
Pediatric clavicle fracture non-union is an uncommon complication of age-centric treatment protocol requiring surgical management.
Dr. Ankit Tripathi, Department of Orthopaedics, Baba Raghav Das Medical College, Gorakhpur - 273013, Uttar Pradesh, India. E-mail: ankit.aki02@gmail.com
Introduction: Clavicle fractures are common in children, representing 7–15% of pediatric fractures, typically healing with conservative management. Non-union is exceedingly rare, especially in children under 3 years of age.
Case Report: We report a case of a 3-year-old male with traumatic midshaft clavicle fracture non-union, presenting 2 years post-injury with persistent pain, swelling, deformity, and restricted shoulder function. Radiographs revealed a hypertrophic non-union with significant displacement and 2 cm shortening. The patient was managed surgically with open reduction, internal fixation using a mini-fragment plate and screws, and autogenous bone grafting. Outcome: Progressive callus formation and complete osseous union were confirmed radiologically by 12 weeks. At final follow-up, the child had a full, pain-free range of motion and no residual deformity, returning to normal activities.
Conclusion: This case highlights that clavicle non-union, although rare, can occur even in toddlers. Surgical management with plate fixation and bone grafting can yield excellent outcomes. Vigilant follow-up of displaced pediatric clavicle fractures is essential to detect and manage this uncommon complication.
Keywords: Pediatric clavicle fracture, non-union, internal fixation, bone grafting, case report
Clavicle fractures are one of the most common bony injuries in the pediatric age group. The incidence ranges from 7% to 15% of all pediatric fractures, and the middle third shaft is the most common location to get fractured [1]. The clavicle fractures in pediatric age groups are commonly treated non-operatively with slings or braces. However, surgical interventions are needed for open or impending open fractures, polytraumatized patients, floating shoulder injuries, and displaced fractures in adolescent age groups [2]. The rate of non-union of clavicle fractures is 6–12% in the adult population, and its incidence is rare in the pediatric population [3]. We report one such rare case of a 3-year-old child with a non-union fracture of the clavicle. Given the scarcity of reported cases of clavicle non-union in children under 3 years old, this report contributes significantly to the orthopedic literature [4].
A 3-year-old male child presented to the orthopedic clinic with a chief complaint of persistent pain and swelling in the right clavicular region for 2 years following a playground injury. The patient had sustained right-side clavicle fracture, which was managed with sling immobilization for 6 weeks. After 6 weeks, the patient was allowed to resume all the activities; however, he continued to experience persistent pain in the overhead abduction of the right shoulder and deformity at the fracture site. On physical examination, there was fullness over the mid-clavicle region on the right side. The overlying skin was normal with no local rise of temperature or tenderness. There was crepitus over the midshaft of the right clavicle, along with observable shortening of the clavicle. The abduction and forward flexion of the right shoulder were restricted and associated with discomfort at the fracture site as compared to the contralateral side. There were no sensory or motor deficits in the upper extremity. The plain X-ray of the right clavicle done in anteroposterior and 45° cephalic tilt showed hypertrophic non-union. The fracture margins were sclerotic without any bridging callus and displacement with approximately 2 cm of shortening (Fig. 1a and b).

Figure 1: (a and b) Plain radiograph depicting hypertrophic non-union of the right clavicle at presentation. (c-e) Intra-operative image depicting planned skin incision (c), Hypertrophic margins of the clavicle fracture (d), and 6-hole 2.7 mm locking compression plate (e). (f) Immediate post-operative radiographs depicting fracture reduction and fixation, along with bone graft.
Based on a comprehensive clinical and radiological evaluation, a definitive diagnosis of hypertrophic non-union of the right clavicle was established, and planned for surgical intervention was made.
Under general anesthesia, the patient was prepared in the supine position with the hand freely draped in the surgical field. Around 7–8 cm of transversely placed skin incision was given over the right clavicle cantered over the non-union site. The subcutaneous tissue and platysma were incised along the line of incision. The deltoid was dissected subperiosteally to expose the fracture site. The fracture ends were freshened, and the hypertrophic ends were nibbled to accommodate the plate. The fibrous tissue intervening at the fracture site and bony margins was sent for histopathological examination, which later came out to be composed of normal tissues, ruling out congenital pseudoarthrosis. A 6-hole 2.7 mm locking compression plate (LCP) was contoured and used for fracture fixation. The locally harvested Autologous bone graft was used to bridge the defect and stimulate osteogenesis at the non-union site. The wound was thoroughly irrigated and closed in layers (Fig. 1c, d, e, f). Postoperatively, the patient’s arm was immobilized in an arm sling for a period of 6 weeks. Range of motion and overhead abduction were allowed after 6 weeks. The patient was followed clinic-radiologically at regular intervals to monitor fracture union and to assess for any potential complications. Serial X-ray images done at 6 weeks, 12 weeks, and 6 months in the post-operative period confirmed progressive callus formation and eventual complete osseous union at 6 months. At the final follow-up at 9 months, the patient demonstrated a full, pain-free range of motion of the right shoulder, with no residual deformity or functional limitations, indicating a successful return to pre-injury activity levels (Fig. 2a, b, c, d, e).
