
This case emphasizes individualized surgical planning and decision-making in windswept elbow deformity following trauma, with dome osteotomy as a safe, reliable corrective procedure.
Dr. Abhinav Singla, Department of Orthopaedics, Government Medical College and Hospital, Chandigarh, India. Email: docabsingla@gmail.com
Introduction: Windswept deformity of the elbow, defined as cubitus varus on one side and cubitus valgus on the contralateral side, is exceptionally rare, particularly in post-traumatic settings. The majority of published literature focuses on windswept deformities of the lower limbs, with almost no evidence-based guidelines for upper limb deformities.
Case Report: An 8-year-old male sustained bilateral elbow injuries in separate falls, leading to an untreated cubitus varus deformity of the left elbow (carrying angle −15°, Baumann’s angle 82°) and a cubitus valgus deformity of the right elbow (carrying angle +20°). The child presented 18 months after the initial trauma due to pandemic-imposed restrictions, with parental concern primarily for cosmesis of the left elbow. Dome osteotomy was performed on the left humerus using a posterior approach with crossed K-wire fixation. The right elbow was managed conservatively due to preserved function and accepted cosmesis. Rehabilitation commenced at 3 weeks, and follow-up over 18 months demonstrated excellent cosmesis and function (Mayo Elbow Performance Score 95, Disabilities of Arm, Shoulder, and Hand score 8). No lateral condylar prominence or recurrent deformity was observed.
Conclusion: This is a rare report of a bilateral windswept elbow deformity. Dome osteotomy offers multiplanar correction with superior cosmesis and biomechanical restoration. Population-based carrying angle norms provide valuable guidance in planning correction when contralateral anatomy is unavailable. This case highlights the importance of individualized surgical decision-making, meticulous planning, and patient-centered care. Furthermore, it highlights the acceptance of a valgus deformity at the elbow as opposed to a varus deformity.
Keywords: Windswept deformity, cubitus valgus, cubitus varus, elbow angular deformity, Dome osteotomy
Windswept deformity is most commonly described in the lower limbs, characterized by valgus deformity on one side and varus deformity on the contralateral limb [1]. Reports of this phenomenon in the upper extremities are extremely rare, with scarce literature providing guidance for management. Etiologies include congenital skeletal dysplasia, metabolic bone disease, trauma, and idiopathic deformities [1,2]. Cubitus varus, or “gunstock deformity,” is the most frequent complication following supracondylar humeral fractures in children. Despite being considered largely cosmetic, untreated cubitus varus can predispose to posterolateral rotatory instability, abnormal stress distribution, degenerative changes, and tardy ulnar nerve palsy [3]. Cubitus valgus deformity, on the other hand, is often secondary to non-union or growth arrest of the lateral condyle and carries risks of progressive deformity and neurological complications [4]. Post-traumatic bilateral symmetrical elbow deformity has been previously described in the literature, with varus more common than valgus deformity, with most patients having skeletal dysplasia and chromosomal abnormalities [5,6,7,8]. In the context of bilateral deformity, surgical planning becomes especially challenging. Contralateral anatomy is often used as a reference for correction; however, this was not possible in our case. This report describes the evaluation, surgical correction, and outcomes of a child with bilateral deformities resulting from untreated bilateral elbow trauma.
An 8-year-old boy presented with progressive deformity of both elbows (Fig. 1), first noticed after a fall on an outstretched hand 18 months prior (left elbow) and again 12 months prior (right elbow). Both injuries were initially managed traditionally with massage and splints due to a lack of access to orthopedic care during the COVID-19 lockdowns. No radiographs were obtained at that time.

Figure 1: Clinical image of the windswept deformity.
The primary parental concern was cosmetic deformity of the left elbow, though the child denied pain or limitation in daily activities. Developmental history was normal, with no family history of skeletal dysplasia or metabolic bone disease.
Clinical examination
- Left Elbow: Irregularity of medial and lateral epicondylar ridges present, carrying angle −15°, fixed varus deformity, Baumann’s angle 82°, range of motion (ROM): flexion 15–120°, supination 80°, and pronation 70°
- Right Elbow: Irregularity of medial and lateral epicondylar ridges present, 3-point bony relationship disturbed, carrying angle +20°, valgus alignment, ROM: flexion 0–100°, full supination and pronation, and no instability
- No tenderness, instability, or neurovascular deficits were noted in either elbow.
Radiology
Plain radiographs (Fig. 2) revealed a distal humeral varus deformity with internal rotation on the left and a mild valgus alignment on the right. No evidence of growth plate arrest was observed.
