
Hip arthroscopy after closed reduction enables minimally invasive removal of incarcerated fragments, confirms joint stability, avoids open surgery, and preserves hip function in selected posterior hip dislocations.
Dr. Abhishek Jain, Department of Orthopaedics, Sanjay Gandhi Post Graduate Institute, Lucknow, Uttar Pradesh, India. E-mail: coslyte@gmail.com
Introduction: Posterior hip dislocations combined with acetabular posterior wall fractures are usually managed with open reduction and internal fixation. However, select cases may benefit from closed reduction followed by minimally invasive arthroscopic evaluation.
Case Report: We report a case of a 27-year-old male who sustained left side complex posterior hip dislocation with ipsilateral compound Grade 2 fracture of the shaft of the tibia with facial and chest injury following a high-speed motorcycle accident. The injury was successfully managed with closed manual reduction of the hip joint with debridement and closed reduction internal fixation of the fractured tibia with intramedullary nailing and subsequent hip arthroscopy. Arthroscopy confirmed fracture stability, revealed loose bodies, and allowed chondral assessment without the need for open reduction. At 3 months follow-up, the patient had returned to full activity with no signs of instability of the hip joint or arthritis, supporting the use of arthroscopy in select cases.
Conclusion: Hip arthroscopy following successful closed reduction is a valuable minimally invasive option in selected posterior hip dislocations, enabling removal of incarcerated fragments, confirmation of stability, reduced surgical morbidity, and favorable functional outcomes.
Keywords: Posterior hip dislocation, acetabular fracture, posterior wall, hip arthroscopy, manual reduction, minimally invasive orthopedics.
Hip dislocations constitute medical emergencies that may present at a hospital and necessitate immediate intervention. Prompt reduction is essential to preserve femoral head vascularity and prevent complications, such as avascular necrosis and joint arthritis. Post-traumatic arthritis following complex posterior hip dislocation is 88%, and simple hip dislocation is 24% [1]. Closed reduction of a hip dislocation can be effectively accomplished using standard reduction techniques, which generally yield a high success rate. However, complications may occur when an associated acetabular fracture is present. During the closed reduction process, there is a risk that the fracture fragment may become incarcerated, leading to a non-concentric reduction. It has been reported that despite the early reduction in <3 h, medium-tolong-term results after simple dislocations show satisfactory results in only one-half of the patients [2]. We present a case involving a posterior hip dislocation accompanied by an associated posterior wall fracture. Initially managed through closed reduction, it was observed that a small bone fragment became entrapped within the joint. To address this complication, we employed minimally invasive hip arthroscopy to successfully remove the fragment, resulting in a favourable functional outcome. The literature on the application of hip arthroscopy in acute trauma settings is notably limited. To the best of our knowledge, this represents the first reported case from India where hip arthroscopy was employed to extract an entrapped bony fragment following a post-reduction hip dislocation.
A 27-year-old male patient reported to the emergency department following a road traffic accident (motorcycle–motorcycle collision) with complaints of facial injury (laceration over scalp and ear), chest injury, pain and swelling over the left hip, and pain, swelling, and wound over the left leg (Fig. 1a).
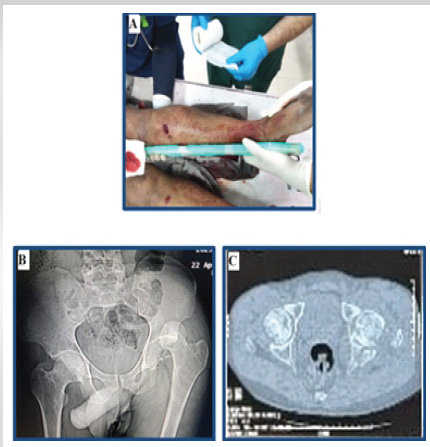
Figure 1: Compound fracture of the tibia with posterior dislocation of the hip in a polytrauma case (a). Posterior dislocation of the left hip with comminuted fracture of the posterior wall of the acetabulum (b). Computed tomography scan showing incarcerated posterior wall fragment in the left hip joint (c).
