
Portal-site ganglion cyst formation is a rare complication following shoulder arthroscopy and should be considered in patients presenting with delayed post-operative swelling or pain. Early recognition and surgical excision provide definitive treatment with excellent outcomes.
Dr. Behic Celik, Department of Orthopedics and Traumatology, Yeditepe University Hospital, Icerenkoy, 34752 Atasehir/Istanbul, Istanbul, Turkey. E-mail: behic13@gmail.com
Abstract
Introduction: Ganglion cyst formation following shoulder arthroscopy is an exceptionally rare complication, particularly when arising from an arthroscopy portal site. Most shoulder ganglion cysts are associated with labral pathology and are typically located in the spinoglenoid or suprascapular notch. Portal-site or periarticular cysts cause a diagnostic challenge and are seldom reported in the literature.
Case Report: We present the case of a 56-year-old female with a history of multiple prior shoulder arthroscopic procedures who developed a painful, localized swelling at the lateral arthroscopy portal site 8 weeks after surgery. Initial post-operative recovery was uneventful. Imaging studies revealed a well-defined cystic lesion without communication with the glenohumeral joint. Laboratory evaluation showed no evidence of infection. Due to persistent symptoms, surgical excision was performed. Intraoperatively, the cyst was found to originate from the periportal region without a clear intra-articular connection. Histopathological examination confirmed the diagnosis of a ganglion cyst. The patient experienced complete symptom resolution with no recurrence at 2-year follow-up.
Conclusion: This case highlights a rare post-operative complication of shoulder arthroscopy and emphasizes the importance of considering periportal ganglion cysts in patients presenting with delayed post-operative swelling or pain. Awareness of this entity allows timely diagnosis and definitive treatment with excellent clinical outcomes.
Keywords: Ganglion cyst, Shoulder arthroscopy, Portal-site complication, Periarticular cyst
Shoulder arthroscopy is one of the most frequently performed orthopedic procedures worldwide, favored for its minimally invasive nature and low complication rates [1]. While overall complication rates are reported to be between 1.0% and 7.9%, these typically include stiffness, infection, or neurological injuries. The development of atypical soft-tissue masses, such as synovial or ganglion cysts in the post-operative period, is considered exceedingly rare [2,3]. Ganglion cysts are benign, fluid-filled lesions that most commonly arise near joints or tendon sheaths and are thought to result from degenerative changes in connective tissue rather than true synovial proliferation [4]. Although frequently encountered in the wrist and hand, intramuscular or periarticular ganglion cysts are rare and represent an unusual diagnostic entity [4]. While ganglion cysts are commonly associated with labral tears in the spinoglenoid or suprascapular notches due to a “one-way valve” mechanism, their emergence at portal sites or within unexpected intramuscular locations following surgery presents a diagnostic challenge [5,6]. In the shoulder region, ganglion cysts are most commonly associated with labral pathology and are typically located in the spinoglenoid or suprascapular notch, where they may cause compression of the suprascapular nerve [7]. Literature suggests that such cysts may arise from leakage of intra-articular fluid through capsular defects or surgical tracts created during arthroscopy [2,6]. This case report presents a rare instance of a periportal ganglion cyst following shoulder arthroscopy, describing its clinical presentation, imaging characteristics, and management.
A 56-year-old female presented with right shoulder pain and restricted range of motion. Her medical history was notable for multiple prior right shoulder arthroscopic procedures. She had previously undergone arthroscopy in March 2010 for a superior labrum anterior to posterior (SLAP) lesion and subacromial impingement, in November 2010 for a rotator cuff tear with recurrent SLAP pathology, and in January 2016 for labral degeneration and impingement. The index arthroscopic procedure was performed in November 2023 due to chondral damage, a rotator cuff tear, and recurrent subacromial impingement. Procedures, including debridement, repair, and acromioplasty, were performed accordingly. The arthroscopy was carried out using three standard portals: Anterior, lateral, and posterior. Post-operative wound healing was uneventful, and early rehabilitation progressed rapidly. At 6 weeks postoperatively, clinical findings were satisfactory, and the patient was asymptomatic. However, 8 weeks after surgery, she was re-presented with pain during shoulder movement and localized swelling in the operated shoulder region. Physical examination revealed a palpable swelling at the lateral arthroscopy portal site without erythema, warmth, or signs of infection. Laboratory evaluation showed normal leukocyte count and C-reactive protein levels. Ultrasonography demonstrated a well-defined fluid-filled cystic lesion without internal vascularization. Magnetic resonance imaging confirmed a cystic mass without communication with the glenohumeral joint (Fig. 1).
