
Docking at the caudal transverse process during full-endoscopic discectomy for far lateral disc herniation provides a simple, safe, and reproducible approach with minimal tissue dissection and reduced nerve manipulation.
Dr. K Nanjunda, Center for Endoscopic Spine Surgery, Sushruta Hospital for Orthopedics and Traumatology, Miraj, Maharashtra, India. E-mail: nanjundadragon@gmail.com
Introduction: The use of least invasive full-endoscopic spine systems has decreased the amount of tissue dissection, blood loss, and duration of post-operative recovery after intervention for far-lateral disc herniations (FLDH).
Case Report: In this technique, docking over the caudal transverse process is described as an efficient alternative approach with a decreased need for manipulation of the exiting nerve root. All cases diagnosed with FLDH in the outpatient department who opted for surgical intervention after a failed non-invasive trial were included. A review of the literature on FLDH regarding the key anatomy used during a far-lateral approach was also performed.
Conclusion: The subjects showed significant improvement at 6-week and 12-week post-operative visits, and at 6-month follow-up had near-complete relief of symptoms, including resolution of lower limb numbness. Prior techniques for full-endoscopic discectomy for FLDH report docking on the facet joint, pars interarticularis, and the cranial transverse process. This technical note details that docking at the caudal transverse process improves upon these established techniques and provides a more straightforward and safer alternative.
Keywords: Full-endoscopic spine surgery, far lateral disc herniation, transverse process, minimally invasive spine surgery, endoscopic discectomy.
The use of full-endoscopic spine systems has significantly decreased the amount of tissue dissection, blood loss, and duration of post-operative recovery for far-lateral disc herniation (FLDH). There are various techniques for docking, including those on the facet joint, pars interarticularis, and the cranial transverse process. The challenges of the least invasive surgery for FLDH lie in the limited bony landmarks compared to soft-tissue elements, which result in variation regarding where to dock. The anatomy is also less familiar than midline posterior approaches, potentially creating spatial confusion. Furthermore, the dorsal root ganglion (DRG) of the exiting nerve root is more susceptible to thermal and mechanical injury, requiring less manipulation than what is used during standard discectomy. In this note, the precise technique for docking on the caudal transverse process is described as an easier approach with decreased need for manipulation of the exiting nerve root [1,2,3,4,5,6,7].
Technical description
Patient selection and evaluation
All patients underwent routine clinical evaluation, including dynamic radiographic views of the spine and magnetic resonance imaging (MRI), which confirmed the diagnosis of FLDH. Each patient was initially given a conservative trial for 2–3 weeks, including non-steroidal anti-inflammatory drugs (NSAIDs) and physiotherapy.
Surgical setup
Surgical intervention was advised only when conservative management failed to alleviate symptoms. The proposed docking technique utilized a full-endoscopic approach for FLDH, performed more efficiently by docking at the transverse process at the caudal level. This technique represents a modification of a previously described approach by the senior author, in which docking was performed at the cranial level and then angled caudally. Docking at the caudal transverse process allows for easier identification of key anatomical landmarks, a logical progression toward the disc space, and minimal manipulation of the sensitive exiting nerve root and DRG. All surgeries were performed at the Center for Endoscopic Spine Surgery, Sushruta Hospital for Orthopedics and Traumatology, Miraj, Maharashtra, by the senior author (Dr. Girish P. Datar).
Patient positioning and marking
Following induction with general anesthesia, the patient was turned to the prone position over bolsters. Fluoroscopy was positioned laterally, and the lumbar spine was prepared and draped in the usual sterile fashion. Using lateral fluoroscopy, the appropriate incision site to approach the right level was identified and marked at the tip of the caudal transverse process.