The patient had a deformity over the left hip and left leg and was unable to walk. On, clinical examination we found that he had flexion – adduction – internal rotation of the left hip. His leg showed external rotation and abduction. There was tenderness and abnormal mobility in the left leg. In addition, there was tenderness at the left hip, and the femoral head was palpable in the gluteal region. The range of movements at the hip was grossly restricted and painful. There was no distal neurovascular deficit noted. After providing advanced trauma life support to the casualty, the patient was sent for radiography. X-rays of the pelvis with both hips and the left leg were taken. From the radiograph, we confirmed that there is a posterior dislocation of the left hip with a posterior wall fracture of the acetabulum (Fig. 1b) and a segmental fracture of the shaft of the left tibia. The patient was then taken to emergency OT and subjected to manual closed reduction of the left hip under sedation. As there was a fracture in the shaft of the tibia, the force was not transmitted to the hip joint, so we gave splintage to the leg, and the hip was reduced using the Allis maneuver. Post–reduction CT scan of the pelvis confirmed concentric reduction with femoral head congruency, minimally displaced posterior wall fragment, and intra-articular bony fragments (Fig. 1c). Since the patient had chest and facial trauma, after pre-anesthetic clearance, the patient was posted on day 2 for fracture fixation of the tibia and hip arthroscopy in the same setting. Under spinal anesthesia in the supine position, closed reduction and internal fixation of the fractured shaft of the left tibia was done using an interlocking intramedullary nail, and then the patient was put on a traction table, and left hip arthroscopy was done. Irrigation, debridement, and dynamic assessment of joint stability were performed. Hip arthroscopy revealed intra-articular loose bodies (small posterior wall fragments), which were removed, minimal chondral injury on the femoral head with intact labrum, and a stable posterior wall fracture (Fig. 2). Due to the stability of the acetabular fracture and to minimize soft-tissue injuries to the capsule and the hip, internal fixation of the fracture was not done. The patient was given below-knee skin traction to prevent abnormal hip movements.
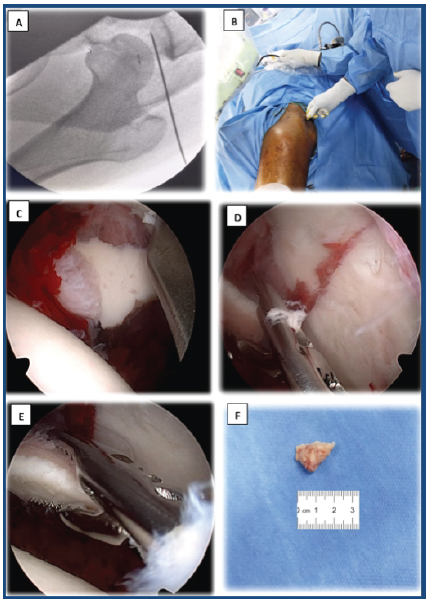
Figure 2: Arthroscopic-assisted removal of an incarcerated fragment from the hip joint. Identification of joint space under fluoroscopy for proper portal positioning (a and b). Assessment of joint congruency and removal of the incarcerated fragment (c, d, e). Extracted bone fragment (f).
Post-surgery, X–rays and CT scans were done, which showed concentric, congruent and reduced hip without any incarcerated fracture fragment in the left hip joint with stable and minimally displaced fracture of the posterior wall of the acetabulum (Fig. 3). At 6 weeks, radiographs showed a stable and congruous left hip with a uniting fracture posterior wall of the acetabulum (Fig. 4). Early range of motion exercises initiated by the 2nd week, progression to partial and full weight-bearing based on pain and imaging. At 8 weeks, the patient has good functional and radiological outcomes (Fig. 5).