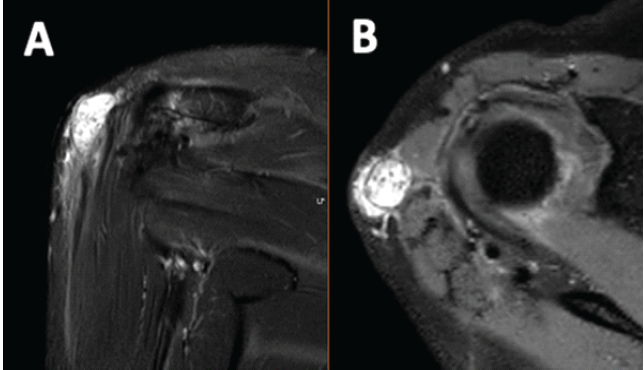
Figure 1: Pre-operative T2-weighted magnetic resonance imaging of the right shoulder demonstrates a well-defined cystic lesion at the lateral arthroscopy portal site. (a) Coronal view showing a hyperintense periarticular cystic mass adjacent to the deltoid muscle. (b) Axial view confirming the cystic nature of the lesion without evidence of communication with the glenohumeral joint.
Given persistent symptoms, surgical excision was performed through a 3-cm longitudinal incision centered over the lateral portal site (Fig. 2). Intraoperatively, a cystic lesion with a deep stalk was identified; however, no clear connection to the joint space or surrounding structures was observed. After excision, the deltoid fascia was closed with absorbable sutures, and the wound was closed in layers.
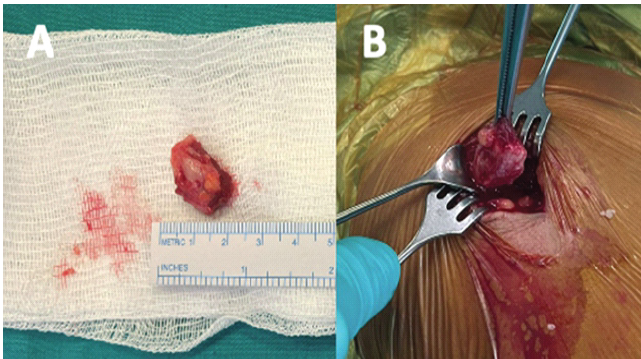
Figure 2: Intraoperative findings and excised specimen of the periportal ganglion cyst. (a) Gross appearance of the excised cystic lesion following complete removal, measured using a sterile ruler. (b) Intraoperative photograph demonstrating the cyst emerging through the lateral arthroscopy portal during surgical excision.
Cyst fluid, cyst wall tissue, and intra-articular tissue samples were obtained for microbiological and histopathological examination. No microbial growth was detected. Histological analysis confirmed the diagnosis of a periarticular ganglion cyst (Fig. 3). At final follow-up, the patient remained asymptomatic with no evidence of recurrence.
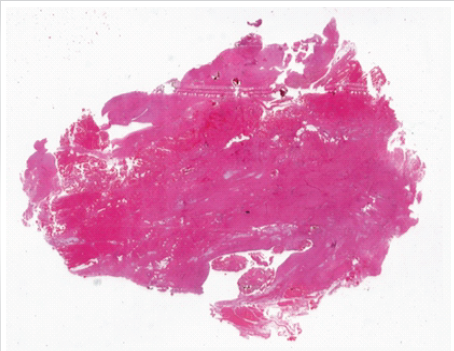
Figure 3: Histopathological examination of the excised cyst wall demonstrates dense fibrous connective tissue without synovial lining, consistent with the diagnosis of a ganglion cyst (hematoxylin and eosin stain, low magnification).
Although shoulder arthroscopy is considered a safe procedure, rare post-operative complications involving atypical soft-tissue lesions have been described and should be recognized to ensure timely diagnosis and management [8]. The most commonly reported post-operative complications include stiffness, persistent pain, infection, and neurovascular injury. Ganglion or synovial cyst formation following shoulder arthroscopy is considered extremely rare, particularly when arising from a portal site or in an atypical periarticular location. Ganglion cysts around the shoulder are most frequently observed in the spinoglenoid or suprascapular notch and may result in compression of the suprascapular nerve with associated weakness or infraspinatus atrophy [2,3]. Less commonly, ganglion cysts have been described at the long head of the biceps tendon, within the bicipital groove, or within rotator cuff musculature [1]. Tan et al. reported that intramuscular synovial cysts are rare entities, often associated with full- or partial-thickness rotator cuff tears, and may require open excision for definitive management [5]. Imaging plays a crucial role in the evaluation of post-operative soft-tissue masses around the shoulder, particularly in differentiating benign cystic lesions from solid or infectious processes. Magnetic resonance imaging is the modality of choice for evaluating ganglion cysts, which typically appear as well-defined, homogeneous, T2-hyperintense lesions, allowing differentiation from solid soft-tissue masses [9,10]. Portal-site synovial cyst formation after shoulder arthroscopy has been reported only once previously. Steiner et al. described a synovial cyst arising from the lateral portal 8 weeks postoperatively, proposed to result from localized fascial weakness and synovial fluid extrusion through a micro-defect [6]. Similar to our case, the patient initially demonstrated satisfactory early post-operative recovery before developing delayed localized swelling requiring surgical excision. Ganglion cysts arising in atypical or post-operative locations may lack a clear communication with the joint space, supporting alternative mechanisms such as localized fascial weakness or fluid extravasation along surgical tracts [10]. Several factors may have contributed to cyst formation in our patient. Repeated arthroscopic procedures may have resulted in cumulative capsular and fascial weakening, predisposing the patient to post-operative synovial fluid leakage. Notably, magnetic resonance imaging showed no communication between the cyst and the joint space, suggesting a periarticular origin rather than extension from an intra-articular structure. To our knowledge, this represents only the second reported case of a portal-site ganglion cyst following shoulder arthroscopy and the first in a patient with multiple prior arthroscopic interventions. This case highlights that periportal ganglion cysts should be considered in patients presenting with unexpected post-operative swelling or pain. Timely surgical excision provides definitive treatment with excellent clinical outcomes.