Docking and instrument placement
After local anesthetic infiltration and incision, the first dilator was placed through the incision and advanced to the desired level. The position was confirmed fluoroscopically. Care was taken not to apply excessive downward pressure to avoid fracture of the transverse process, and the tip of the dilator was rested at the junction of the transverse process and facet joint (similar to the technique used for inserting a percutaneous pedicle screw). The position and level were again confirmed with fluoroscopy. The working sleeve was inserted over the dilator, followed by the introduction of the endoscope. Soft-tissue clearance was performed using plasma or radiofrequency.
Foraminotomy and disc removal
The cranial tip of the transverse process, the transverse process–facet junction, and the dorsal wall of the foramen were identified. A joker or angled curette was used to develop a plane between the soft tissue and the dorsal wall of the foramen. The intertransverse ligament attached to the cranial part of the caudal transverse process was separated. A Kerrison punch was then used for foraminotomy at the dorsal wall; the cranial margin of the caudal transverse process was trimmed, the intertransverse ligament removed, and the foraminal ligaments released. The transverse process–to–transverse process corridor was exposed and dissected. The exiting nerve root was identified and gently retracted toward the cranial transverse process to visualize the herniated disc, which was confirmed fluoroscopically. Annulotomy was performed, and disc fragments were removed using rongeurs.
Confirmation of decompression
The foraminal, extraforaminal, and epidural spaces were inspected for residual disc fragments using blunt probes. At the end of the procedure, complete decompression of the exiting nerve root was confirmed. Below are the images from an example case performed at our setup.
Representative case
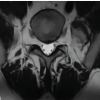
A female patient presented with complaints of left lower limb radiculopathy without any neurological deficits. MRI revealed a left FLDH at the L4–L5 level. A trial of non-invasive management, including NSAIDs and physiotherapy, failed to alleviate her symptoms, following which she was planned for surgical intervention. The patient had no significant comorbidities and was deemed fit for surgery after obtaining physician clearance. A full-endoscopic paraspinal approach was planned and performed. Pre-operative MRI and dynamic radiographs of the lumbosacral spine showed decreased disc height at L4–L5 with age-related degeneration but no evidence of instability (Fig. 1).

Figure 1: MRI LS spine with whole spine screening suggestive of L4-L5 left sided far lateral disc herniation. Dynamic Radiographs of the Lumbo-sacral spine shows decreased disc height at L4-L5 and age related degenration. No obvious instability is noted.
Intraoperative fluoroscopic imaging demonstrated the docking point at the caudal transverse process of the desired operating level, similar to that used in percutaneous pedicle screw insertion (Fig. 2).

Figure 2: C-ARM intra operative picture depicting the docking point at the Caudal Transverse process of the desired operating level.
Endoscopic visualization identified the caudal transverse process, superior articular process (facet), and the transverse process (TP)–facet junction (Fig. 3a). After debulking, the superficial and deep layers of the intertransverse ligament were visualized (Fig. 3b). Following trimming of the transverse process and removal of the inter-transverse ligament, the exiting nerve root and its accompanying vascular plexus became clearly visible (Fig. 3c).

Figure 3: (a) Intraoperative endoscopic view stills of the labeled structures. (1) Caudal transverse process. (2) Facet (S.A.P). (3) Transverse process-Facet junction. (b) Intraoperative picture after debulking showing the superficial and deep layers of the intertransverse ligament. (c) After trimming the transverse process and removing the intertransverse ligament, the exiting nerve root and its accompanying vascular plexus become clearly visible. Gentle dissection through the fibrous tissue allows cranial retraction of the root, exposing the herniated disc located within the safe triangle between the transverse process and the exiting root.
Fig. 4 shows the docking points used in full-endoscopic approach for FLDH. Gentle dissection through the fibrous tissue allowed cranial retraction of the exiting root, revealing the herniated disc located within the “safe triangle” between the transverse process and the exiting root, which was subsequently extracted under direct endoscopic vision, achieving complete decompression. (Table 1)

Figure 4: The docking points used in the full-endoscopic approach for far-lateral disc herniations.

