
Atypical periprosthetic femur fractures should be considered and promptly investigated in patients on bisphosphonate therapy with post-operative pain. Minimally invasive prophylactic plating is an effective way to treat these fractures.
Dr. Shaunak S Patwardhan, Department of Trauma and Orthopaedics, Salford Royal Hospital, Salford, England. E-mail: patwardhanshaunak@gmail.com
Introduction: Periprosthetic fractures are excluded from Atypical Femur Fractures as per the report of American Society for Bone and Mineral Research. However, there are increasing reports demonstrating the existence of atypical periprosthetic femur fractures (APFF) which are related to chronic bisphosphonate use. Literature states that these fractures can be treated as per the atypical femur fracture treatment algorithm, and prophylactic fixation can be suitable to treat symptomatic incomplete fractures. An impending or incomplete APFF can be an important reason for post-operative lateral thigh pain, which needs to be kept in mind, appropriately investigated and treated. We present a case of Bisphosphonate-induced APFF treated with minimally invasive plating, leading to good clinical results and pain relief.
Case Report: In this case report, we present a 86-year-old female who came with a history of bilateral hip and knee arthritis and osteoporosis for which her General Practitioner had started her on bisphosphonates in the form of Ibandronic Acid 150 mg each month. The patient had undergone a right total hip replacement a year after, following which she was progressing well in the subsequent post-operative period. However, she developed new complaints of right thigh pain beginning 6–8 months post-operative. Investigations such as magnetic resonance imaging lumbar spine were done to rule out other causes, and also some therapeutic interventions, like US-guided injection to trochanter and gluteus tendon and physiotherapy were also tried, but unfortunately, provided no relief. Further imaging revealed features of impending APFF, and the patient underwent a prophylactic plating for the same after discussions in the regional arthroplasty multidisciplinary team meeting.
Conclusion: This case report highlights the possibility of APFF in elderly patients with post-operative thigh pain who have had a history of bisphosphonate use. When prophylactic nailing is not possible, spanning the length of the bone with minimally invasive plating gives good results and pain relief.
Keywords: Atypical fracture, bisphosphonate, MIPPO, plating, periprosthetic
Bisphosphonates are osteoclast inhibitors used to treat osteoporosis and other metabolic bone diseases. Although they have reduced the incidence of osteoporotic fractures, there is an increased risk of subtrochanteric and femoral shaft fractures amongst patients on long-term bisphosphonates [1,2]. There have been cases reported in literature of periprosthetic fractures associated with the use of bisphosphonates occurring in the long-term following a total hip replacement [3,4,5]. These periprosthetic fractures are excluded from atypical femur fractures as per the report of American Society for Bone and Mineral Research [1]. These fractures can be treated as per the atypical femur fracture treatment algorithm, and prophylactic fixation can be suitable to treat symptomatic incomplete fractures [3]. This case is an important reminder that bisphosphonate-induced atypical proximal femur periprosthetic fractures should be on the orthopedic surgeon’s differential diagnosis as an explanation for lateral thigh pain following total hip arthroplasty, especially for patients on long-term bisphosphonate therapy [4].
An 86-year-old female presented to the outpatient clinic with symptomatic of bilateral hip and knee arthritis. She was known to have osteoporosis for which her GP had started her bisphosphonates in the form of Ibandronic Acid 150 mg each month. The patient underwent a right total hip replacement almost a year after commencing bisphosphonate therapy (Fig. 1).

Figure 1: Post-operative X-ray after cemented total hip replacement – no obvious signs of atypical periprosthetic femur fractures.
