
Column specific fixation of complex distal radius fractures can be achieved using standard implants, without reliance on costly low profile systems.
Dr. Kumar Rahul, Department of Joint Replacement and Orthopaedics, Tata Main Hospital, C-Road West, Northern Town, Bistupur - 831001, Jamshedpur, Jharkhand, India. E-mail: drkrahul90@gmail.com
Introduction: Distal forearm fractures, particularly AO type 23B and 23C, pose challenges in achieving anatomical alignment and functional recovery. Fragment-specific fixation has emerged as a promising approach, especially for complex fracture patterns.
Objectives: The objective of the study was to evaluate the radiological and functional outcomes of column-specific fixation in distal forearm fractures using cost-effective implants
Materials and Methods: This retrospective observational study was conducted over 2 years at a tertiary care center in Eastern India. Distal forearm fractures operated using low-cost, standard orthopedic implants were studied.
Results: Functional outcomes were good to excellent in 70.1% of patients. No cases of tendon attrition or hardware prominence were observed.
Conclusion: Fragment-specific fixation can be safely performed without high-end implants and with minimal complications, supporting its use as a cost-effective and anatomically sound technique.
Keywords: Fragment-specific, column-specific, distal radius fracture, distal forearm fractures.
Intra‑articular distal radius fractures (DRFs) are complex injuries [1]. They commonly include multiple articular fragments along with areas of metaphyseal impaction. These fractures account for about 17% of all fractures and nearly 75% of forearm fractures, making them a significant clinical problem [2,3]. Rikli and Regazzoni [4] used computed tomography (CT) studies to propose the three‑column concept of the distal forearm. In this model, the intermediate column, formed by the lunate fossa and sigmoid notch, bears most of the axial load. The radial column also contributes substantially. Medoff and Kopylov [5] later described the key ligament attachments of the intermediate column. Their work strengthened the rationale for fragment‑specific fixation, which focuses on stabilizing each fracture fragment separately. Volar locking plates remain widely used for DRFs. However, they often fail to provide adequate support to dorsal articular fragments. These dorsal fragments are better stabilized using fragment‑specific implants. High‑end, low‑profile, and anatomical implants are effective but expensive. Their limited availability, especially in many Indian hospitals, adds further challenges to routine care. This study evaluates the outcomes of complex intra‑articular DRFs treated with fragment‑specific fixation using standard, readily available orthopedic implants. The aim is to demonstrate that reliable results can be achieved without the need for costly, specialized implant systems.
This study was approved by the Ethics Committee of Tata Main Hospital and Manipal Tata Medical College, Jamshedpur, adhering to the ethical standards.
Study design and setting
A retrospective observational study was conducted at our institution over a 2-year period, from May 2022 to May 2024. All eligible cases were identified through electronic medical records and radiologic databases, in accordance with STROBE recommendations for transparent reporting of study design and data sources.
Participants
Patients diagnosed with DRFs based on standard anteroposterior and lateral radiographs, supplemented with CT when needed for articular detail, were screened for eligibility. Individuals who underwent operative management for AO/OTA type 23B1 to 23C3 fractures during the study period were included in the study.
Eligibility criteria
Inclusion criteria
- Age 20–60 years
- Radiologically confirmed DRF classified as AO type 23B1 to 23C3
- Patients treated operatively within 2 weeks of injury
- Availability of complete clinical and radiographic records.
Exclusion criteria
Patients were excluded if they met any of the following:
- Presence of associated ipsilateral upper‑limb injuries
- Fractures older than 2 weeks at the time of presentation
- Pathological fractures
- Age <20 years or >60 years
- Open fractures or fractures complicated by neurovascular compromise
- Pre‑existing deformities or prior surgical interventions in the ipsilateral limb
- Inability or unwillingness to provide informed consent for the use of clinical data.
Sample size and pre-operative assessment
The sample size was calculated based on the reported incidence of intra‑articular distal radius fractures in prior literature and the expected variability in post-operative radiological parameters and Modified Mayo Wrist scores. Allowing for an anticipated 5% attrition rate, a minimum of 86 patients was determined to be necessary to ensure adequate statistical power for the primary outcome measures. The retrospective process of patient identification and selection is summarized in Table 1.
As part of routine pre-operative evaluation, all patients underwent standard radiographic assessment supplemented by CT to delineate articular involvement. The injured column(s) were identified systematically, and any fragment requiring fixation or buttressing was characterized to guide surgical planning. Surgical planning was individualized to utilize one‑, two‑, or three‑column fixation depending on the fracture morphology.
Surgical technique
A modified Henry approach was employed for volar exposure and placement of implants. When required, a dorsal approach was utilized to address fractures involving the dorsal intermediate column or the radial column. Following definitive fixation, the extensor retinaculum was split. It was interposed between the implant and the extensor tendons (Fig. 1 and 2).
