
Unclassified sciatic nerve variants may be encountered during acetabular surgery, and awareness of such atypical anatomy is essential to prevent iatrogenic nerve injury.
Dr. Abhimaan Reddy Bheemreddyvalla, Department Of Orthopedics, Vinayaka Missions Kirupananda Variyar Medical College and Hospital, Salem, Tamil Nadu, India. E-mail: bheemreddyabhimaan@gmail.com
Introduction: Anatomical variations of the sciatic nerve are of significant clinical importance due to their implications in hip surgery, regional anesthesia, and the evaluation of sciatic neuropathies. The most widely accepted description of sciatic nerve-piriformis muscle relationships is the Beaton and Anson classification, which encompasses six recognized patterns. However, rare anatomical variants exist that do not conform to this classification and may predispose patients to nerve injury or diagnostic challenges.
Case Report: We report a rare, unclassified anatomical variation of the sciatic nerve encountered intraoperatively during open reduction and internal fixation of a posterior wall acetabular fracture in a 32-year-old male following a road traffic accident. The sciatic nerve was observed to divide into its tibial and common peroneal components below the piriformis muscle; a pattern not described in existing classification systems.
Conclusion: Awareness of such atypical anatomy is essential for orthopedic surgeons to prevent iatrogenic nerve injury and highlights the need for further anatomical and radiological studies to expand current classification systems.
Keywords: Sciatic nerve variation, piriformis muscle, Beaton and Anson classification, acetabular fracture, posterior wall acetabulum, sciatic nerve anatomy, Kocher-Langenbeck approach.
The sciatic nerve is the chief nerve of the posterior compartment of the thigh and is the largest branch of the sacral plexus, as well as the thickest nerve in the human body. It arises from the ventral rami of spinal nerves L4, L5, S1, S2, and S3 and is composed of two distinct components enclosed within a common sheath: The tibial and the common peroneal (fibular) components [1,2]. The tibial component is derived from the ventral divisions of the ventral rami of L4 to S3, while the common peroneal component originates from the dorsal divisions of the ventral rami of L4 to S2. The sciatic nerve leaves the pelvis through the greater sciatic notch, usually passing below the piriformis muscle, and descends in the gluteal region over the obturator internus, gemelli, and quadratus femoris muscles, coursing between the ischial tuberosity and the greater trochanter of the femur [3,4]. It then enters the posterior compartment of the thigh, where it runs downward deep to the hamstring muscles, and on reaching the superior border of the popliteal fossa, it typically divides into the tibial and common fibular (peroneal) nerves. Beaton and Anson classified six anatomical variations of the sciatic nerve based division of the nerve distal and proximal to the piriformis muscle [5]. In this case report, we intend to discuss about the rare anatomical sciatic nerve variation not classified under Beaton and Anson in a case of posterior wall of acetabular fracture.
A 32-year-old gentleman was brought to the emergency department with an alleged history of a road traffic accident and sustained a closed injury to the pelvis. On initial assessment, the patient was conscious, oriented, and hemodynamically stable, with normal vital parameters. A detailed primary and secondary survey revealed no evidence of head injury, spinal injury, or blunt trauma to the chest or abdomen. Neurological examination was normal, with no motor or sensory deficits in any of the limbs. On local examination of the pelvis and hip region, the patient complained of severe pain in the hip and groin area and was unable to bear weight on the affected limb. The limb was held in a guarded position, and any attempt at active or passive movement of the hip elicited significant pain. There was marked tenderness on palpation over the acetabular and pelvic region, with a painful and restricted range of motion, particularly during hip flexion, abduction, and rotational movements. No obvious shortening or gross deformity of the limb was noted, and there were no open wounds, abrasions, or external signs of injury over the pelvis or hip. Distal neurovascular examination of the affected limb was normal, with intact distal pulses and preserved motor and sensory functions, including no features suggestive of sciatic nerve involvement. These clinical findings were suggestive of an acetabular fracture in the setting of high-energy pelvic trauma.