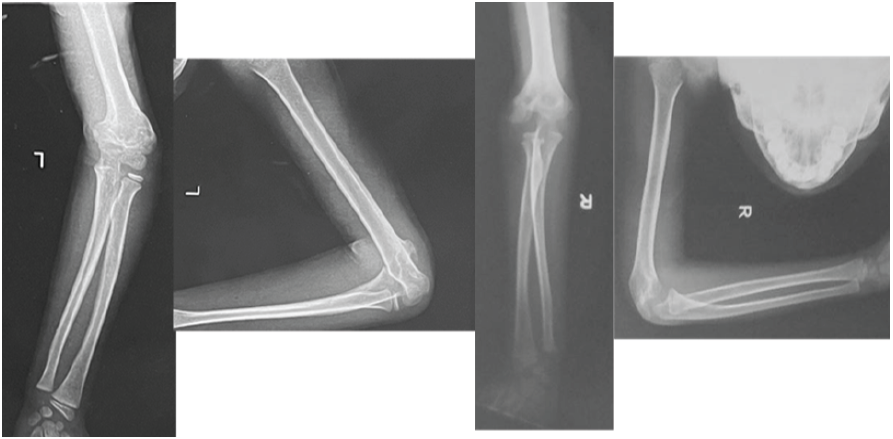
Figure 2: Pre-operative radiographs of both elbows.
Surgical technique
The child underwent dome osteotomy of the left distal humerus. Dome supracondylar osteotomy was performed as described by Tien et al. [9]. A posterior midline incision was given, and the triceps aponeurosis flap was raised. The center of the dome was defined as the point where the midline axis meets the margin of the olecranon fossa and was labeled as “O.” The line OA was taken as the base of the segment, and a second line, “OB,” was drawn from point O to form an angle equal to the planned correction. The radius of the dome was formed by the length of line OB (Fig. 3). Drill holes were made using 2 mm K-wire along the dome, and osteotomy was completed using a quarter-inch osteotome. The distal segment was rotated so that point A came to lie at the position of point B (Fig. 3). The distal fragment was rotated until 10° of valgus alignment was achieved, referencing normative carrying angle data (mean pediatric carrying angle 10.3°) [10,11,12]. Fixation was performed using two crossed K-wires (Fig. 4), and an above-elbow plaster slab was applied for 3 weeks.
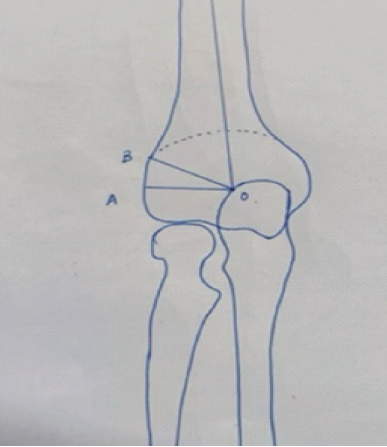
Figure 3: Depiction of the dome osteotomy.

Figure 4: Post-operative radiograph of the dome osteotomy.
Post-operative rehabilitation
The slab was maintained for 3 weeks, with initiation of passive range-of-motion exercises thereafter. K-wires were removed at 4 weeks. Full active mobilization was commenced at 6 weeks, and the patient was followed regularly with radiographs at 6 weeks, 3 months, 6 months, 12 months, and 18 months (Fig. 5).

Figure 5: Healed dome osteotomy.
As described in a case of bilateral cubitus valgus by Pei Ern Ngo, since symptoms are often mild and do not significantly affect a patient’s function, observation alone is the standard treatment with a good functional outcome in patients with cubitus valgus. Surgical management is usually indicated in cases of limitation in the range of movement, persistent pain, or for cosmetic reasons [13]. The decision to treat the right elbow cubitus valgus deformity conservatively was made since no cosmetic concerns or limitation of function were present.
Outcome
At 18 months:
- Left Elbow: Carrying angle +10°, Mayo Elbow Performance Score (MEPS) 95, Disabilities of Arm, Shoulder, and Hand (DASH) 8, full symmetric strength, no lateral condylar prominence or instability
- Right Elbow: Valgus deformity remained stable, with no functional limitations
- Cosmetic results were satisfactory to the family, and the patient returned to full sports participation.
This case illustrates several unique aspects of pediatric upper limb deformity management:
- Rarity: Windswept deformity of the elbow, irrespective of cause, has been sparingly described in literature. Most of the existing literature defines the term as an asymmetric angular deformity of the knees requiring the need for bilateral intervention [14]. Here we describe a post-traumatic windswept deformity of the elbow. The deformity developed after trauma occurring at different periods of time. The deformity also developed due to a lack of specialist orthopedic care, due to lockdowns imposed due to the COVID-19 pandemic.