Fractures at the base of the ulnar styloid indicate possible radioulnar ligament instability. Ethibond sutures were passed around the ulnar styloid. These were tied through a trans‑osseous tunnel (made in distal third ulna) in a figure‑of‑eight pattern.
Implant
Anatomically contoured locking plates are available for column-specific fixation. These implants require two key features: A low-profile design and a locking construct to prevent screw heads from impinging on the extensor tendons. However, cost and limited availability restrict their use in developing countries. Complex fracture patterns often require multiple plates, increasing expense. To overcome this, standard trauma implants were used following column-specific principles. One-third tubular plates and non-locking distal radius plates, low-profile dental plates were selected for their low profile and easy contouring to the dorsal and radial surfaces. One-third tubular plates were selected for fixation because of their malleability and low-profile design. These properties allow easy contouring and help minimize soft-tissue irritation. These plates can be cut through the edges to be placed on the radial styloid. Sections of the plate were cut through the pre-existing screw holes, to create a hook configuration. This modification enabled the plate to capture and secure small articular fragments effectively. The modified plates were then applied to maintain fragment stability and preserve joint congruity throughout the healing process. Occasionally, 2.7 mm locking screws or 3 mm Herbert screws were inserted distally through the cut holes of the modified plate (Fig. 3 and 4). This technique mimicked a headless locking construct, providing additional stability and minimizing hardware prominence in periarticular region.
Fracture patterns were evaluated preoperatively. Displaced or angulated fragments indicative of column instability were stabilized using tubular buttress plates. Minimally displaced fragments were managed with dental plates.
Clinical assessment
Early mobilization was encouraged. Wrist range‑of‑motion exercises and six‑pack hand exercises were initiated as early as post-operative day 1, depending on patient pain tolerance. Sutures were removed at 2 weeks. Follow-up evaluations were conducted at 4, 8, 12, 16, and 20 weeks, and subsequently at 6 months and 1 year.
At each visit, radiographs were obtained, and functional outcomes were assessed using the Modified Mayo Wrist score. This scoring system evaluates pain, patient satisfaction, range of motion, and grip strength, assigning 25 points to each domain for a total score of 100. The final score at 12 months was recorded and categorized as detailed in Table 2-4.
Radiological assessment
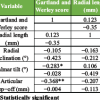
During follow-up the radiographs were assessed for the radial height, radial inclination and volar tilt. This was done on the MedDream picture archiving and communication system platform, which provided exact measurement details.
Statistical analysis
Sample size was calculated on power analysis and sample size version 15.0, and the statistical analysis of P-value was done on the Statistical Package for the Social Sciences version 22.0. A P < 0.05 was considered statistically significant.
Demographics
Of the 100 patients enrolled, 3 were lost to follow-up, leaving 97 for analysis. There were 47 males and 50 females, with a mean age of 49.7 years (range 20–60 years). Road traffic accidents were the predominant cause of injury, followed by domestic falls.
Fracture pattern
Fracture distribution included 46 AO type 23B1–B3 and 51 AO type 23C1-C3 distal radius fractures.
Fixation type
31 out of 97 patients were treated with triple column plating. 54 patients needed double column fixation, whereas 12 patients with single column plating.
Radiographic findings
At 12 months, all patients maintained radial height within normal limits (13.6 ± 2.1 mm). Radial inclination (26.8 ± 3.6°) was preserved in 94 patients (96.9%), and volar tilt (15.4 ± 4.3°) in 93 patients (95.9%).
Functional scores
Modified Mayo wrist score showed good to excellent results in 68 patients (70.1%).
Complications
Those with dorsal and radial styloid plates exhibited terminal restriction of palmar flexion, whereas volar incision cases showed terminal restriction of dorsiflexion. Post-operative complications were minimal, including two cases of transient blistering and one superficial radial nerve injury, all resolving without sequelae. No tendon attrition or hardware prominence was observed.
Representative case
A 45-year-old male sustained an AO type 23-B3 distal radius fracture following a road traffic accident. CT imaging with 3D reconstruction confirmed the fracture configuration. The fracture was approached dorsally and stabilized using dorsal and radial column plates, with additional K-wire support for the dorsal column. At 12-month follow-up, radiographs demonstrated maintained alignment, and functional assessment revealed satisfactory recovery (Fig. 5 and 6).