Following this, she was progressing well in the subsequent post-operative period. However, she developed new complaints of right thigh pain, which were increasing over time. These new symptoms were initially noticed and gradually increased 6–8 months after the operation. She was continuing with the bisphosphonate therapy during this time. Investigations such as magnetic resonance imaging (MRI) lumbar spine were done to rule out other causes, including radicular pain due to nerve root compression. Therapeutic interventions like ultrasound-guided injection to the trochanter and gluteus tendon were tried, for possible trochanteric bursitis and gluteal tendinopathy, but unfortunately, provided no relief. Further imaging revealed features of impending atypical periprosthetic femur fractures (APFF) (Fig. 2), and the patient underwent a prophylactic plating for the same after discussion in the regional arthroplasty multidisciplinary team meeting (Fig. 3).

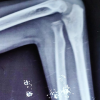
Figure 2: Interim X-ray when patient was symptomatic – showing features of atypical periprosthetic femur fractures and evident lateral beaking



Figure 3: Serial Post-operative X-rays after minimally invasive plating spanning the length of the femur – proximal screws through the cement mantle. (a) Immediate post-operative, (b) 3-month post-operative, (c) 6-month Post-operative.
Investigations
The patient underwent X-rays of the pelvis with bilateral hip, along with anteroposterior and lateral views of the right hip. Routine pre-operative blood investigations were done. X-rays had showed bilateral cortical thickening of the lateral cortex in the subtrochanteric region with lateral beaking. Subsequently, an MRI of the proximal femur also showed the presence of an incomplete atypical fracture of the left proximal femur with evidence of bridging and lateral cortical thickening; however, it was not possible to get an adequate assessment of the right proximal femur due to the metal artefact (hip prosthesis).
Treatment
The patient was put in the lateral position under general anesthesia and block with all aseptic precautions being followed strictly. The pre-operative protocol of the World Health Organisation checklist and administration of antibiotics was followed, and then the limb was prepared using an antibiotic solution and draped. A lateral incision was made over the proximal femur, and dissection was done in layers till the bone, and a submuscular plane was developed. A large fragment 18-holed LCP with staggered holes was used, and the plate was contoured to accommodate the bone and slid under the submuscular space. A distal incision was made, and the correct placement of the plate was confirmed, and proximal and distal screws were inserted. The proximal screws were staggered through the cement mantle by missing the stem in order to give it a stable fixation. Closure was done in layers, sterile dressing was applied, and final images were taken to confirm the plate and screw placement. The patient was then allowed to weight bear postoperatively without restriction from post-operative day 1.
Follow-up and outcome
The patient was followed up at 6 weeks postoperatively, and it was seen that the surgical site had healed well without any wound-related complications, and there was a complete resolution of right thigh pain. There was a pain-free active straight leg raise and right hip range of motion on follow-up at 6 weeks, and was also mobilizing well and engaging well with physiotherapists. The patient was also referred for a DEXA scan and a rheumatology evaluation to consider starting teriparatide and further medical management for the incomplete left-sided fracture. An orthopedic follow-up was also suggested, which included doing serial X-rays every 3 months for the left femur.
