortical screws, followed by locking screws bicortically, while ensuring that drilling was performed cautiously and checked under thoracoscopy to avoid irritation of underlying structure (Vid). Final reduction was deemed satisfactory and confirmed through fluoroscopy and thoracoscopy. The wound was closed in layers and stapled. The post-operative period was uneventful, and the patient was able to sit upright the following day. Sutures were removed on 12th postoperative day, and follow-up X-rays (Fig. 6) showed that the implants were in good position.
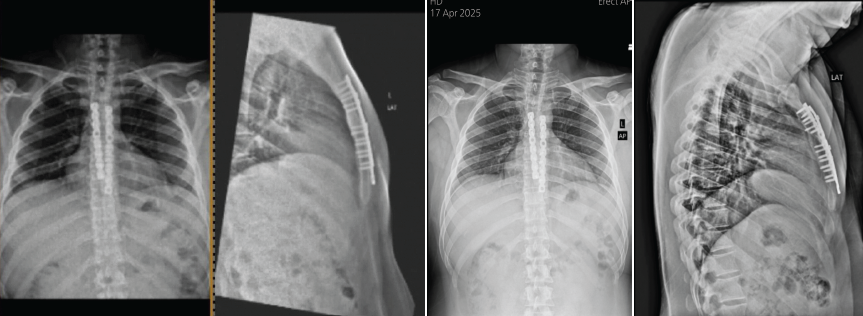
Figure 6: Final check xray and 1yr follow up x ray.
The patient was advised to perform respiratory exercises and wear a rib binder for support. At 6-month follow-up, the patient relieved of chest pain and was functionally doing well.
Sternal fractures are rare, comprising <0.5% of all fractures and occurring in 3–8% of blunt trauma cases, primarily due to direct blunt trauma from motor vehicle accidents. Most are transverse fractures, while manubrial and xiphoid fractures are less frequent. The morbidity and mortality associated with these injuries depend significantly on concurrent internal thoracic organ injuries, with mortality rates ranging from 4% to 45%. Common associated injuries include vertebral, rib, clavicular, and scapular fractures, as well as pulmonary contusions and cardiac injuries. Severe chest pain and concomitant injuries can lead to respiratory insufficiency and organ failure. Over 95% of sternal fractures are managed conservatively.
Conservative treatment of sternal fractures can lead to non-union, resulting in false joints and overlap deformities. Surgical intervention is recommended for selected cases, especially in instances of unstable fractures, thoracic wall instability, fracture displacement, persistent dislocation, sternal deformity, respiratory insufficiency, compression of mediastinal organs, or associated organ injury, severe pain, and non-union [1,2,3,10].
Various fixation methods for sternal fractures have been documented in the literature, with wiring and plating being the most commonly employed techniques. While steel wire fixation is straightforward, it can occasionally lead to loss of tensile strength or wire cut-out effects (naoko). Operative stabilization of sternal fractures using double 3.5 mm LCP provides excellent long-term functional outcomes and is considered a suitable option for internal fixation. This method offers rigid and stable fixation with minimal exposure of the sternum, leading to a low rate of post-operative complications; however, 27% of patients required a second procedure for implant removal. The advantages of using locking plates include enhanced stability and preservation of periosteal blood supply, which are critical for effective healing [4,5,6,8,11,12].
Thoracoscopy is essential for minimally invasive surgical repair of sternal fractures, enabling surgeons to visualize the fracture site through a small chest incision. This technique allows for the precise placement of fixation devices, stabilizing the fractured sternum while minimizing tissue damage and promoting quicker recovery than traditional open surgery. Key advantages include enhanced visualization for accurate assessment, reduced tissue trauma from smaller incisions, and the ability to identify associated injuries. This approach also leads to less post-operative pain, fewer complications, quicker recovery, and shorter hospital stays compared to open surgery. Thoracoscopy improves cosmetic outcomes and enables easier management of concomitant thoracic injuries during fixation procedures. It is particularly beneficial for managing displaced or unstable fractures and cases of non-union, facilitating effective surgical intervention [1,7,9,13].
To date, there have been no documented cases of sternal fracture fixation utilizing thoracoscopic assistance by orthopedic surgeons in any orthopedic journal. This case report is significant as it fills a critical gap in the literature regarding surgical fixation techniques for these rare injuries, which are often managed conservatively. A 31-year-old male with a transverse sternal body fracture and a minor lung contusion treated through minimally invasive plate osteosynthesis under thoracoscopic guidance. The procedures included retrosternal dissection and dual plate placement using the railroad technique, successfully providing effective repair and immediate relief from persistent chest pain. The patient’s postoperative recovery was smooth, with no complications observed. This case underscores the potential benefits of thoracoscopic assistance for internal fixation of sternal fractures. In addition, it highlights the advantages of a low-profile 3.5 mm titanium locking plate system in managing such injuries. By documenting this novel approach, we aim to contribute valuable insights into the management of sternal fractures and encourage further exploration of thoracoscopic techniques in orthopedic surgery.