Distal radius fractures are common in clinical practice. X-rays often misjudge the injury. Pruitt et al. [6] stressed the role of CT scans in accurate fracture assessment. CT imaging reveals overlapping fragments and guides management. It can shift treatment from conservative to operative in many cases [7]. Anatomical reduction is essential to prevent post-traumatic arthritis. Even a minor articular step-off can lead to arthritis in up to 91% of cases [8]. Rikli and Regazzoni’s three-column theory highlights wrist biomechanics. The radial column stabilizes the wrist and articulates with the carpus [9,10]. The intermediate column maintains carpal alignment [11]. The ulnar column, including the ulnar head and triangular fibrocartilage complex, supports stability and rotation. Ulnar styloid base fractures often indicate distal radioulnar joint ligament disruption, requiring fixation. The fragment-specific approach tailors treatment to fracture characteristics. It avoids a one-size-fits-all strategy and provides more consistent results. Volar locking plates have been the preferred option for intra-articular distal radius fractures for many years. However, growing understanding of fracture columns and fragment-specific fixation challenges this approach. A single volar plate may not provide adequate support in complex patterns. Studies have found dorsal plating to be superior for comminuted lunate fossa fractures, preventing dorsal collapse [12,13,14]. This shift represents a paradigm that requires both unlearning and relearning the established concepts. Dorsal fixation of distal radius fractures has long been approached cautiously due to the proximity of extensor tendons. Advanced implants address this by providing distal locking constructs. Simic et al. [15] reported only 2% tendon irritation with dorsal low-profile plates. Hozack et al. [16] emphasized fixing the radial styloid, volar rim, dorsal wall, and dorsal-ulnar corner for joint congruity, which is difficult with just a volar locking plate construct. In our study, we achieved similar stability using commonly available orthopedic and dental implants configured as a headless construct. The 2.7 mm locking screw or the 3 mm Herbert screw in the distal hole minimizes the chances of tendon attrition over the screw head. Smaller intra-articular fragments were buttressed using the low-profile dental plates or with one-third plates modified into hook plates. The retinaculum repair was also planned in such a way that it reduced friction of the implant over the tendons. This approach was cost-effective and technically feasible. Importantly, no cases of tendon irritation or injury were observed in this study. Our findings indicate that safe and effective dorsal fixation does not require high-end implants. This reinforces that adherence to fundamental tenets of fracture management remains paramount for achieving optimal outcomes. The average implant cost for the 97 patients in our cohort was approximately ₹5,600. This expenditure is substantially lower than that associated with modern high‑end, low‑profile, anatomical, column‑specific plating systems, which often cost several times more. The markedly reduced cost of the implants used in our study underscores an important economic advantage, particularly in resource‑constrained settings. Initial cases required longer operative time and resulted in greater blood loss. However, the learning curve was steep, and subsequent surgeries were completed more efficiently with reduced operative time and blood loss. The increased operative time was, however, compensated by the early rehabilitation of the patient [17]. Early rehabilitation was started, often as early as post-operative day 2 or day 3. By the end of 6 weeks, most patients recovered joint mobility compared to ligamentotaxis or other traditional fixation, which would start joint mobility at around 4–6 weeks. However, this construct demonstrated limited effectiveness in osteoporotic complex fractures. Although adequate column buttressing could be achieved, the fixation often lacked sufficient structural support. As a result, the risk of secondary collapse remained high. Reduced bone quality likely contributed to the inability of the construct to maintain fracture alignment over time. Fractures involving the ulnar head represented another limitation of this technique. Stable fixation in this region could not be consistently achieved. Consequently, clinical and radiological outcomes in ulnar head fractures were frequently suboptimal. This study was retrospective in nature and lacked a comparative control group, which represents a significant limitation. The absence of randomization and control may introduce selection bias and restrict the generalizability of the findings. In addition, the analysis was based on 97 patients, which, although informative, may not provide sufficient statistical power to detect subtle differences or rare complications. Future research should include prospective case-control or randomized trials with larger cohorts to validate the application of column theory using modified plates.
Fragment-specific fixation is a reliable technique for restoring anatomical congruity and biomechanical stability. This study emphasizes on following the principles to restoring joint congruity rather than relying on fancy implants to replicate outcomes.
Complex intra-articular distal radius fractures can be effectively managed using fragment-specific, column-based fixation principles without dependence on expensive implant systems. Standard, readily available implants, when applied thoughtfully can achieve stable fixation, good functional outcomes, and minimal complications. This approach offers a cost-effective, reproducible solution, particularly valuable in resource-constrained settings, while maintaining sound biomechanical principles.