APFFs are fractures characterized by atypical features of atypical femoral fractures (AFF) and occur around femoral stem prostheses. Although both APFFs and AFFs would have a theoretically similar pathogenesis, only a few studies have addressed APFF patient characteristics [6], and previous studies showed that APFFs had significantly higher fracture-related complications compared to AFFs or typical periprosthetic femoral fractures. Although the original definition of AFF excludes periprosthetic fractures, similar bisphosphonate-associated fractures have also been reported in the setting of orthopedic implants. Lee et al. reported on 11 low-energy peri-implant (mostly plates and one periprosthetic stemmed total knee arthroplasty) fractures in 10 ambulant females, 48 months after the index surgery [7]. They hypothesized that dynamic strains under tension may be accentuated, contributing to local micro-damage that overwhelms the impaired healing capacity of the anti-resorptive-treated bone. There are also several case reports on similar fractures after total hip arthroplasty in patients on bisphosphonates, in spite of the intramedullary stems, analogous to an intramedullary fixation. These findings are important as the use of bisphosphonates has been paradoxically encouraged to increase the periprosthetic bone mineral density and improve implant survival in patients who have undergone a total joint arthroplasty of the lower limb [8]. Moreover, this may call for a revision of the definition of AFF or introduction of a newer entity, as these bisphosphonates-associated peri-prosthetic/peri-implant fractures appear similar to AFF in terms of etiology [9]. Sabsuantang et al., in their study, stated that regarding the treatment strategy, APFFs show a poor fracture healing potential and require special attention. Incomplete fracture has a poor-to-fair success rate and mostly requires prophylactic fixation with a plate and screws or revision arthroplasty in some cases. Complete fractures require optimization of the fixation strategy and using, if possible, local and systemic biological enhancement for improving treatment outcomes [10]. Concerning the treatment of incomplete APFFs, Sabsuantang et al. also demonstrated the high failure rate of conservative treatment, which was comparable to the results from a systematic review by De Cicco et al. the effectiveness of conservative treatment and prophylactic fixation in the incomplete APFFs was 40% (4 in 10) and 83% (5 in 6), respectively [11]. These results were comparable to the results from the systematic review of the treatment of AFFs by Koh et al., as the success rates of conservative treatment and prophylactic fixation in AFFs were 53% and 97%, respectively [11]. Toro et al. stated that it is important to underline that both complete and incomplete AFF are associated with a high risk of contralateral AFF [12]. Therefore, at least a contralateral femoral X-ray is recommended during hospitalization to early identify and treat an unknown AFF. In their cohort, two patients sustained a contralateral AFF 13 months after the initially reported APFF. Moreover, bisphosphonate use must be stopped to prevent the occurrence of contralateral fracture [12]. Early identification of both AFF and APFF can be performed using several imaging modalities such as DXA, MRI, and bone scan [12]. This latter might be the preferred modality in APFF, considering the possibility of metal artefacts that could obscure the fracture, especially if metal artefact reduction sequences for MRI are not considered [6]. Due to ever-increasing use of bisphosphonates for osteoporosis, APFF should be considered in patients who complain of thigh/hip pain even with intramedullary fixation or prostheses. It is also important to note that these patients may or may not be symptomatic until a complete fracture occurs. Therefore, regular clinical and radiological follow-up is encouraged and should be part of the discussion with the patient before surgical intervention. Moreover, stoppage of bisphosphonates, correction or modification of other risk factors, and implant selection are all important considerations.
This case report highlights the possibility of APFF in elderly patients with post-operative thigh pain who have had a history of bisphosphonate use. When prophylactic nailing is not possible, spanning the length of the bone with minimally invasive plating gives good results and pain relief.
• Surgeons should maintain a high index of suspicion for APFF in elderly patients with a history of bisphosphonate use with post-operative thigh pain
• Post-operative lateral thigh pain should be investigated appropriately – cortical thickening starts to show on X-rays early
• When prophylactic nailing is not possible, as this case – spanning the length of the bone with minimally invasive plating gives good results and pain relief.
