
Incidental contralateral imaging can reveal benign bone lesions such as non-ossifying fibromas, and careful radiological pattern recognition allows safe conservative management while avoiding unnecessary invasive intervention.
Dr. Muhammed Vally, Department of Orthopaedics, Chris Hani Baragwanath Academic Hospital, University of the Witwatersrand, Johannesburg, South Africa. E-mail: cerezvally@gmail.com
Introduction: Bone tumours are rare neoplastic disorders, with their infrequent malignant counterparts posing significant risks to child and adolescent morbidity and mortality. Thus, appropriate recognition and distinction of such lesions remain pivotal. In the South African context, where local epidemiological data remain limited, this case enhances clinical awareness and highlights the importance of specialist referral and ongoing surveillance.
Case Report: We report a case of an 18-year-old scholar in whom an X-ray evaluation for an old sports injury to the left knee revealed an incidental benign bone tumour of the contralateral distal femur. Radiographs were obtained to assess the affected knee, and a control X-ray of the opposite limb unexpectedly demonstrated a distal femoral lesion, prompting further orthopaedic evaluation. Radiological findings suggested a benign bone tumour, and based on imaging characteristics, multiple non-ossifying fibromas were diagnosed. Given the absence of symptoms and radiological signs of aggressiveness, a conservative management plan with serial imaging was adopted.
Conclusion: This case underscores the value of contralateral imaging and vigilance in distinguishing benign from malignant lesions in adolescents.
Keywords: Non-ossifying fibroma, incidental bone tumour, adolescent musculoskeletal neoplasms, skeletal neoplasms, aneurysmal bone cysts.
Primary bone tumours are rare among other neoplastic disorders, accounting for approximately 0.2% of tumours recorded in the National Cancer Institute’s Surveillance, Epidemiology, and End Results registry (2024) [1]. However, despite its infrequent incidence, malignant primary bone tumours are a pertinent contributor to cancer morbidity and mortality, ranking among the top five causes of cancer-related deaths in the child and adolescents age groups [1]. Recognition and distinction of such malignancies from its more frequent, benign counterparts remain pivotal, particularly within the primary healthcare setting, in which referral to a specialist, multidisciplinary team is necessitated. Thus, in this article, we underscore an approach to bone tumours and its benign manifestations, as illustrated through a patient with an incidental benign bone tumour identified in clinical practice on the contralateral side to that of injury and symptomatology.
An 18-year-old South African adolescent with no significant medical history presented to the outpatient orthopaedics clinic at a tertiary academic hospital with a 5-year history of intermittent left knee discomfort and instability. These symptoms followed a sporting injury involving a collision to the lateral aspect of the knee. The patient described intermittent cramping pain localized to the medial knee, exacerbated by intense activity but mild in intensity and without limitation to daily activities. He reported no constitutional or infectious symptoms, family history of malignancy, radiation exposure, or occupational risks. On examination, he appeared well, with no stigmata of chronic illness. Systemic assessment was unremarkable, with musculoskeletal examination of both knees revealing a normal gait with no obvious deformities and full range of motion with no signs of meniscal, ligamentous, or bony injury in either limb. Given the chronic, non-specific knee pain, plain radiographs were performed. The symptomatic left knee appeared normal (Fig. 1).

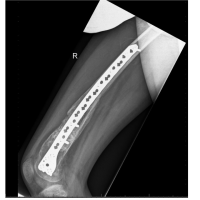
Figure 1: Initial anteroposterior (AP) radiograph showing distal femoral non-ossifying fibromas. AP radiograph of both knees obtained at the initial presentation. The right distal femur demonstrates three well-defined, eccentric, cortically based metaphyseal lucent lesions with thin sclerotic margins and internal septations. The largest lesion shows mild cortical expansion without cortical breach, periosteal reaction, or soft-tissue involvement. The left knee appears radiographically normal, confirming the contralateral and incidental nature of the right-sided lesions. These imaging features are consistent with multiple non-ossifying fibromas.