Investigations
The 3-dimensional reconstructed computed tomography scans of the pelvis with both hip joints demonstrate a fracture involving the acetabulum, with disruption of the acetabular rim and articular surface on the affected side. There is a visible irregularity and discontinuity of the pelvic ring at the acetabular region, with extension of the fracture line into the surrounding pelvic bone. The femoral head appears seated within the acetabulum without gross dislocation, although subtle incongruity of the hip joint surface is noted, suggesting intra-articular involvement. The sacrum, sacroiliac joints, and contralateral hemipelvis appear intact, with no obvious widening or diastasis (Fig. 1 and 2).
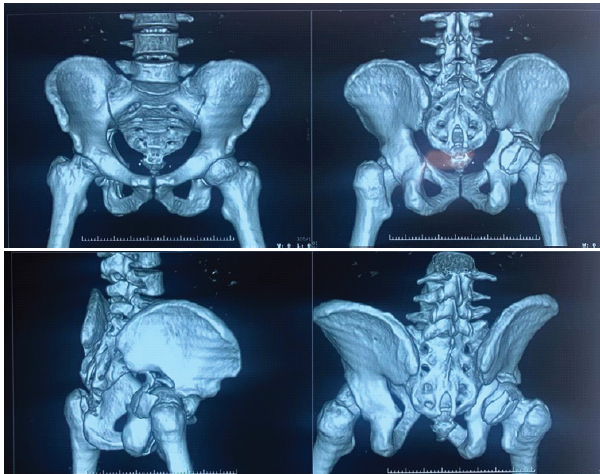
Figure 1& 2: 3-dimensional reconstructed computed tomography scans of the pelvis with both hip joints.
Management
Under spinal anesthesia patient underwent open reduction and internal fixation of the acetabulum through the posterior Kocher-Langenbeck approach on deep dissection, we encountered a rare anatomical variation, the sciatic nerve dividing into common peroneal and tibial nerve below the piriformis (Figs. 3 and 4).
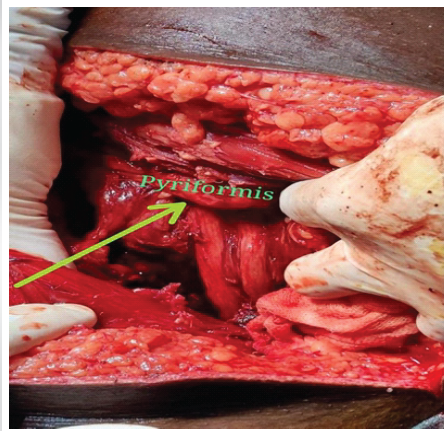
Figure 3: Intra-operatively, on deep dissection we encountered rare anatomical variation, sciatic nerve dividing into common peroneal and tibial nerve below the piriformis
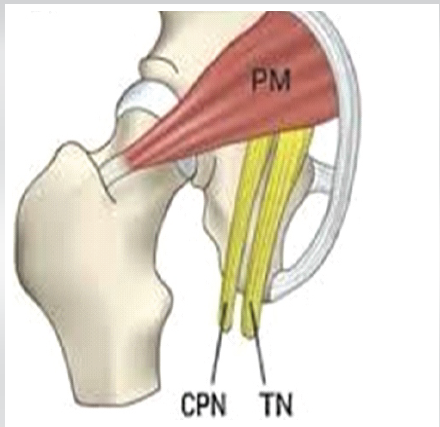
Figure 4: Pictorial depiction of sciatic nerve dividing into common peroneal and tibial nerve below the piriformis.
After noticing the sciatic nerve variation intraoperatively, with adequate pre-caution to prevent from the traction neuropraxia and nerve damage, internal fixation with plate osteosynthesis of the acetabular fracture was done.
Outcome and follow-up
During the hospital stay, he remained hemodynamically stable with no neurological deterioration. Pain was adequately controlled, and there were no immediate post-operative or in-hospital complications. Gradual mobilization was initiated as per protocol, with protected or non-weight-bearing advised on the affected limb. On follow-up visits, the patient showed progressive improvement in pain and hip range of motion. Long-term neurological and functional outcomes were normal. Radiological evaluation demonstrated satisfactory fracture alignment and healing. At the latest follow-up, the patient was ambulatory with support, had no neurovascular deficits, and reported improvement in functional outcomes, with no evidence of complications, such as infection, implant failure, or post-traumatic arthritis (Fig. 5).