Ganglion cyst formation at an arthroscopy portal site is an exceptionally rare complication of shoulder arthroscopy. In patients presenting with delayed post-operative swelling or pain near a portal site, a periportal ganglion cyst should be considered in the differential diagnosis. Surgical excision is effective and results in favorable clinical outcomes.
Delayed-onset localized swelling or pain after shoulder arthroscopy should raise suspicion for rare complications such as periportal ganglion cyst formation. Awareness of this entity allows prompt diagnosis and definitive surgical management with excellent outcomes
References
- 1. Shin JJ, Popchak AJ, Musahl V, Irrgang JJ, Lin A. Complications after arthroscopic shoulder surgery: A review of the American board of orthopaedic surgery database. JAAOS Glob Res Rev 2018;2:e093. [Google Scholar] [PubMed]
- 2. Schroder CP, Skare Ø, Stiris M, Gjengedal E, Uppheim G, Brox JI. Treatment of labral tears with associated spinoglenoid cysts without cyst decompression. J Bone Joint Surg Am 2008;90:523-30. [Google Scholar] [PubMed]
- 3. Khubaib MU, Monaco R. Unique location and origin of a ganglion cyst. Cureus 2021;13:e16453. [Google Scholar] [PubMed]
- 4. Gude W, Morelli V. Ganglion cysts of the wrist: Pathophysiology, clinical picture, and management. Am Fam Physician 2008;78:725-32. [Google Scholar] [PubMed]
- 5. Tan EW, Dharamsi FM, McCarthy EF, Fayad LM, McFarland EG. Intramuscular synovial cyst of the shoulder: A case report. J Shoulder Elbow Surg 2010;19:e20-4. [Google Scholar] [PubMed]
- 6. Steiner CL, Schreiber VM, Braun S, Imhoff AB. Synovial cyst in the portal site: A rare complication after shoulder arthroscopy. Arthroskopie 2011;24:216-9. [Google Scholar] [PubMed]
- 7. Piatt BE, Hawkins RJ, Fritz RC, Ho CP, Wolf E, Schickendantz M. Clinical evaluation and treatment of spinoglenoid notch ganglion cysts. J Shoulder Elbow Surg 2002;11:600-4. [Google Scholar] [PubMed]
- 8. Moen TC, Rudolph GH, Caswell K, Espinoza C, Burkhead WZ Jr., Krishnan SG. Complications of shoulder arthroscopy. J Am Acad Orthop Surg 2014;22:410-9. [Google Scholar] [PubMed]
- 9. Beaman FD, Peterson JJ. MR imaging of cysts, ganglia, and bursae about the knee. Radiol Clin North Am 2007;45:969-82. [Google Scholar] [PubMed]
- 10. McCarthy CL, McNally EG. The MRI appearance of cystic lesions around the joints. Skeletal Radiol 2004;33:187-209. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Angiofibroma of Knee Masquerading as Ganglion Cyst – A Rare Case Report
July 1, 2026 Angiofibroma of Knee Masquerading as Ganglion Cyst – A Rare Case Report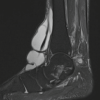 May 1, 2026 Giant Ganglion Cyst of the Tibialis Anterior Tendon Presenting with Adult-Acquired Flatfoot Deformity: A Case Report
May 1, 2026 Giant Ganglion Cyst of the Tibialis Anterior Tendon Presenting with Adult-Acquired Flatfoot Deformity: A Case Report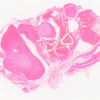 April 1, 2026 Cavernous Hemangioma Masquerading as a Ganglion Cyst of the Flexors of the Index Finger: A Case Report
April 1, 2026 Cavernous Hemangioma Masquerading as a Ganglion Cyst of the Flexors of the Index Finger: A Case Report February 1, 2026 Minimally Invasive Double Loop Suture Technique for Recurrent Acromioclavicular Joint Ganglion Cyst in an Elderly Female: A Case Report
February 1, 2026 Minimally Invasive Double Loop Suture Technique for Recurrent Acromioclavicular Joint Ganglion Cyst in an Elderly Female: A Case Report