
Bent intramedullary nails can be successfully managed with minimally invasive percutaneous straightening techniques followed by exchange nailing.
Dr. Anaïs Labar, Department of Orthopedics and Traumatology, Hôpital Erasme–Université Libre de Bruxelles, Bruxelles, Belgium. E-mail: anais.m.labar@gmail.com
Abstract
Introduction: Bending of tibial intramedullary (IM) nails is an extremely rare complication, usually resulting from high-energy trauma. Management options are not standardized, and removal or exchange nailing can be technically challenging.
Case Report: We report the case of a 23-year-old male who sustained a displaced fracture of the left tibial shaft following a motorcycle accident. He was treated with closed reduction and IM nailing (9 mm), with uneventful recovery and fracture union at 6 months. One year later, the patient was involved in another motorcycle accident, leading to acute pain and deformity of the same tibia. Radiographs revealed significant bending of the previously implanted IM nail with a refracture at the former fracture site. Attempts to straighten the nail by counter-pressure against a tibial support and on an orthopedic traction table were unsuccessful. Using fluoroscopic guidance, the maximal bending point was identified and drilled percutaneously to weaken the nail. A Schanz pin was then inserted into the distal oval foramen after removal of a mediolateral screw, and horizontal traction was applied to gradually realign the nail. Following successful straightening, the bent nail was removed and replaced with a larger-diameter nail (10 mm) after reaming.
Conclusion: This case demonstrates that percutaneous straightening and subsequent exchange nailing is a safe and effective approach for managing bent IM nails. This minimally invasive technique reduces surgical morbidity while restoring stability and may serve as an alternative to complex extraction methods.
Keywords: Tibial fracture, intramedullary nail, bent nail, percutaneous drilling, exchange nailing.
Tibial shaft fractures are among the most common long bone injuries. These fractures represent a significant portion of all long bone fractures in adults, with an incidence that varies with age and mechanism of injury [1]. Intramedullary (IM) nailing is considered the gold standard of management due to its biomechanical stability and allowance of early weight-bearing [2,3]. While standard mechanical complications of tibial IM nailing include malalignment, delayed union, and hardware failure [4], post-traumatic bending of IM nails is extremely rare, with only a handful of cases described in the literature [5,6,7,8,9,10,11]. Bent nail removal is technically demanding because of implant deformation and limited surgical corridors [6]. We present a rare case of a bent tibial nail after a second high-energy motorcycle accident, managed successfully with fluoroscopy-guided percutaneous weakening, controlled straightening, and exchange nailing.
Initial injury and management
A 23-year-old male presented after a motorcycle accident with a displaced left tibial shaft fracture (Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association 42–A3). He underwent closed reduction and IM nailing with a standard 9-mm titanium nail. Post-operative recovery was uneventful with radiographic union at 6 months.
Reinjury
Twelve months later, he sustained another motorcycle accident (high-energy trauma), developing acute pain and visible deformity of the left leg (Fig. 1).

Figure 1: Clinical photograph showing visible deformity of the left lower limb following high-energy motorcycle trauma. Note the characteristic angulation at the tibial shaft level corresponding to the bent intramedullary nail position.
Radiographs revealed a markedly bent IM nail at the distal-third of the diaphysis and a refracture at the prior union site. The deformity measured approximately 17° anteroposterior and 15° mediolateral (Fig. 2). The skin was intact; there were no signs of compartment syndrome or neurovascular compromise.

Figure 2: Sagittal computed tomography image demonstrating the bent tibial intramedullary nail with measurement of angular deformity. The nail shows approximately 17° of anteroposterior angulation at the distal third of the tibial diaphysis, with refracture at the previous union site.
Operative technique
Under general anesthesia and fluoroscopic guidance, we first attempted closed straightening by counter-pressure against a tibial support and then on a traction table. Both attempts were unsuccessful. We then identified the point of maximal bending by fluoroscopy to define the percutaneous drilling zone. Through a small incision, we weakened the nail using a transcutaneous drill (6.5 mm diameter; Fig. 3) near the bend apex through the fracture site.

Figure 3: The 6.5-mm extraction drill bit from the Operace series (Swiss Tools) used for percutaneous weakening of the bent nail at the point of maximal deformity under fluoroscopic guidance.
Next, a Schanz pin was inserted through the distal oval foramen of the nail after removal of a mediolateral screw, and horizontal traction was applied to progressively straighten the implant. After realignment, the nail was removed as a single piece, using the standard extraction technique, and exchanged for a larger-diameter (10-mm) tibial titanium nail following canal reaming.
Post-operative course
The patient followed partial weight-bearing for 4 weeks, then advanced weight bearing as tolerated. At 8 months, he was pain-free, had returned to sports, and radiographs showed maintained alignment with intact fixation (Fig. 4). Wound healing was uneventful, including at the percutaneous drilling site.