Unexpectedly, the contralateral right distal femur showed three eccentric metaphyseal hypodense lesions. The largest was multi-septated, with geographic bone destruction, thin sclerotic margins, and a protruding cortex. All lesions displayed a narrow transition zone, preserved joint space, and no soft-tissue involvement or features suggesting malignancy (Fig. 1).
These findings were most consistent with multiple non-ossifying fibromas (NOFs) of the right distal femur. Differential diagnoses included an aneurysmal bone cyst (ABC) or chondromyxoid fibroma (CMF), though both typically present with pain and swelling, supporting NOF as the likely diagnosis in this asymptomatic limb.
Advanced imaging, such as magnetic resonance imaging, was recommended for further characterisation but deferred in favour of conservative management given the benign features and lack of symptoms. In addition, targeted radiographic surveillance was initiated, with repeat imaging planned at 3-month intervals to monitor lesion evolution and determine the need for further intervention. The patient and family were counseled regarding this approach and advised to report any new symptoms. At follow-up, the patient remained asymptomatic with no red-flag features. Repeat right knee radiographs (Fig. 2 & 3) showed no change in the lesions’ appearance, morphology, or size, confirming the diagnosis of multiple NOFs.

Figure 2: Anteroposterior radiograph of the right knee at follow-up.
AP radiograph of the right knee obtained at follow-up demonstrates multiple well-defined, eccentric, cortically based metaphyseal lucent lesions in the distal femur. The lesions maintain thin sclerotic margins and internal septations, with mild cortical expansion but no cortical breach, periosteal reaction, or associated soft-tissue abnormality. There is no interval change in size or morphology compared with the initial study, supporting lesion stability and a benign diagnosis consistent with non-ossifying fibromas.

Figure 3: Follow-up lateral radiograph demonstrating lesion stability. Lateral radiograph of the right knee obtained at 3-month follow-up. The previously identified distal femoral lesions show no interval change in size, morphology, cortical integrity, or margins. There is no new periosteal reaction or soft-tissue abnormality. These findings support the benign nature of the lesions and justify continued conservative management with radiographic surveillance.
Primary bone tumours are uncommon neoplasms derived from primitive bone cells, with limited epidemiological data in the Southern African context. Globally, they display a bimodal age distribution – peaking in adolescence and late adulthood, with a slight male predominance. Most are benign, with malignant forms remaining rare but prognostically severe. Considering their asymptomatic and incidental nature, early radiological recognition is essential for distinguishing benign from aggressive lesions [2,3]. Radiographic evaluation provides key clues to biological behavior. According to Lodwick’s classification, patterns of bone destruction progress from geographic (well-defined and slow growing) to moth-eaten and permeative (aggressive) [4,5]. Benign tumours usually show sclerotic margins and a narrow zone of transition, whereas malignant lesions have ill-defined borders and cortical breach. Similarly, periosteal response reflects growth rate: slow lesions form smooth, uninterrupted periosteal reactions, whereas rapid ones yield lamellated or spiculated appearances or, if growth exceeds callus deposition, a Codman triangle [6,7]. In addition, soft-tissue extension further signals aggressive behavior. In this case, the patient’s lesions demonstrated a geographic pattern, sharp margins, intact cortex, and absent soft-tissue component – features consistent with a benign process. The radiological and clinical constellation supported a diagnosis of multiple NOFs, the most common benign bone tumour of childhood, with a prevalence up to 30% [6]. NOF typically arises incidentally in the metaphyseal cortices of long bones; most often the distal femur, knee, and proximal tibia [7,8,9]. They tend to either occur in isolation or, rarely, as part of syndromes such as Neurofibromatosis Type 1 or Jaffe-Campanacci [10]. Radiographically, NOF appears as an eccentric, cortically based, lucent lesion with a thin sclerotic rim. Lesions may be staged using the Ritschl classification, from early cortical lucencies (Stage A) to eventual sclerosis and resolution (Stage D) [10]. Because malignant transformation does not occur, management is conservative, relying on periodic plain-film surveillance (3–6-monthly) until sclerosis or involution. The main differential diagnoses, ABC and CMF, are usually symptomatic. ABC presents with acute pain and swelling, shows expansile multiloculated radiolucencies, and may arise secondarily within other lesions such as NOF [2]. CMF, an exceedingly rare benign tumour of cartilaginous origin, manifests with intermittent pain, cortical erosion, and histological myxoid stroma [2]. Both are usually managed surgically, unlike NOF’s expectant approach.