References
- 1. Shane E, Burr D, Abrahamsen B, Adler RA, Brown TD, Cheung AM, et al. Atypical subtrochanteric and diaphyseal femoral fractures: Second report of a task force of the American society for bone and mineral research. J Bone Miner Res 2014;29:1-23. [Google Scholar] [PubMed]
- 2. MacKenzie SA, Ng RT, Snowden G, Powell-Bowns MF, Duckworth AD, Scott CE. Periprosthetic atypical femoral fractures exist and are associated with duration of bisphosphonate therapy. Bone Joint J 2019;101-B:1285-91. [Google Scholar] [PubMed]
- 3. Dózsai D, Ecseri T, Csonka I, Gárgyán I, Doró P, Csonka Á. Atypical periprosthetic femoral fracture associated with long-term bisphosphonate therapy. J Orthop Surg Res 2020;15:414. [Google Scholar] [PubMed]
- 4. Curtin BM, Fehring TK. Bisphosphonate fractures as a cause of painful total hip arthroplasty. Orthopedics 2011;34:e939-44. [Google Scholar] [PubMed]
- 5. Bhattacharyya R, Spence S, O’Neill G, Periasamy K. Bisphosphonate-induced periprosthetic fracture: A cause of painful total hip arthroplasty. Case Rep Surg 2014;2014:631709. [Google Scholar] [PubMed]
- 6. Robinson Jde D, Leighton RK, Trask K, Bogdan Y, Tornetta P 3rd. Periprosthetic atypical femoral fractures in patients on long-term bisphosphonates: A multicenter retrospective review. J Orthop Trauma 2016;30:170-6. [Google Scholar] [PubMed]
- 7. Lee JY, Soh T, Howe TS, Koh JS, Kwek EB, Chua DT. Bisphosphonate-associated peri-implant fractures: A new clinical entity? A series of 10 patients with 11 fractures. Acta Orthop 2015;86:622-6. [Google Scholar] [PubMed]
- 8. Bhandari M, Bajammal S, Guyatt GH, Griffith L, Busse JW, Schünemann H, et al. Effect of bisphosphonates on periprosthetic bone mineral density after total joint arthroplasty. A meta-analysis. J Bone Joint Surg Am 2005;87:293-301. [Google Scholar] [PubMed]
- 9. Maheshwari AV, Yarmis SJ, Tsai J, Jauregui JJ. Progression of bisphosphonate-associated impending atypical femoral fracture despite prophylactic cephalomedullary nailing: A case report and review of literature. J Clin Orthop Trauma 2016;7 Suppl 1:92-8. [Google Scholar] [PubMed]
- 10. Sabsuantang K, Chotanaphuti T, Wongsak S, Sa-Ngasoongsong P, Khuangsirikul S, Chulsomlee K, et al. Atypical periprosthetic femoral fracture associated with prolonged bisphosphonate therapy: A two-centered retrospective case series and literature review. Cureus 2022;14:e24514. [Google Scholar] [PubMed]
- 11. De Cicco A, Toro G, Oliva F, Tarantino U, Schiavone Panni A, Maffulli N. Atypical periprosthetic femoral fractures of the hip: A PRISMA compliant systematic review. Injury 2021;52:2407-14. [Google Scholar] [PubMed]
- 12. Toro G, Ojeda-Thies C, Calabrò G, Toro G, Moretti A, Guerra GM. Management of atypical femoral fracture: A scoping review and comprehensive algorithm. BMC Musculoskelet Disord 2016;17:227. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 October 1, 2025 Neglected Monteggia Fracture-Dislocation in an 8-Year-Old Child with Posterior Interosseous Nerve Palsy: A Case Report
October 1, 2025 Neglected Monteggia Fracture-Dislocation in an 8-Year-Old Child with Posterior Interosseous Nerve Palsy: A Case Report September 1, 2025 Periprosthetic Humeral Shaft Fracture about Total Elbow Arthroplasties Managed with Medial and Lateral Femoral Strut Allografts and Implant Retention: A Case Report
September 1, 2025 Periprosthetic Humeral Shaft Fracture about Total Elbow Arthroplasties Managed with Medial and Lateral Femoral Strut Allografts and Implant Retention: A Case Report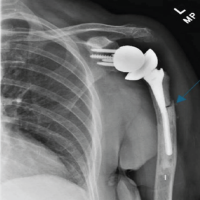 September 1, 2025 Transverse Periprosthetic Fracture With a Bent Stem Following Reverse Total Shoulder Arthroplasty – A Case Report
September 1, 2025 Transverse Periprosthetic Fracture With a Bent Stem Following Reverse Total Shoulder Arthroplasty – A Case Report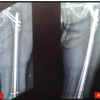 August 1, 2025 Fracture Occurrence following Prophylactic Nailing in a Case of Bisphosphonate-induced Atypical Femoral Fracture – A Rare Case Report
August 1, 2025 Fracture Occurrence following Prophylactic Nailing in a Case of Bisphosphonate-induced Atypical Femoral Fracture – A Rare Case Report