- Surgical decision-making: In unilateral deformities, the contralateral limb’s carrying angle guides correction. Bilateral deformity required reliance on normative anatomical data. In a study described by Verma et al., of 140 children, the mean radiological carrying angle on the left side and right side were 9.07 ± 2.13 and 8.85 ± 2.09, respectively. The mean values of clinical carrying angle (CCA) on the left side and right side were 8.77 ± 2.03 and 8.55 ± 2.01, respectively [15]. Erdoğan and Malas measured CCA in a study of 20 dead fetuses aged between 10 and 35 weeks of gestation, without external anomalies. The mean ± standard deviation values of the carrying angle were 14.18 ± 5.52 and 8.21 ± 4.82° in males and in females, respectively [16]. Golden et al. found in a study of 300 children that the carrying angle in girls (11.5 ± 4.81) was significantly greater than in boys (9.3 ± 4.21), with a mean of 10.3±4.62 [17].
- Technique choice: A variety of corrective osteotomies have been described for cubitus varus [3,10,18,19]. Lateral closing wedge osteotomy is the most described method to correct cubitus varus, but it has its pitfalls [4]. The cosmetic result with lateral closing wedge osteotomy is frequently compromised by its propensity to result in a prominent lateral condyle when the angulation is rectified [3,11,18,19]. Following osteotomies that prevent the distal humerus translation, the injured side appears different from the unaffected side, as if the varus deformity is still present. This may happen due to the radial shift of the distal humeral fragment relative to the shaft. Wong et al. [11] reported an incidence of 64% of this complication in a series of 22 patients; Bellemore et al. [3] noted this complication in 22% of patients (6/27). However, spontaneous correction of the lateral prominence has been described because of remodeling.
Because a disfiguring deformity is the primary reason for surgery for the majority of cubitus varus patients, the corrective surgery should be straightforward, safe, and technically sound, and ought to provide almost normal cosmesis. Dome osteotomy is an alternative to the lateral closing wedge osteotomy that results in better cosmesis. The first person to describe dome osteotomy for cubitus varus correction was Tachdjian [10], who did not record any outcomes. Both Kanaujia et al. [19] and Tien et al. [9] showed good outcomes without side effects. Bellemore MC et al. [3] did not report any lateral condylar prominence in their series of 12 patients operated on with dome osteotomy. Tien et al. [9] observed a similar result in their series of 15 patients.
- Functional evaluation: Objective scores (MEPS and DASH) are essential for standardized reporting. Few studies on pediatric deformity correction include these validated scores [13]. In our case, rehabilitation commenced at 3 weeks, and follow-up over 18 months demonstrated excellent cosmesis and function (MEPS 95 and DASH score 8). No lateral condylar prominence or recurrent deformity was observed.
- Delayed presentation: This case reflects the consequences of delayed orthopedic care during the pandemic, emphasizing global health disparities [13].
Limitations
- Single case report: Findings may not be generalizable
- Selective imaging: Advanced imaging was limited. Surgical planning was based on plain radiographs
- Follow-up: Longer follow-up beyond 18 months is required
- No alternative techniques: Gradual correction with external fixation was not explored
- Ethical considerations: Surgical planning was influenced by parental preference.
Windswept deformity of the elbow is a rare post-traumatic phenomenon, and the literature is insufficient to guide management. This case demonstrates that dome osteotomy offers safe and cosmetically superior correction, with excellent functional outcomes. Normative anatomical data can guide surgical planning in bilateral deformities when contralateral reference points are unavailable.
Windswept deformity of the elbow is a rare but possible phenomenon with limited literature, making it difficult to form a definite protocol to treat it. When such a condition arises, decision-making depends on the functional limitation and cosmetic concern. Angular deformity correction can be decided using the population average in such cases.