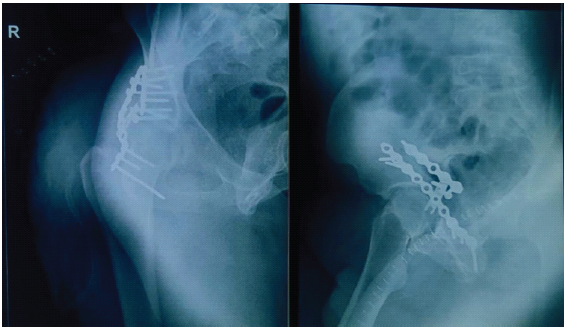
Figure 5: Post-operative X-rays.
Beaton and Anson proposed a classical classification describing the anatomical relationship between the sciatic nerve and the piriformis muscle, which remains the most widely accepted system to date (Beaton and Anson, 1937). Multiple cadaveric studies across different populations have consistently demonstrated that Type A, in which an undivided sciatic nerve passes below an undivided piriformis muscle, represents the normal anatomical configuration and is the most prevalent pattern, reported in approximately 85–92% of cases [3,4,5]. The remaining variants – Types B–F – are relatively uncommon and together account for a small proportion of cases, with reported incidences varying between 1% and 13% depending on ethnicity and sample size [6,7,8]. Cadaveric studies from India, Africa, Nepal, and Europe have reaffirmed the predominance of Type A anatomy, while documenting occasional occurrences of Types B, C, and D, and extremely rare presentations of Types E and F [4,5,6,7]. Several authors have also reported atypical findings, such as trifurcation of the sciatic nerve, reunion of divided components in the thigh, and anomalous muscular branches, which do not strictly conform to the original Beaton and Anson classification, thereby highlighting inherent limitations of the system [8,9]. Our finding is not reported by the existing cadaveric dissection or anatomical study literature, which could have strengthened our anatomical description. This potential intraoperative observation bias is due to the underreporting of subtle variants by the surgeons. The Beaton and Anson classification may evolve with future anatomical and radiological evidence. In the present case report, the observed sciatic nerve variation does not correspond to any of the six types described by Beaton and Anson, emphasizing the existence of rare and unclassified anatomical patterns. Such variants are infrequently documented in the literature and may be overlooked during routine dissection or imaging studies. Although modern radiological modalities, including magnetic resonance imaging (MRI) and magnetic resonance neurography, have improved visualization of sciatic nerve anatomy and its relationship with the piriformis muscle, most imaging-based studies primarily describe variants that fit within the established classification, with limited reporting of completely unclassified patterns [5,8 ]. We acknowledge that no comparative cohort with standard sciatic anatomy was evaluated, and therefore, relative risk assessment is not possible. Our findings are specific to the Kocher-Langenbeck posterior approach and may not extrapolate to other surgical approaches. We acknowledge that this is a single-case report, which inherently limits generalizability. However, these anatomical variations are of considerable importance, as they may predispose individuals to non-discogenic sciatica, particularly piriformis syndrome, which accounts for approximately 6–8% of sciatica cases [6,8,10]. Furthermore, anatomical variation was not identified on routine pre-operative imaging and magnetic resonance neurography or dedicated sciatic nerve MRI was not performed, and that such imaging could have potentially characterized the variation pre-operatively. Unrecognized or unclassified sciatic nerve variants may contribute to persistent or unexplained sciatic pain, failed sciatic nerve blocks, or iatrogenic nerve injury during hip, pelvic, or gluteal surgeries. The post-operative nerve conduction studies or electromyography were not performed as there were no clinical deficits. Therefore, this case underscores the need for further detailed cadaveric studies and advanced radiological investigations in patients with both discogenic and non-discogenic sciatica. Accumulation of such data may facilitate refinement or expansion of existing classification systems, leading to improved anatomical understanding, more accurate diagnosis, and safer surgical and anesthetic interventions.