The findings from this case indicate that for patients with sternal fractures who require expedited post-operative recovery, a brief hospitalization, and minimal incisional trauma, minimally invasive techniques combined with video-assisted thoracoscopic surgery are superior. This approach minimizes damage to adjacent vital structures while ensuring proper reduction of the fracture. The utilization of a low-profile 3.5 mm titanium locking plate system using the railroad technique may provide an effective strategy for managing transverse sternal fractures. However, it is important to note that this study is limited as it is based on a single case involving a middle-aged patient. Therefore, further research is warranted to establish the efficacy and advantages of thoracoscopy in the treatment of sternal fractures more broadly.
This novel technique of video-assisted thoracoscopic minimal invasive method of fixation of transverse fracture of the sternal body using low-profile 3.5 mm titanium locking plate as railroad technique facilitates rapid recovery, minimizes incisional trauma, and safeguards vital structures, ensuring proper reduction of fracture.
References
- 1. Klei DS, De Jong MB, Öner FC, Leenen LP, Van Wessem KJ. Current treatment and outcomes of traumatic sternal fractures-a systematic review. Int Orthop 2019;43:1455-64. [Google Scholar] [PubMed]
- 2. Şimşek S, Özmen CA, Onat S. Morbidity and mortality associated with fracture of the sternum due to blunt trauma, by fracture type and location. Radiol Bras 2022;55:167-72. [Google Scholar] [PubMed]
- 3. Christian AB, Grigorian A, Nahmias J, Duong WQ, Lekawa M, Joe V, et al. Comparison of surgical fixation and non-operative management in patients with traumatic sternum fracture. Eur J Trauma Emerg Surg 2022;48:219-24. [Google Scholar] [PubMed]
- 4. Zhao Y, Yang Y, Gao Z, Wu W, He W, Zhao T. Treatment of traumatic sternal fractures with titanium plate internal fixation: A retrospective study. J Cardiothorac Surg 2017;12:22. [Google Scholar] [PubMed]
- 5. Kalberer N, Frima H, Michelitsch C, Kloka J, Sommer C. Osteosynthesis of sternal fractures with double locking compression plate fixation: A retrospective cohort study. Eur J Orthop Surg Traumatol 2020;30:75-81. [Google Scholar] [PubMed]
- 6. Kar BK, Behera S, Kashyap N, Dash RN, Dhaka R. A devastating chest injury: A case report. J Orthop Case Rep 2025;15:107-12. [Google Scholar] [PubMed]
- 7. Azumi T, Sasaki H, Tamaoka T, Maruno F. Efficacy of thoracoscopic assistance using a mesh plate for nonunion of the sternal fracture: A case report. JOS Case Rep 2024;3:122-6. [Google Scholar] [PubMed]
- 8. Ahmed M, Khatib MN, Roopashree R, Kaur M, Srivastava M, Barwal A, et al. Effectiveness of sternal wiring versus plating on operative and postoperative recovery metrics in sternal fractures and sternotomies: A systematic review and meta-analysis. Curr Probl Surg 2025;65:101728. [Google Scholar] [PubMed]
- 9. Xia H, Zhu D, Li J, Sun Z, Deng L, Zhu P, et al. Current status and research progress of minimally invasive surgery for flail chest (Review). Exp Ther Med 2020;19:421-7. [Google Scholar] [PubMed]
- 10. Armstrong BA, Lorch SM, Diaz JJ. Sternal fracture management. Curr Probl Surg 2025;64:101725. [Google Scholar] [PubMed]
- 11. Groh J, Kern F, Schenderlein A, Krause J, Perl M, Schulz-Drost S. Traumatic fractures of the sternum – typical distribution and need for subgroups within AO and OTA classification system? Eur J Trauma Emerg Surg 2025;51:234. [Google Scholar] [PubMed]
- 12. Doyle JE, Diaz-Gutierrez I. Traumatic sternal fractures: A narrative review. Mediastinum 2021;5:34. [Google Scholar] [PubMed]
- 13. Ahmed K, Nady MA. Sternal reconstruction using locking compression plates (LCP): Our experience in Egypt, a case series. J Cardiothorac Surg 2020;15:224. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2025 A Prospective Study Comparing the Functional Outcomes of Complex Tibial Plateau Fractures Using Computed Tomography-based Three-column Theory Versus X-Ray-based Schatzker Classification Treated with Open Reduction with Locking Compression Plates
December 1, 2025 A Prospective Study Comparing the Functional Outcomes of Complex Tibial Plateau Fractures Using Computed Tomography-based Three-column Theory Versus X-Ray-based Schatzker Classification Treated with Open Reduction with Locking Compression Plates September 1, 2025 Rare Periprosthetic Fractures Following Oxford Unicompartmental Knee Arthroplasty: A Case Series of Supracondylar Femoral and Proximal Tibial Fractures
September 1, 2025 Rare Periprosthetic Fractures Following Oxford Unicompartmental Knee Arthroplasty: A Case Series of Supracondylar Femoral and Proximal Tibial Fractures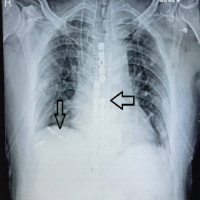 June 1, 2025 A Devastating Chest Injury: A Case Report
June 1, 2025 A Devastating Chest Injury: A Case Report October 1, 2024 Outcome Analysis of Fixed angle Locking Plate in Comminuted Patella Fractures: A Single-center Prospective study from South India with Early Results
October 1, 2024 Outcome Analysis of Fixed angle Locking Plate in Comminuted Patella Fractures: A Single-center Prospective study from South India with Early Results