References
- 1. Jansen NJ, Dockx RB, Witlox AM, Straetemans S, Staal HM. Windswept deformity a disease or a symptom? A systematic review on the aetiologies and hypotheses of simultaneous genu valgum and varum in children. Children (Basel) 2022;9:703. [Google Scholar] [PubMed]
- 2. Shetty GM, Mullaji A, Khalifa AA, Ray A. Windswept deformities – An indication to individualise valgus correction angle during total knee arthroplasty. J Orthop 2016;14:70-2. [Google Scholar] [PubMed]
- 3. Bellemore MC, Barrett IR, Middleton RW, Scougall JS, Whiteway DW. Supracondylar osteotomy of the humerus for correction of cubitus varus. J Bone Joint Surg Br 1984;66:566-72. [Google Scholar] [PubMed]
- 4. Griffin PP. Supracondylar fractures of the humerus. Treatment and complications. Pediatr Clin North Am 1975;22:477-86. [Google Scholar] [PubMed]
- 5. Miyamura S, Oka K, Abe S, Shigi A, Tanaka H, Sugamoto K, et al. Altered bone density and stress distribution patterns in long-standing cubitus varus deformity and their effect during early osteoarthritis of the elbow. Osteoarthritis Cartilage 2018;26:72-83. [Google Scholar] [PubMed]
- 6. Döhler JR. Suprakondyläre korrekturosteotomie beim post-traumatischen cubitus varus 3 fälle bei 2 Patienten. Unfallchirurg 2002;105:397-400. [Google Scholar] [PubMed]
- 7. Gorelick L, Robinson D, Loberant N, Rozano-Gorelick A, Yassin M, Garti A, et al. Assessment of the normal and pathological alignment of the elbow in children using the trochleocapitellar index. BMC Musculoskelet Disord 2014;15:60. [Google Scholar] [PubMed]
- 8. Joseph B. Deformities and limitation of movement of the elbow. In: Paediatric Orthopaedic Diagnosis. New Delhi: Springer India; 2015. p. 269-78. Available from: https://link.springer.com/10.1007/978-81-322-2392-4_27 [Last accessed on 2023 May 30]. [Google Scholar] [PubMed] [CrossRef]
- 9. Tien YC, Chih HW, Lin GT, Lin SY. Dome corrective osteotomy for cubitus varus deformity. Clin Orthop Relat Res 2000;380:158-66. [Google Scholar] [PubMed]
- 10. Tachdjian MR. Osteotomy of distal humerus for correction of cubitus varus. In: Smith AB, editor. Pediatric Orthopedics. Philadelphia, PA: WB Saunders; 1972. p. 1588-91. [Google Scholar] [PubMed]
- 11. Wong HK, Lee EH, Balasubramaniam P. The lateral condylar prominence. A complication of supracondylar osteotomy for cubitus varus. J Bone Joint Surg Br 1990;72:859-61. [Google Scholar] [PubMed]
- 12. Cho CH, Song KS, Min BW, Bae KC, Lee KJ. Long-term results of remodeling of lateral condylar prominence after lateral closed-wedge osteotomy for cubitus varus. J Shoulder Elbow Surg 2009;18:478-83. [Google Scholar] [PubMed]
- 13. Ngo PE, Lau Huey Yih F, Sabir Husin Athar S. A rare case of bilateral cubital valgus secondary to congenital anterior radial head dislocation. Cureus 2024;16:e70855. [Google Scholar] [PubMed]
- 14. Babu S, Vaish A, Vaishya R. Windswept deformities of the knee are challenging to manage. Knee Surg Relat Res 2020;32:46. [Google Scholar] [PubMed]
- 15. Verma V, Singh A, Kushwaha NS, Sharma Y, Singh A. Correlation between morphometric measurements and carrying angle of human elbow. Cureus 2022;14:e27331. [Google Scholar] [PubMed]
- 16. Erdoğan K, Malas MA. The investigation of the carrying angle of the elbow in fetal period. Surg Radiol Anat 2020;42:911-8. [Google Scholar] [PubMed]
- 17. Golden DW, Jhee JT, Gilpin SP, Sawyer JR. Elbow range of motion and clinical carrying angle in a healthy pediatric population. J Pediatr Orthop B 2007;16:144-9. [Google Scholar] [PubMed]
- 18. Matsushita T, Nagano A. Arc osteotomy of the humerus to correct cubitus varus. Clin Orthop Relat Res 1997;336:111-5. [Google Scholar] [PubMed]
- 19. Kanaujia RR, Ikuta Y, Muneshige H, Higaki T, Shimogaki K. Dome osteotomy for cubitus varus in children. Acta Orthop Scand 1988;59:314-8. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2025 Evaluating Outcomes of Step-Cut Osteotomy for Pediatric Cubitus Deformities
January 1, 2025 Evaluating Outcomes of Step-Cut Osteotomy for Pediatric Cubitus Deformities August 10, 2023 Persistent Ulnar Nerve Palsy with Cubitus Valgus Deformity Following a Surgically Treated Flexion-type Supracondylar Humeral Fracture – A Case Report
August 10, 2023 Persistent Ulnar Nerve Palsy with Cubitus Valgus Deformity Following a Surgically Treated Flexion-type Supracondylar Humeral Fracture – A Case Report March 10, 2023 Analysis of Gait Ability and Patient Reported Outcome Measurements after Robotic-assisted Total Knee Arthroplasty for Osteoarthritis of the Knee with Windswept Deformity
March 10, 2023 Analysis of Gait Ability and Patient Reported Outcome Measurements after Robotic-assisted Total Knee Arthroplasty for Osteoarthritis of the Knee with Windswept Deformity March 10, 2024 Bilateral Sprengel Deformities, Mirror Movements Synkinesis, and Arthrogryposis Multiplex Congenita: A Novel Combination
March 10, 2024 Bilateral Sprengel Deformities, Mirror Movements Synkinesis, and Arthrogryposis Multiplex Congenita: A Novel Combination