
Iatrogenic neck femur fracture can occur as a complication of intramedullary nailing and such a complication can be dealt with the miss-a-nail technique.
Dr. Nehal Salgaokar, Department of Orthopaedic Surgery, Goa Medical College, Bambolim, Goa, India, E-mail: nehalshrikantsalgaokar@gmail.com
Introduction: Femur shaft fractures are common fractures that orthopedic surgeons come across. Intramedullary nailing is the most frequently used modality of management for shaft of femur fractures. Fracture of the femoral neck is an unusual complication while performing Intramedullary nailing of a shaft fracture.
Case Report: A 28-year-old male with a history of motor vehicular accident suffered a left shaft of femur fracture for which the patient got operated with intramedullary nailing. Post-operative X-ray revealed an iatrogenic neck femur fracture. Patient then referred to a higher center and got operated for the same.
Conclusion: There are many techniques to treat missed iatrogenic neck femur fracture. One such technique is to put miss-a-nail compression screw to achieve good compression at the neck site.
Keywords: Iatrogenic, fracture neck, intramedullary nailing, miss-a-nail screw.
Intramedullary interlocking nailing is the standard choice of treatment for isolated femoral shaft fractures. Ipsilateral neck of femur fractures are an unusual complication following intramedullary nailing of femoral shaft fractures, most commonly occurring due to technical difficulties. Wrong positioning, Wrong entry point, inadequate entry point reaming, inadequate shaft reaming in a tight canal, and hammering the nail are some of the causes for iatrogenic neck femur fracture. The treatment of such fractures is done by placement of compression screws into the head of the femur around the proximal end of the nail, known as the “Miss-a-nail” technique [1]. Miss-a-nail technique is where the intramedullary interlocking nail is not removed and then Cancellous cannulated screws are put by missing the nail across the fracture site of the neck, such that the compression is achieved as well as reduction is maintained. Another method could be to remove the interlocking nail and change to Proximal femoral nail (PFN-A1); however, there is a chance of displacement of neck fractures while removing and inserting, hence, losing the reduction. The Miss-a-nail technique is technically more difficult comparatively [3,4].
A 28-year-old male presented to the emergency department of district hospital after a motor vehicular accident, sustaining injury to the left thigh on June 12, 2025. X-ray confirmed a fracture of the shaft of the femur (Fig. 1). He did have any injury to the head, neck, chest, or abdomen, nor any other bony injury. He was then admitted for the same and got operated for a shaft femur fracture on June 15, 2025.

Figure 1: Anteroposterior radiograph of left thigh and of pelvis showing fracture of left shaft femur. When he presented 1st time in casualty there is NO neck fracture.
Post-operative X-ray was done, and it revealed a fracture of the neck of the femur. X-ray also revealed distraction at the fracture site (Fig. 2). Patient post-operative day 2 developed fever and respiratory distress and saturation 96% on room air, followed by which the patient referred to Goa Medical College, Bambolim, on June 17, 2025 in view of suspected fat embolism.
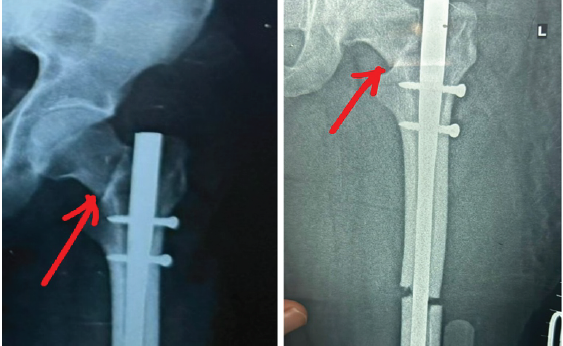
Figure 2: Immediate post-operative radiograph of the hip after the first surgery revealed iatrogenic neck femur fracture (marked with red arrow in figure 2) along with distraction at the shaft femur fracture site, which was not corrected after the first surgery.
Patient was hemodynamically stable with Blood pressure of 130/80 mmhg and saturation of 97% on room air. Any other injury was ruled out and he was then admitted in Goa Medical College on June 17, 2025. Investigations revealed low hemoglobin of 9.2 g/dL; the rest of the investigations, including Renal and liver function tests, were normal. Computed tomography pulmonary angiography was done to rule out pulmonary embolism and was found to be normal. He was kept on 4L oxygen with a facemask and low molecular weight heparin till the operation. After omitting heparin 12 h before the surgery, the patient was then taken to OT on June 21, 2025 under combined epidural and spinal anesthesia. Two important things, which had to be addressed: First, to reduce distraction at the shaft fracture and second, the neck fracture. The patient was positioned on a traction table. The same incision was used. First, the femur nail tip was felt and identified and then the femur jig was connected to it. Then, both the proximal bolts were removed to backslap the nail till the fracture site gap of the shaft got reduced, and then only the proximal dynamic bolt was put. Now, for neck fracture, two 6.5 mm Cannulated Cancellous screws (one with a washer) were passed from the neck to the head of the femur. Both the screws have to be put in the posterior quadrant as the entry of the femur nail was found to be a little anterior. Good compression was achieved at both the fracture sites (Figs. 3 and 4).