Table 1: Docking landmarks in FLDH techniques
All patients experienced significant pain relief by 6 weeks postoperatively. Numbness resolved progressively by 12 weeks to 3 months, with most patients symptom-free at 6 months. No perioperative complications were observed.
FLDH originates within or lateral to the neural foramen, compressing the exiting nerve root. These patients are more likely to present with neurological deficits due to the constrained space. Traditionally, these herniations were managed through a midline approach and laminotomy, with resection of the pars, facetectomy, and interbody fusion. Modified far-lateral approaches were later successfully adopted to access FLDH using varied techniques. As surgical methods advanced, minimally invasive surgery (MIS) and endoscopic approaches for FLDH have been increasingly advocated. A comprehensive review of the literature on FLDH regarding the key anatomy used during a MIS far-lateral approach was also performed. Articles on PubMed were searched, and publications that contained descriptions of surgical techniques for FLDH were collected. Open midline approaches were excluded. The selected articles were categorized into mini-open Wiltse approaches and MIS tubular or endoscopic approaches. These were further subdivided based on the authors’ descriptions of their key anatomic landmarks for accessing the disc space and herniated fragment. The summary is tabulated below:
The present technique is a modification of previously used MIS tubular and endoscopic discectomy methods for FLDH. Docking at the caudal TP emphasizes minimal soft-tissue dissection and bone removal, which aligns with the natural anatomy at the caudal TP. Previous reports have described partial removal of the lateral pars; however, since the lateral pars has the greatest thickness, its removal carries a risk of iatrogenic stress fractures [8,9]. Similarly, surgeons targeting the facet joint risk poorer outcomes if more than 25–30% of the joint is removed [8,10]. Excessive removal or thermal injury to the facet capsule and synovium can lead to early-onset arthritis and act as a source of post-operative pain. Docking on the inferior TP provides readily identifiable anatomy under both fluoroscopy and direct endoscopic visualization, reducing the need for more complex and expensive intraoperative imaging [11]. Furthermore, this approach eliminates an additional step required when docking at the cranial TP, which typically necessitates subsequent caudal angulation. It also minimizes endoscope movement, allowing easier isolation of the disc space and herniated fragment. Extraforaminal or extreme lateral lesions can be effectively reached through this far-lateral approach. Decreased nerve root manipulation is achieved via the natural corridor to the disc space, following the pedicle of the caudal level. The caudal TP naturally guides the surgeon medially toward the junction with the facet. After releasing the intertransverse membrane from the caudal TP, the TP-facet junction can be used as a guide to slide cranially along the bone and pedicle. This maneuver isolates the caudal aspect of the neural foramen and provides direct access to the disc space without requiring soft-tissue stripping over the exiting nerve root. In addition, a cadaveric study demonstrated that drilling of the caudal TP – or, in the case of L5–S1 FLDH, the superior sacral ala – most effectively exposed the exiting nerve root while providing access to the disc without further bone removal [12]. In almost all cases, the extraforaminal disc fragment lies caudal to the exiting nerve root and displaces it superiorly and laterally. Thus, the caudal TP serves as the most consistent bony landmark for accessing the extraforaminal disc. Extruded disc fragments can be mobilized with blunt dissecting probes, sliding beneath the nerve and into the disc space. If necessary, the annulus may be incised to allow further disc removal. Minimal retraction of the exiting nerve root is required and can be performed in a lateral-cranial direction. This approach positions the surgeon close to the disc level, reducing the need for soft-tissue retraction. In contrast, other docking points, such as the pars or facet position, the disc to be at a greater distance, requiring more extensive maneuvering. The primary limitation of this study is the rarity of FLDH, which limits the sample size and precludes statistically significant comparisons between techniques. Recurrence of FLDH also presents an additional challenge not addressed here, and its optimal management remains controversial even in conventional revision discectomy or fusion. Nonetheless, this technique offers an easily adaptable approach. Future studies with larger prospective case series and detailed analysis of operative techniques and anatomical variations are warranted [6,7,13,14,15,16,17].