This case report highlights a rare and unclassified anatomical variation of the sciatic nerve encountered during surgical management of a posterior wall acetabular fracture. Although the Beaton and Anson classification accounts for the majority of known sciatic nerve-piriformis relationships, uncommon variants may exist outside this framework and pose potential risks during surgical and anesthetic procedures. Recognition of such anomalies is crucial to avoid iatrogenic nerve injury and unexplained post-operative neuropathies. This report emphasizes the need for increased awareness among clinicians and supports the necessity for further cadaveric and radiological studies to refine and expand existing classifications, thereby improving diagnostic accuracy and surgical safety.
Orthopedic surgeons should anticipate rare sciatic nerve configurations during posterior hip approaches, employ meticulous dissection and nerve protection, and consider advanced imaging or anatomical variation when unexplained neuropathy or technical difficulty is encountered.
References
- 1. Standring S, editor. Gray’s Anatomy: The Anatomical Basis of Clinical Practice. 42nd ed. London: Elsevier; 2021. p. 1302-6. [Google Scholar] [PubMed]
- 2. Moore KL, Dalley AF, Agur AM. Clinically Oriented Anatomy. 9th ed. Philadelphia, PA: Wolters Kluwer; 2023. p. 610-4. [Google Scholar] [PubMed]
- 3. Beaton LE, Anson BJ. The relation of the sciatic nerve and its subdivisions to the piriformis muscle. Anat Rec 1937;70:1-5. [Google Scholar] [PubMed]
- 4. Adibatti M, Sangeetha V. Study on variant anatomy of sciatic nerve. J Clin Diagn Res 2014;8:AC07-9. [Google Scholar] [PubMed]
- 5. Poutoglidou F, Piagkou M, Totlis T, Tzika M, Natsis K. Sciatic nerve variants and the piriformis muscle: A systematic review and meta-analysis. Cureus 2020;12:e11531. [Google Scholar] [PubMed]
- 6. Atoni AD, Oyinbo CA, Francis DA, Tabowei UL. Anatomic variation of the sciatic nerve: A study on the prevalence, and bifurcation loci in relation to the piriformis and popliteal fossa. Acta Med Acad 2022;51:52-8. [Google Scholar] [PubMed]
- 7. Jha AK, Baral P. Composite anatomical variations between the sciatic nerve and the piriformis muscle: A Nepalese cadaveric study. Case Rep Neurol Med 2020;2020:7165818. [Google Scholar] [PubMed]
- 8. Bharadwaj UU, Varenika V, Carson W, Villanueva-Meyer J, Ammanuel S, Bucknor M, et al. Variant sciatic nerve anatomy in relation to the piriformis muscle on magnetic resonance neurography: A potential etiology for extraspinal sciatica. Tomography 2023;9:475-84. [Google Scholar] [PubMed]
- 9. Misra BD. The relations of the sciatic nerve to the piriformis muscle in Indian cadavers. J Anat Soc India 1954;3:5-12. [Google Scholar] [PubMed]
- 10. Fassler PR, Swiontkowski MF, Kilroy AW, Routt MLC. Injury of the sciatic nerve associated with acetabular fracture. J Bone Joint Surg Am. 1993;75(8):1157-1166. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Navigation-Assisted Percutaneous Fixation of an Anterior Column and Posterior Hemitransverse Fracture in an Elderly Patient: A Case Report
March 1, 2026 Navigation-Assisted Percutaneous Fixation of an Anterior Column and Posterior Hemitransverse Fracture in an Elderly Patient: A Case Report February 1, 2026 Arthroscopic-Assisted Removal of Incarcerated Fragment following Manual Reduction of Posterior Hip Dislocation in Acute Polytrauma Patient: A Case Report
February 1, 2026 Arthroscopic-Assisted Removal of Incarcerated Fragment following Manual Reduction of Posterior Hip Dislocation in Acute Polytrauma Patient: A Case Report December 1, 2025 The use of an Antiprotrusio Cage in Acetabular Reconstruction for Periprosthetic Transverse Fracture through a Direct Anterior Approach: A Case Report
December 1, 2025 The use of an Antiprotrusio Cage in Acetabular Reconstruction for Periprosthetic Transverse Fracture through a Direct Anterior Approach: A Case Report December 1, 2025 Total Hip Arthroplasty for Neglected Hip Dislocation – Surgical Technique and Results
December 1, 2025 Total Hip Arthroplasty for Neglected Hip Dislocation – Surgical Technique and Results