Primary bone tumours are rare among neoplastic disorders, with malignant forms posing a significant risk to child and adolescent morbidity and mortality. Through this case review, in which an incidental bone tumour (NOF) was unravelled contralateral to the symptomatic side of injury, the pivotal principles of evaluation of bone tumours are expounded upon, underlining the differentiating features of benign and malignant bone neoplasms. Thus, appropriate referral and orthopaedic management are vital within our South African context, in which there is a recognized dearth of local epidemiological exploration into child and adolescent bone tumours.
Asymptomatic, radiologically benign bone lesions in adolescents can be managed conservatively with surveillance, provided malignant features are confidently excluded through careful imaging assessment.
References
- 1. Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024. CA Cancer J Clin 2024;74:12-49. [Google Scholar] [PubMed]
- 2. Franchi A. Epidemiology and classification of bone tumours. Clin Cases Miner Bone Metab 2012;9:92-5. [Google Scholar] [PubMed]
- 3. Abril Martín JC, Arroba PM. Most common bone tumours. Pediatr Integr 2024;28:260-5. [Google Scholar] [PubMed]
- 4. Caracciolo JT, Temple HT, Letson GD, Kransdorf MJ. A modified Lodwick-Madewell grading system for the evaluation of lytic bone lesions. AJR Am J Roentgenol 2016;207:150-6. [Google Scholar] [PubMed]
- 5. Benndorf M, Bamberg F, Jungmann PM. The Lodwick classification for grading growth rate of lytic bone tumours: A decision tree approach. Skelet Radiol 2021;51:737-45. [Google Scholar] [PubMed]
- 6. Herget GW, Mauer D, Krauß T, El Tayeh A, Uhl M, Südkamp NP, et al. Non-ossifying fibroma: Natural history with an emphasis on a stage-related growth, fracture risk and the need for follow-up. BMC Musculoskelet Disord 2016;17:147. [Google Scholar] [PubMed]
- 7. Pretell-Mazzini J, Zhang J. Benign bone lesions in children: General characteristics and management options. Curr Orthop Pract 2013;24:590-7. [Google Scholar] [PubMed]
- 8. Paulos J. Non-ossifying fibroma. In: Bone Tumours: Diagnosis and Therapy Today. Cham: Springer; 2021. p. 139. [Google Scholar] [PubMed]
- 9. Bonifazi E. Non-ossifying fibroma of bone and ipsilateral hypermelanic nevus. An example of the relationship between skeletal and pigment abnormalities. Eur J Pediatr Dermatol 2013;23:168-71. [Google Scholar] [PubMed]
- 10. Błaż M, Palczewski P, Swiątkowski J, Gołębiowski M. Cortical fibrous defects and non-ossifying fibromas in children and young adults: The Analysis of radiological features in 28 cases and a review of literature. Pol J Radiol 2011;76:32-9. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 March 10, 2024 Operative Treatment of a Patient with a Pathological Fracture through a Large Non-ossifying Fibroma: A Case Report
March 10, 2024 Operative Treatment of a Patient with a Pathological Fracture through a Large Non-ossifying Fibroma: A Case Report January 10, 2024 Primary Aneurysmal Bone Cyst in the Iliac Bone: A Case Report
January 10, 2024 Primary Aneurysmal Bone Cyst in the Iliac Bone: A Case Report July 10, 2023 Atypical Presentation of Non-Ossifying Fibroma in a Professional Muay Thai Boxer: A Case Report and a Narrative Review of the Literature
July 10, 2023 Atypical Presentation of Non-Ossifying Fibroma in a Professional Muay Thai Boxer: A Case Report and a Narrative Review of the Literature February 10, 2022 Fibrocartilaginous Dysplasia – A Report of Five Cases with Review of Literature
February 10, 2022 Fibrocartilaginous Dysplasia – A Report of Five Cases with Review of Literature