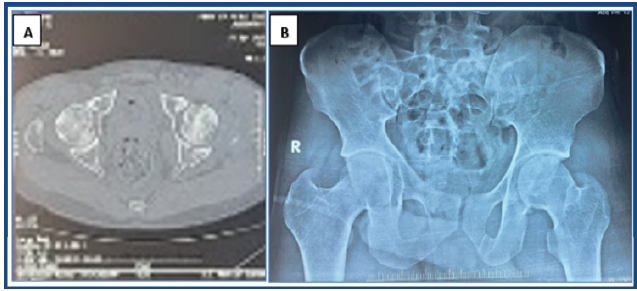
Figure 3: Post-operative computed tomography scan (a) and X-rays (b) showing a congruous left hip joint.
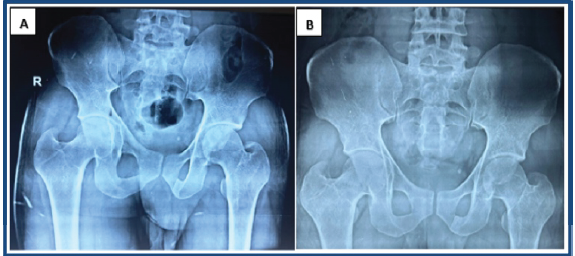
Figure 4: Follow-up X-ray after 4 weeks (a) and after 8 weeks (b) showing congruous left hip joint and uniting fracture of the posterior wall of the acetabulum.
Figure 5: Functional status of the patient at 2 months post-arthroscopy. Standing (a). Sitting (b).
Distraction of the hip for inspection of the joint with successful removal of intra-articular loose bodies after closed reduction of a hip dislocation was reported in two patients in 1994 by Keene and Villar [3]. Byrd described 30 successful hip arthroscopy cases in 1996, of which three were performed for post-traumatic loose fragments in young athletic males [4]. This was followed by several studies where hip arthroscopy was used to treat intra-articular damage associated with hip trauma in cases without complex injuries [5,6,7]. One successful case of arthroscopically assisted percutaneous fixation of a fracture of the weight-bearing region of the acetabulum was reported by Yamamoto et al. [8] in 2003. Yang et al. subsequently reported on two cases of anterior column acetabular fractures that were treated with arthroscopically assisted indirect reduction and percutaneous fixation. This case highlights a successful minimally invasive approach for a traditionally surgical condition. According to conventional medical practice, the patient would have necessitated a safe surgical dislocation or a posterior approach to the hip joint, involving capsulotomy, distraction, and fragment removal. These procedures inherently carry an increased risk of avascular necrosis and heterotopic ossification. In addition, they pose the potential for further damage to the surrounding area and elevate the likelihood of intraoperative and post-operative complications. Careful selection of patients based on displacement, stability, and congruency post-reduction can allow for less invasive options. The reported benefits of this technique included fracture and cartilage debridement, decreased fluoroscopy use required to ensure no joint penetration of acetabular column screws, and to directly assess joint congruity after reduction [9]. Arthroscopically diagnosed loose bodies were reported in 92% of 39 dislocated hips, including seven of nine patients in whom the reduction was concentric and loose bodies were not identified on CT [10], and another reported that eight of 11 cases had loose bodies that had not been diagnosed on pre-operative imaging [8]. Owens and Busconi [11] also described a consecutive cohort of patients undergoing hip arthroscopy for loose bodies after dislocations and fracture dislocations that did not require an open procedure, and a successful outcome was reported in all patients. In our case, the patient presented with multiple injuries, necessitating that any significant surgical intervention be optimized over several days or conducted under high risk. For a non-concentric reduction, early intervention was imperative to mitigate the risk of hip arthritis and avascular necrosis. Hip arthroscopy effectively addressed both concerns; it allowed for a procedure with minimal surgical duration and employed a minimally invasive technique. This approach facilitated the removal of the bone fragment and achieved concentric reduction of the joint.