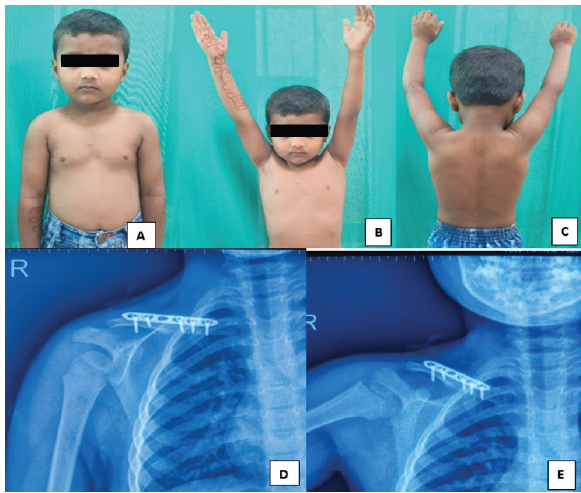
Figure 2: (a-c) 6-month post-operative image showing healed scar with full abduction and function. (d and e) Plain radiograph at 6-month post-operative depicting fracture union with no deformity and plate in situ.
Clavicle fractures are common injuries in both adults and the pediatric age group. With rich blood supply and high remodeling capacity, the pediatric clavicle fracture is preferably managed non-operatively, and the surgical intervention is reserved for older adolescents or highly displaced fractures. Most of the paediatric clavicle fractures show a similar outcome when treated non-operatively or operatively, with a rarely reported incidence of non-union [5,6,7]. Literature suggests older age as the most common cause of clavicle fracture non-union. The study by Hughes et al. [3] for the pediatric age group has suggested the mean age for clavicle non-union to be 11.4 years, with incidences ranging from 4 to 17 years. The initial fracture displacement was found to be the critical contributory factor, with completely displaced fractures having increased odds of complication by a factor of 3.2 [8]. Similar to our case, Smith and Williams have noted that in the majority of non-union cases, the right-sided clavicle was involved with suspicion of subclinical congenital pseudoarthrosis [9]. Surgical intervention for non-union involves open reduction, freshening of margins, internal fixation, and bone grafting to provide mechanical stability and enhance biological healing, which is essential for overcoming persistent non-union, particularly in cases with significant displacement. The LCP and intramedullary nails have comparable long term outcome for displaced mid-shaft clavicular fractures for fresh fractures; however, LCPs are commonly used for treating clavicle fracture non-union along with bone grafting [3,10]. We have used contoured 2.7 mm LCP commonly used mini-fragment plates for stable internal fixation while accommodating smaller bone dimensions and minimizing potential growth plate disturbance with locally harvested bone. Despite the rare occurrence of clavicle fracture non-union in children, it must be taken into consideration while managing this common injury. The clear guidelines for radiological follow-up in children with clavicle fractures are not available in the literature [3,11,12,13]. However, the treating doctors should be aware of this uncommon complication and must remain vigilant in follow-up to identify this possible complication. Our case highlights the possibility of clavicle fracture non-union even in very young children. It stressed the initial fracture displacement and lack of apposition being a common cause for this complication, even in the very young pediatric age group with abundant remodeling potential. This specific presentation also challenges the prevailing notion that non-union of clavicle fractures is almost non-existent in children under three, adding valuable data to the limited existing literature on this demographic [14,15,16].
The clavicle fracture managed non-operatively has a very high incidence of union with excellent functional outcome in the majority of patients. However, there is sporadic evidence of non-union warranting surgical intervention. The fracture displacements with lack of apposition most commonly result in this complication. The successful outcome in this 3-year-old male highlights the importance of a comprehensive approach that considers both fracture characteristics and patient factors, moving beyond age-centric treatment paradigms.
This report highlights the importance of awareness of this uncommon complication among clinicians, allowing a vigilant and fracture-specific plan of management for a better outcome.