Figure 3: Intraoperative C-arm shoots of hip anteroposterior and lateral views and the shaft anteroposterior view shows two cannulated cancellous screws for neck femur, screws are in the posterior quadrant, as nail entry was anterior fracture gap at shaft was reduced and only proximal dynamic bolt inserted.
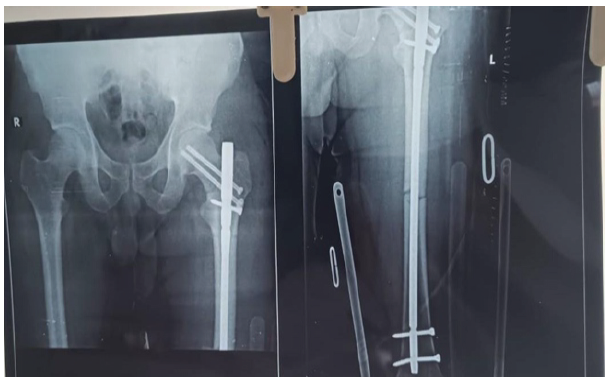
Figure 4: Immediate post-operative radiograph after the second surgery of the hip and full-length femur anteroposterior view showing miss-a-nail compression screws for the neck femur with fracture distraction reduced at the shaft.
Post-operatively patient was started with knee range of motion, bed-side sitting, and non-weight bearing with a walker. Serial X-rays were taken and it showed Good union at both the fracture site and NO avascular necrosis (AVN) changes in the head of the femur. After 2 months, the patient was advised to follow weight-bearing mobilization with the help of a walking cane and to continue knee and hip strengthening exercises. Patient is symptomatically better and has minimal pain over the operated limb.
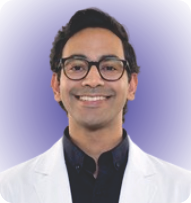
Patient post-operative follow-up at 6 months is walking comfortably without any walking aid and without any pain (Fig. 5).
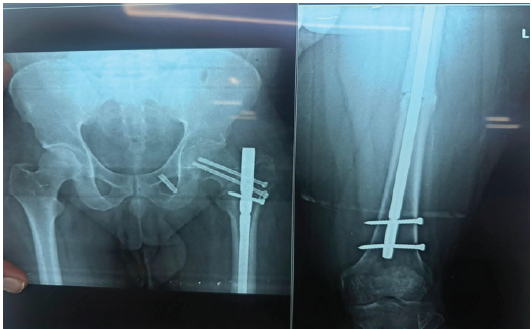
Figure 5: Six-month follow-up post-operative radiograph of the left hip and full-length femur anteroposterior view shows a united fracture of both neck and shaft of the femur. There is no evidence of avascular necrosis of the head and the patient is able to walk full weight bearing without any pain.
Early closed intramedullary nailing using locking bolts to enhance stabilization is now the preferred method of management for femur shaft fractures in adults [4]. Iatrogenic neck fracture is one of the complications following intramedullary nailing of the femur [1]. Treatment of isolated femur neck fractures is often performed with open or closed reduction with cannulated cancellous screw fixation [6]. With an anterograde femoral nail in situ, it complicates the fixation of the neck of the femur fracture. One option includes removing the previous implant before inserting the screws for the neck fractures. However, removing the implant may increase intra-operative time and difficulty in re-inserting the nail following screw fixation for the neck [7]. The other option includes fixation of the neck fracture by inserting cancellous screws with the anterograde nail in situ. This is done by using the Miss-a-nail technique [8]. Another technique for management of such a condition is to remove the femur intramedullary interlocking nail and change to a long PFN-A1, such that you get to reduce both fractures. Kow et al. described a somewhat similar technique but did not give the description and details of the procedure [7]. Wheeless. Miss-A-nail technique described the miss-a-nail technique, but did not show any comparison with other methods [8]. Challenges with this case were not only to address the neck femur fracture, along with that to reduce the distraction at the shaft femur fracture. This was done by first attaching the femur jig to the nail and back slapping the nail till the fracture gap got reduced and then two Cannulated Cancellous screws were put neck fracture. The entry point of the nail was not changed; hence, screws for the neck were inserted posterior part of the neck as the nail was anteriorly placed. The reasons for an iatrogenic neck fracture during femoral nail include Wrong positioning of patient, wrong entry, the forceful use of an awl in wrong direction, multiple entry points in greater trochanter may weaken neck of femur such that subsequent insertion of the nail completes the fracture, inadequate entry point reaming, inadequate shaft reaming and hammering of the nail insertion jig [3]. Khan et al. conducted a study wherein the authors observed good functional outcomes in patients who sustained iatrogenic neck fractures while Intramedullary nailing of femoral shaft fractures, which were treated conservatively [2,9-11]. Various factors influence the healing process of neck fractures and management depends of the surgeon’s preference. Neck fractures, if treated improperly, often lead to AVN of the femoral head, non-union, coxa vara, secondary osteoarthritis of the hip joint, financial burden, and disability [5].