Docking at the caudal transverse process in full-endoscopic discectomy for FLDH minimizes soft-tissue dissection, nerve manipulation, and bone removal. It offers a straightforward, reproducible, and anatomically consistent approach compared to docking at the facet, pars interarticularis, or cranial TP.
The caudal transverse process serves as a dependable bony landmark for endoscopic access to FLDH, offering surgeons a simpler and safer alternative for complete decompression with minimal invasiveness.
References
- 1. Epstein NE. Foraminal and far lateral lumbar disc herniations: Surgical alternatives and outcome measures. Spinal cord 2002;40:491-500. [Google Scholar] [PubMed]
- 2. Akinduro OO, Kerezoudis P, Alvi MA, Yoon JW, Eluchie J, Murad MH, et al. Open versus minimally invasive surgery for extraforaminal lumbar disk herniation: A systematic review and meta-analysis. World Neurosurg 2017;108:924-38.e3. [Google Scholar] [PubMed]
- 3. O’Toole JE, Eichholz KM, Fessler RG. Surgical site infection rates after minimally invasive spinal surgery. J Neurosurg Spine 2009;11:471-6. [Google Scholar] [PubMed]
- 4. Lofrese G, Mongardi L, Cultrera F, Trapella G, De Bonis P. Surgical treatment of intraforaminal/extraforaminal lumbar disc herniations: Many approaches for few surgical routes. Acta Neurochir (Wien) 2017;159:1273-81. [Google Scholar] [PubMed]
- 5. Berra LV, Di Rita A, Longhitano F, Mailland E, Reganati P, Frati A, et al. Far lateral lumbar disc herniation part 1: Imaging, neurophysiology and clinical features. World J Orthop 2021;12:961-9. [Google Scholar] [PubMed]
- 6. Khan JM, McKinney D, Basques BA, Louie PK, Carroll D, Paul J, et al. Clinical presentation and outcomes of patients with a lumbar far lateral herniated nucleus pulposus as compared to those with a central or paracentral herniation. Global Spine J 2019;9:480-6. [Google Scholar] [PubMed]
- 7. Voyadzis JM, Gala VC, Sandhu FA, Fessler RG. Minimally invasive approach for far lateral disc herniations: Results from 20 patients. Minim Invasive Neurosurg 2010;53:122-6. [Google Scholar] [PubMed]
- 8. Ivanov AA, Faizan A, Ebraheim NA, Yeasting R, Goel VK. The effect of removing the lateral part of the pars interarticularis on stress distribution at the neural arch in lumbar foraminal microdecompression at L3-L4 and L4-L5: Anatomic and finite element investigations. Spine (Phila Pa 1976) 2007;32:2462-6. [Google Scholar] [PubMed]
- 9. Sari R, Elibol FK, Özlü EB, Elmacı İ, Demir T. Could isthmic approach to far lateral disc hernias cause instability? Clinical Biomech (Bristol) 2020;76:105004. [Google Scholar] [PubMed]
- 10. Bae JS, Kang KH, Park JH, Lim JH, Jang IT. Postoperative clinical outcome and risk factors for poor outcome of foraminal and extraforaminal lumbar disc herniation. J Korean Neurosurg Soc 2016;59:143-8. [Google Scholar] [PubMed]
- 11. Nicoletti GF, Umana GE, Chaurasia B, Ponzo G, Giuffrida M, Vasta G, et al. Navigation-assisted extraforaminal lumbar disc microdiscectomy: Technical note. J Craniovertebr Junction Spine 2020;11:316-20. [Google Scholar] [PubMed]