References
- 1. Zhou L, Gao Y, Wang D, Zhao Y, Lu T, Wang H, et al. The comparison of clinical outcomes between volar locking plate fixation and dual-plate fixation in high-energy distal radius fractures. Front Surg 2025;12:1552764. [Google Scholar] [PubMed]
- 2. Singer BR, McLauchlan GJ, Robinson CM, Christie J. Epidemiology of fractures in 15,000 adults: The influence of age and gender. J Bone Joint Surg Br 1998;80:243-8. [Google Scholar] [PubMed]
- 3. Kopylov P, Johnell O, Redlund-Johnell L, Bengner U. Fractures of the distal end of the radius in young adults: A 30-year follow-up. J Hand Surg Br 1993;18:45-9. [Google Scholar] [PubMed]
- 4. Rikli DA, Regazzoni P. Fractures of the distal end of the radius treated by internal fixation and early function. A preliminary report of 20 cases. J Bone Joint Surg Br 1996;78:588-92. [Google Scholar] [PubMed]
- 5. Medoff RJ, Kopylov P. Immediate internal fixation and motion of comminuted distal radius fractures using a new fragment specific fixation system. Orthop Trans 1998;22:165. [Google Scholar] [PubMed]
- 6. Pruitt DL, Gilula LA, Manske PR, Vannier MW. Computed tomography scanning with image reconstruction in evaluation of distal radius fractures. J Hand Surg Am 1994;19:720-7. [Google Scholar] [PubMed]
- 7. Katz MA, Beredjiklian PK, Bozentka DJ, Steinberg DR. Computed tomography scanning of intra-articular distal radius fractures: Does it influence treatment? J Hand Surg Am 2001;26:415-21. [Google Scholar] [PubMed]
- 8. Knirk JL, Jupiter JB. Intra-articular fractures of the distal end of the radius in young adults. J Bone Joint Surg Am 1986;68:647-59. [Google Scholar] [PubMed]
- 9. Anderson DD, Deshpande BR, Daniel TE, Baratz ME. A three-dimensional finite element model of the radiocarpal joint: Distal radius fracture step-off and stress transfer. Iowa Orthop J 2005;25:108-17. [Google Scholar] [PubMed]
- 10. Dwyer CL, Crosby NE, Cooney T, Seeds W, Lubahn JD. Treating unstable distal radius fractures with a nonspanning external fixation device: Comparison with volar locking plates in historical control group. Am J Orthop (Belle Mead NJ) 2017;46:E344-52. [Google Scholar] [PubMed]
- 11. Hoekzema NA, Brambila M. Column-specific distal radius fracture fixation. J Orthop Trauma 2021;35 Suppl 3:s17-20. [Google Scholar] [PubMed]
- 12. Miyashima Y, Kaneshiro Y, Yano K, Teraura H, Sakanaka H, Uemura T. Size and stabilization of the dorsoulnar fragment in AO C3-type distal radius fractures. Injury 2019;50:2004-8. [Google Scholar] [PubMed]
- 13. Ikeda K, Osamura N, Tada K. Fixation of an ulnodorsal fragment when treating an intra-articular fracture in the distal radius. Hand Surg 2014;19:139-44. [Google Scholar] [PubMed]
- 14. Chou YC, Chen AC, Chen CY, Hsu YH, Wu CC. Dorsal and volar 2.4-mm titanium locking plate fixation for AO type C3 dorsally comminuted distal radius fractures. J Hand Surg Am 2011;36:974-81. [Google Scholar] [PubMed]
- 15. Simic PM, Robison J, Gardner MJ, Gelberman RH, Weiland AJ, Boyer MI. Treatment of distal radius fractures with a low-profile dorsal plating system: An outcomes assessment. J Hand Surg Am 2006;31:382-6. [Google Scholar] [PubMed]
- 16. Hozack BA, Tosti RJ. Fragment-specific fixation in distal radius fractures. Curr Rev Musculoskelet Med 2019;12:190-7. [Google Scholar] [PubMed]
- 17. Brink PR, Rikli DA. Four-corner concept: CT-based assessment of fracture patterns in distal radius. J Wrist Surg 2016;5:147-51. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2025 Functional and Radiological Outcomes Following Volar Locking Plate Fixation for Distal Radius Fractures: A Prospective Analytical Study
December 1, 2025 Functional and Radiological Outcomes Following Volar Locking Plate Fixation for Distal Radius Fractures: A Prospective Analytical Study November 1, 2025 The Use of a Tendon Protector Sheath for Prevention of First Extensor Compartment Tendon Adhesions after Radial Column Plating for Distal Radius Fracture: A Case Report
November 1, 2025 The Use of a Tendon Protector Sheath for Prevention of First Extensor Compartment Tendon Adhesions after Radial Column Plating for Distal Radius Fracture: A Case Report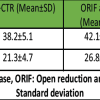 October 1, 2025 Beneath the Surface: Prophylactic Carpal Tunnel Release Cuts Carpal Tunnel Syndrome Risk Post Volar Plating
October 1, 2025 Beneath the Surface: Prophylactic Carpal Tunnel Release Cuts Carpal Tunnel Syndrome Risk Post Volar Plating October 1, 2025 Femoral Stem Subsidence Rate with Cementless Stems in Patients with Sub-capital Femoral Neck Fractures: Relationship to Proximal Femoral Geometry
October 1, 2025 Femoral Stem Subsidence Rate with Cementless Stems in Patients with Sub-capital Femoral Neck Fractures: Relationship to Proximal Femoral Geometry