Surgeons must be aware of the intra-op complications of femoral shaft fractures during nailing, the most important being neck of femur fracture, and the miss-a-nail technique is an appropriate way of fixation of such fractures with intramedullary nail in situ.
Intraoperative complications, such as an iatrogenic neck fracture, can occur anytime. It is important to take necessary pre-cautions to avoid it, such as proper positioning the patient on a traction table, proper entry point both on Anteroposterior and lateral view on shoot X-rays, adequate entry point reaming as well as reaming one size larger the final nail size in a tight canal, and taking pre-cautions while hammering and back slapping the jig. Always take a shoot of the neck before closing the wound.
References
- 1. Grala P, Mankowski B, Kierzynka G. Femoral neck fracture following intramedullary nailing with misplacement of an end cup: Report of two cases. J Orthopaed Traumatol 2009;10:35-8. [Google Scholar] [PubMed]
- 2. Khan FA, Ikram MA, Badr AA, Al-Khawashki H. Femoral neck fracture: A complication of femoral nailing. Injury 1995;26:319-21. [Google Scholar] [PubMed]
- 3. Rudloff MI, Smith WR. Intramedullary nailing of the femur: Current concepts concerning reaming. J Orthop Trauma 2009;23:S12-7. [Google Scholar] [PubMed]
- 4. Christie J, Court-Brown C, Kinninmonth AW, Howie CR. Intramedullary locking nails in the management of femoral shaft fractures. J Bone Joint Surg Br 1988;70:206-10. [Google Scholar] [PubMed]
- 5. Dedrick DK, Mackenzie JR, Burney RE. Complications of femoral neck fracture in young adults. J Trauma 1986;26:932-7. [Google Scholar] [PubMed]
- 6. Yang KH, Choi YW, Won JH, Yoo JH. Subcapital femoral neck fracture after removal of gamma/proximal femoral nails: Report of two cases. Injury Extra 2005;36:245-8. [Google Scholar] [PubMed]
- 7. Kow RY, Abdul-Aziz A, Low CL. Miss-A-nail technique for neck of femur screw fixation: It is easier said than done. Malays Orthop J 2020;14:96-7. [Google Scholar] [PubMed]
- 8. Wheeless CR. Miss A Nail Technique: (Special Aiming Arm). North Carolina: Wheeless’ Textbook of Orthopaedic; 2012. Available from: https://www.wheelessonline.com/joints/miss-a-nail-technique- special-aiming-arm [Last assessed on 2022 Mar 05]. [Google Scholar] [PubMed]
- 9. Pauyo T, Drager J, Albers A, Harvey EJ. Management of femoral neck fractures in the young patient: A critical analysis review. World J Orthop 2014;5:204-17. [Google Scholar] [PubMed]
- 10. Protzman RR, Burkhalter WE. Femoral-neck fractures in young adults. J Bone Joint Surg Am 1976;58:689-95. [Google Scholar] [PubMed]
- 11. Davidson A, Blum S, Harats E, Kachko E, Essa A, Efraty R, et al. Neck of femur fractures treated with the femoral neck system: Outcomes of one hundred and two patients and literature review. Int Orthop 2022;46:2105-15 [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Comparative Analysis of Suprapatellar and Infrapatellar Nailing in Tibial Fracture: A Randomized Clinical Study
March 1, 2026 Comparative Analysis of Suprapatellar and Infrapatellar Nailing in Tibial Fracture: A Randomized Clinical Study January 1, 2026 The Importance of Closed Reduction and Internal Fixation done with Intramedullary Implants in Pathological Fractures – A Case Series
January 1, 2026 The Importance of Closed Reduction and Internal Fixation done with Intramedullary Implants in Pathological Fractures – A Case Series December 1, 2025 Management of a Case of Adult Mid-Shaft Femur Fracture in Osteogenesis Imperfecta by Long Proximal Femoral Nail: A Case report
December 1, 2025 Management of a Case of Adult Mid-Shaft Femur Fracture in Osteogenesis Imperfecta by Long Proximal Femoral Nail: A Case report November 1, 2025 Incidence and Functional Impact of Malrotation after Intramedullary Nailing of Femoral Shaft Fractures: A Prospective Computed Tomography-based Observational Study
November 1, 2025 Incidence and Functional Impact of Malrotation after Intramedullary Nailing of Femoral Shaft Fractures: A Prospective Computed Tomography-based Observational Study