- 12. Soliman H, Fridley J, Telfeian A, Choi DB, Galgano M, Kosztowski T, et al. Minimally invasive, far lateral lumbar microdiscectomy with intraoperative computed tomography navigational assistance and electrophysiological monitoring. World Neurosurg 2019;122:e1228-39. [Google Scholar] [PubMed]
- 13. Park HW, Park KS, Park MS, Kim SM, Chung SY, Lee DS. The comparisons of surgical outcomes and clinical characteristics between the far lateral lumbar disc herniations and the paramedian lumbar disc herniations. Korean J Spine 2013;10:155-9. [Google Scholar] [PubMed]
- 14. Marquardt G, Bruder M, Theuss S, Setzer M, Seifert V. Ultra-long-term outcome of surgically treated far-lateral, extraforaminal lumbar disc herniations: A single-center series. Eur Spine J 2012;21:660-5. [Google Scholar] [PubMed]
- 15. Tessitore E, De Tribolet N. Far-lateral lumbar disc herniation: The microsurgical transmuscular approach. Neurosurgery 2004;54:939-42; discussion 942. [Google Scholar] [PubMed]
- 16. Hodges SD, Humphreys SC, Eck JC, Covington LA. The surgical treatment of far lateral L3-L4 and L4-L5 disc herniations. A modified technique and outcomes analysis of 25 patients. Spine (Phila Pa 1976) 1999;24:1243-6. [Google Scholar] [PubMed]
- 17. O’Hara LJ, Marshall RW. Far lateral lumbar disc herniation. The key to the intertransverse approach. J Bone Joint Surg Br 1997;79:943-7. [Google Scholar] [PubMed]
- 18. Hitchon PW, Awe OO, Close L, Sukkarieh HG. Minimally invasive pars approach for foraminal disc herniation. J Clin Neurosci 2015;22:1128-32. [Google Scholar] [PubMed]
- 19. Phan K, Dunn AE, Rao PJ, Mobbs RJ. Far lateral microdiscectomy: A minimally-invasive surgical technique for the treatment of far lateral lumbar disc herniation. J Spine Surg 2016;2:59-63. [Google Scholar] [PubMed]
- 20. Siu TL, Lin K. Microscopic tubular discectomy for far lateral lumbar disc herniation. J Clin Neurosci 2016;33:129-33. [Google Scholar] [PubMed]
- 21. Salame K, Lidar Z. Minimally invasive approach to far lateral lumbar disc herniation: Technique and clinical results. Acta Neurochir (Wien) 2010;152:663-8. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Surgical Experience in Symptomatic Bertolotti Syndrome: Clinical Follow-up of Three Patients Refractory to Conservative Management
January 1, 2026 Surgical Experience in Symptomatic Bertolotti Syndrome: Clinical Follow-up of Three Patients Refractory to Conservative Management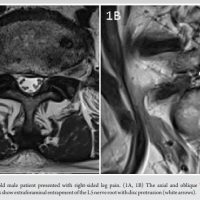 March 10, 2024 Unilateral Biportal Endoscopy for L5-S1 Extraforaminal Stenosis (Far Out Syndrome) – Technical note With Literature Review
March 10, 2024 Unilateral Biportal Endoscopy for L5-S1 Extraforaminal Stenosis (Far Out Syndrome) – Technical note With Literature Review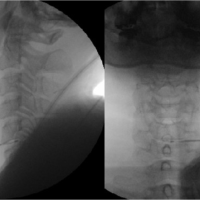 January 10, 2024 Use of Navigable Ablation Decompression Treatment (L-DISQ) for Contained Cervical Disc Herniation – Technical Note and Literature Review
January 10, 2024 Use of Navigable Ablation Decompression Treatment (L-DISQ) for Contained Cervical Disc Herniation – Technical Note and Literature Review March 1, 2025 Simultaneous Bilateral Knee Extensor Mechanism Injury in a Young Male: A Clinical Diagnosis and Literature Review
March 1, 2025 Simultaneous Bilateral Knee Extensor Mechanism Injury in a Young Male: A Clinical Diagnosis and Literature Review