Figure 4: Follow-up lateral radiograph at 8 months postoperatively showing complete fracture union with preserved bone alignment and intact fixation following exchange nailing with the larger-diameter (10-mm) tibial nail.
Bent IM nails are rare and most often occur after high-energy trauma [5,6,7,8,9,10,11]. While mechanical complications of IM nails generally include cutout, delayed union, implant fracture, and malalignment [4], nail bending represents a singular complication requiring specialized management approaches. Extraction of a deformed implant can be technically challenging, with options including open osteotomy, partial cutting of the nail, or complex extraction devices [7,8]. Our case highlights a minimally invasive alternative: percutaneous drilling near the maximal bending point, combined with controlled traction to restore alignment before safe extraction. This approach avoids extensive bone resection, preserves soft tissues, and shortens operative time compared to open techniques [5,6,7,11]. The minimally invasive percutaneous nature of this technique may also contribute to better fracture healing by preserving the local biological environment and fracture hematoma, which are essential for optimal bone consolidation [2,6]. The exchange to a larger-diameter nail after reaming provides additional stability, consistent with biomechanical studies supporting nail size optimization in tibial fractures [2,3]. This case supports previously reported strategies for bent nail management [6,7,11] and demonstrates that fluoroscopy-guided percutaneous straightening is reproducible, safe, and effective.
Bent tibial IM nails represent an uncommon but challenging complication. This case demonstrates that fluoroscopy-guided percutaneous drilling, straightening with controlled traction, and exchange nailing is a minimally invasive and effective option. Surgeons should consider this strategy before proceeding to more aggressive extraction techniques.
Bent IM nails following high-energy trauma can be successfully managed using fluoroscopy-guided percutaneous drilling and controlled straightening techniques, avoiding complex open extraction procedures while preserving soft tissues and reducing surgical morbidity.
References
- 1. Court-Brown CM, Caesar B. Epidemiology of adult fractures: A review. Injury 2006;37:691-7. [Google Scholar] [PubMed]
- 2. Trafton PG. Tibial shaft fractures. In: Browner BD, Jupiter JB, Levine AM, Trafton PG, editors. Skeletal Trauma: Basic Science, Management, and Reconstruction. 5th ed. Philadelphia, PA: Saunders Elsevier; 2015. p. 2039-117. [Google Scholar] [PubMed]
- 3. Xia L, Zhou J, Zhang Y, Mei G, Jin D. A meta-analysis of reamed versus unreamed intramedullary nailing for the treatment of closed tibial fractures. Orthopedics 2014;37:e332-8. [Google Scholar] [PubMed]
- 4. Manon J, Detrembleur C, Van De Veyver S, Tribak K, Cornu O, Putineanu D. Predictors of mechanical complications after intramedullary nailing of tibial fractures. Orthop Traumatol Surg Res 2019;105:523-7. [Google Scholar] [PubMed]
- 5. Mousley JJ, Kjar R, Reidy M, Lambers A. Closed management of a bent tibial nail: Can revision be avoided?: A case report. JBJS Case Connect 2025;15:e24.00379. [Google Scholar] [PubMed]
- 6. Apivatthakakul T, Chiewchantanakit S. Percutaneous removal of a bent intramedullary nail. Injury 2001;32:725-6. [Google Scholar] [PubMed]
- 7. Kose O, Guler F, Kilicaslan OF, May H, Yuksel HY. Removal of a bent intramedullary nail in lower extremity: Report of two cases and review of removal techniques. Arch Orthop Trauma Surg 2016;136:195-202. [Google Scholar] [PubMed]
- 8. Arif H, Molina S, LeBrun C. Removal of a bent tibial intramedullary nail through osteotomy and partial sectioning: A case report. JBJS Case Connect 2023;13:e23.00186. [Google Scholar] [PubMed]
- 9. Gaubert L, Breda R. Removal of a bent tibial intramedullary nail: A case report and a review of the literature. Clin Case Rep Int 2019;3:1097. [Google Scholar] [PubMed]
- 10. Aggerwal S, Soni A, Saini UC, Gahlot N. Removal of a bent tibial intramedullary nail: A rare case report and review of the literature. Chinese J Traumatol 2011;14:107-10. [Google Scholar] [PubMed]
- 11. Suh YS, Lee WS, Ahn J, Choi HS, Baek MJ, Choi SW. Removal of bent intramedullary nail. Medicine (Baltimore) 2020;99:e19935. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Endoscopic Flexor Hallucis Longus Tenotomy for Post-traumatic Checkrein Deformity: A Case Report
February 1, 2026 Endoscopic Flexor Hallucis Longus Tenotomy for Post-traumatic Checkrein Deformity: A Case Report December 1, 2025 New Gen Halifax Nail with Novel Tri-Wire Concept for Intertrochanteric Fracture
December 1, 2025 New Gen Halifax Nail with Novel Tri-Wire Concept for Intertrochanteric Fracture December 1, 2025 Correlation between Biochemical Parameters and Radiographic Healing Score in Tibial Fractures
December 1, 2025 Correlation between Biochemical Parameters and Radiographic Healing Score in Tibial Fractures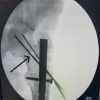 October 1, 2025 Miss-a-nail Technique of Femur Neck Fracture with Femur Interlocking Nail in Situ: A Technical Description
October 1, 2025 Miss-a-nail Technique of Femur Neck Fracture with Femur Interlocking Nail in Situ: A Technical Description