Hip arthroscopy provides valuable intra-articular assessment, enabling confident conservative management. The early intervention minimized soft tissue trauma and preserved hip function in this case.
In selected posterior hip dislocations with stable posterior wall fractures, hip arthroscopy after closed reduction allows safe removal of incarcerated fragments, accurate intra-articular assessment, and avoids morbid open surgery while preserving hip function.
References
- 1. Padhyay SS, Moulton A. The long-term results of traumatic posterior dislocation of the hip. J Bone Joint Surg Br 1981;63: 548–51. [Google Scholar] [PubMed]
- 2. Dreinhöfer KE, Schwarzkopf SR, Haas NP, et al. Isolated traumatic dislocation of the hip: Long-term results in 50 patients. J Bone Joint Surg Br 1994;76: 6–12. [Google Scholar] [PubMed]
- 3. Keene GS, Villar RN. Arthroscopic loose body retrieval following traumatic hip dislocation. Injury 1994;25: 507–10 [Google Scholar] [PubMed]
- 4. Byrd JW. Hip arthroscopy for posttraumatic loose fragments in the young active adult: three case reports. Clin J Sport Med 1996;6: 129-33; discussion 133–4 [Google Scholar] [PubMed]
- 5. Khanna V, Harris A, Farrokhyar F. Hip arthroscopy: prevalence of intra-articular pathologic findings after traumatic injury of the hip. Arthroscopy 2014;30: 299–304. [Google Scholar] [PubMed]
- 6. Ilizaliturri VM, Jr, Gonzalez-Gutierrez B, Gonzalez-Ugalde H. Hip arthroscopy after traumatic hip dislocation. Am J Sports Med 2011;39(Suppl): 50S–7S. [Google Scholar] [PubMed]
- 7. Philippon MJ, Kuppersmith DA, Wolff AB. Arthroscopic findings following traumatic hip dislocation in 14 professional athletes. Arthroscopy 2009;25: 169–74. [Google Scholar] [PubMed]
- 8. Yamamoto Y, Ide T, Ono T. Usefulness of arthroscopic surgery in hip trauma cases. Arthroscopy 2003;19: 269–73. [Google Scholar] [PubMed]
- 9. Yang JH, Chouhan DK, Oh KJ. Percutaneous screw fixation of acetabular fractures: applicability of hip arthroscopy. Arthroscopy 2010;26: 1556–61. [Google Scholar] [PubMed]
- 10. Mullis BH, Dahners LE. Hip arthroscopy to remove loose bodies after traumatic dislocation. J Orthop Trauma 2006;20: 22–6. [Google Scholar] [PubMed]
- 11. Owens BD, Busconi BD. Arthroscopy for hip dislocation and fracture-dislocation. Am J Orthop 2006;35: 584–7. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 September 1, 2025 Total Hip Arthroplasty with Cage Application for Complex Posterior Hip Dislocation and Acetabular Fracture in a Patient with Prior Patellectomy: A Case Report
September 1, 2025 Total Hip Arthroplasty with Cage Application for Complex Posterior Hip Dislocation and Acetabular Fracture in a Patient with Prior Patellectomy: A Case Report December 1, 2025 The use of an Antiprotrusio Cage in Acetabular Reconstruction for Periprosthetic Transverse Fracture through a Direct Anterior Approach: A Case Report
December 1, 2025 The use of an Antiprotrusio Cage in Acetabular Reconstruction for Periprosthetic Transverse Fracture through a Direct Anterior Approach: A Case Report December 1, 2025 Total Hip Arthroplasty for Neglected Hip Dislocation – Surgical Technique and Results
December 1, 2025 Total Hip Arthroplasty for Neglected Hip Dislocation – Surgical Technique and Results December 1, 2025 Total Hip Replacement after Acetabular Fracture Fixation: Surgical Challenges, Techniques, and Outcomes
December 1, 2025 Total Hip Replacement after Acetabular Fracture Fixation: Surgical Challenges, Techniques, and Outcomes