References
- 1. Van Scoy GK, Sajadi KR, Uhl TL. Consequences of delayed surgical intervention of a displaced midshaft clavicle fracture: A case report. JSES Rev Rep Tech 2023;3:410-5. [Google Scholar] [PubMed]
- 2. Strong DH, Strong MW, Hermans D, Duckworth D. Operative management of clavicular malunion in midshaft clavicular fractures: A report of 59 cases. J Shoulder Elbow Surg 2019;28:2343-9. [Google Scholar] [PubMed]
- 3. Hughes K, Kimpton J, Wei R, Williamson M, Yeo A, Arnander M, et al. Clavicle fracture nonunion in the paediatric population: A systematic review of the literature. J Child Orthop 2018;12:2-8. [Google Scholar] [PubMed]
- 4. Gupta A, Singal RP, Singal R, Sahu P, Singal S, Gupta R, et al. Report of two cases of non-union of clavicle treated with nonsurgical management. North Am J Med Sci 2010;2:544-6. [Google Scholar] [PubMed]
- 5. Parry JA, Van Straaten M, Luo TD, Simon AL, Ashraf A, Kaufman K, et al. Is there a deficit after nonoperative versus operative treatment of shortened midshaft clavicular fractures in adolescents? J Pediatr Orthop 2017;37:227-33. [Google Scholar] [PubMed]
- 6. Schulz J, Moor M, Roocroft J, Bastrom TP, Pennock AT. Functional and radiographic outcomes of nonoperative treatment of displaced adolescent clavicle fractures. J Bone Joint Surg 2013;95:1159-65. [Google Scholar] [PubMed]
- 7. Caird MS. Clavicle shaft fractures: Are children little adults? J Pediatr Orthop 2012;32 Suppl 1:S1-4. [Google Scholar] [PubMed]
- 8. Strauss BJ, Carey TP, Seabrook JA, Lim R. Pediatric clavicular fractures: Assessment of fracture patterns and predictors of complicated outcome. J Emerg Med 2012;43:29-35. [Google Scholar] [PubMed]
- 9. Smith NW, Williams N. Post-traumatic nonunion of a clavicle fracture in a 9-year-old child. J Pediatr Orthop B 2016;25:74-7. [Google Scholar] [PubMed]
- 10. Rajnand K, Sujeet HK, Suresh C. A retrospective observational study to assess functional outcome of closed clavicle fractures treated with locking compression plate verses elastic intramedullary nail. Int J Sci Study 2025;12:11-4. [Google Scholar] [PubMed]
- 11. Ropars M, Bey M, Bouin M, Chapuis M, Bracq H, Violas P. Pseudarthrose d’une fracture de clavicule chez l’enfant. Rev Chir Orthop Réparatrice Appar Mot 2004;90:666-9. [Google Scholar] [PubMed]
- 12. O’Neill BJ, Molloy AP, Curtin W. Conservative management of paediatric clavicle fractures. Int J Pediatr 2011;2011:172571. [Google Scholar] [PubMed]
- 13. Adamich J, Howard A, Camp M. Do all clavicle fractures in children need to be managed by orthopedic surgeons? Pediatr Emerg Care 2018;34:706-10. [Google Scholar] [PubMed]
- 14. Stewart SK. Fracture non-union: A review of clinical challenges and future research needs. Malays Orthop J 2019;13:1-10. [Google Scholar] [PubMed]
- 15. Niikura T, Lee SY, Sakai Y, Nishida K, Kuroda R, Kurosaka M. Causative factors of fracture nonunion: The proportions of mechanical, biological, patient-dependent, and patient-independent factors. J Orthop Sci 2014;19:120-4. [Google Scholar] [PubMed]
- 16. Jerome JT. Combined intrafocal K-wire pinning for unstable pediatric distal forearm fractures. J Musculoskelet Surg Res 2025;9:379-86. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 September 1, 2025 Non-union Hoffa’s fracture in an Adult Male managed with Total Knee Arthroplasty : A Rare Case Report
September 1, 2025 Non-union Hoffa’s fracture in an Adult Male managed with Total Knee Arthroplasty : A Rare Case Report October 1, 2024 Non-union Patella Fracture – Extensor Mechanism Repair with Quadriceps Release: A Case Report
October 1, 2024 Non-union Patella Fracture – Extensor Mechanism Repair with Quadriceps Release: A Case Report February 10, 2021 Non -Union of Lateral Hoffa Fracture – A Case Report
February 10, 2021 Non -Union of Lateral Hoffa Fracture – A Case Report March 1, 2026 Salvage of a Broken Magnetic Tibia Nail with Plate Fixation Without Nail Removal: A Case Report
March 1, 2026 Salvage of a Broken Magnetic Tibia Nail with Plate Fixation Without Nail Removal: A Case Report