
Navigated percutaneous fixation using large porous 3D-printed screws provides a safe and effective minimally invasive option for acetabular fractures in elderly osteoporotic patients.
Mr. Matthew Rohl, Department of Orthopaedic Surgery, Ohio University Heritage College of Osteopathic Medicine, Dublin, Ohio, USA. E-mail: mr067923@ohio.edu
Introduction: Acetabular fractures in elderly patients are often the result of low-energy trauma and are complicated by osteopenia, comorbidities, and limited physiologic reserve. Minimally invasive approaches, such as percutaneous fixation have emerged as viable alternatives to open reduction in selected fracture patterns.
Case Report: We report the case of a 76-year-old male with a history of coronary artery disease, hypertension, hyperlipidemia, and osteopenia who sustained a comminuted right anterior column and posterior hemitransverse acetabular fracture following a ground-level fall. His hospital course was complicated by rhabdomyolysis and elevated troponin levels, necessitating cardiac evaluation, which demonstrated normal left ventricular function and no evidence of valvular disease. Given the fracture pattern and his polytrauma status, including an ipsilateral proximal humerus fracture and multiple rib fractures, he underwent navigated percutaneous screw fixation of the right acetabulum using O-arm-assisted guidance and iFuse TORQ TNT Screws (SI-Bone, Santa Clara, California).
Outcome: The patient recovered well without perioperative or post-operative complications. Radiographs at 6 months post-operatively demonstrated fracture healing and stable hardware. He achieved independent ambulation with full, pain-free, passive right hip range of motion.
Conclusion: This case highlights the successful application of image-guided percutaneous fixation in an elderly patient with polytrauma and poor bone quality. The use of 3-dimensional navigation and larger-diameter porous screws may offer a biomechanical advantage with improved fixation in osteoporotic acetabulum fractures. Further studies are warranted to evaluate long-term outcomes in this patient population.
Keywords: Acetabular fracture, navigation, percutaneous fixation.
In younger patients, acetabular fractures tend to result from high-energy trauma. However, in the elderly population, these injuries may occur even after low-energy mechanisms, such as ground-level falls, mainly due to osteopenia and age-related structural changes in the pelvis [1]. As the population ages, these fractures are becoming increasingly common and pose significant management challenges, particularly in patients with multiple comorbidities or poor bone quality. Operative fixation in geriatric patients must balance the goals of fracture stabilization and early mobilization against the risks of invasive surgery. Minimally invasive techniques, including percutaneous screw fixation, have gained traction in selected fracture patterns, offering a less morbid approach with acceptable outcomes [2,3]. The use of intraoperative navigation and 3-dimensional (3D) imaging with O-arm-assisted guidance can facilitate precise screw placement, especially in osteoporotic bone, where traditional tactile cues may be limited and radiographic visualization may be obscured. We present the case of a 76-year-old male with a comminuted right anterior column and posterior hemitransverse acetabular fracture sustained after a ground-level fall. The patient was treated successfully with navigated percutaneous screw fixation using intraoperative O-arm imaging with large diameter screws. This case highlights the success of image-guided minimally invasive stabilization in the elderly population. It underscores the importance of individualized surgical planning in the setting of severe osteopenia and associated injuries.
A 76-year-old male with a medical history of coronary artery disease, hypertension, hyperlipidemia, osteoarthritis of bilateral hips, osteopenia, and prior inguinal hernia repair presented to our institution 2 days after a fall from standing height. He was a daily smoker and consumed alcohol regularly. The fall resulted in multiple closed injuries, of which included a right acetabular fracture, right proximal humerus fracture, and rib fractures in right ribs 8–12. Of note, there were no neurovascular injuries recorded. His initial hospital course was complicated by rhabdomyolysis and a modestly elevated troponin level. On exam, the patient had pain while sitting and during pelvic squeeze on evaluation. The right lower extremity demonstrated intact sensation to light touch in all lower extremity dermatomes, palpable dorsalis pedis and posterior tibial pulses, brisk capillary refill, and full motor strength in the extensor hallucis longus, flexor hallucis longus, tibialis anterior, and gastrocnemius-soleus complex. He had no evidence of incontinence or bladder injury. Radiographs and computerized tomography (CT) revealed a comminuted, minimally displaced, anterior column and posterior hemitransverse fracture of the right acetabulum, along with fractures of the right superior and inferior pubic rami as seen in Fig. 1a and b.
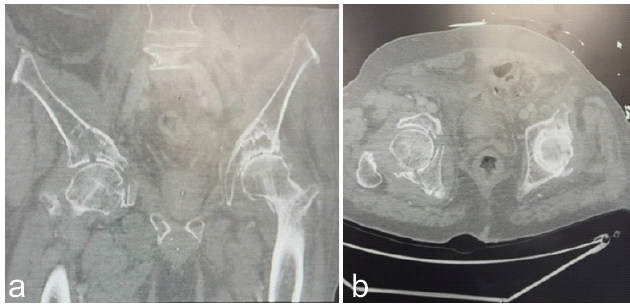
Figure 1: (a and b) Axial and coronal images from a pre-operative computed tomography-scan of the pelvis demonstrating a right anterior column and posterior hemitransverse acetabular fracture.
Additional injuries included a displaced right proximal humerus fracture and right-sided rib fractures involving ribs 8–12. The decision was ultimately made to proceed with operative fixation of the acetabulum to restore alignment and stability, while improving pain and allowing early mobility. The patient was taken to the operating room for percutaneous fixation the following day. The fractures to the right ribs 8–12 were managed non-operatively with pulmonary hygiene exercises and a multimodal pain regimen. Following percutaneous screw fixation, his post-operative protocol included touch-down weight bearing through the right lower extremity with activity as tolerated. He continually worked with physical therapy while inpatient, and his pain slowly improved each day. After addressing his injuries, the patient was discharged on post-operative day 9 to a skilled nursing facility.
Technique
The patient was placed in the supine position following induction of general anesthesia. A small flat bump was placed directly under the midline of the patient’s sacrum to slightly elevate the patient’s pelvis relative to the bed. A standard surgical time-out was performed. Navigation reference guide pins were percutaneously inserted into the left ilium, and initial intraoperative O-arm imaging was used to confirm appropriate visualization of the acetabular corridors. A small incision was made, and dissection was carried down to the bone in the usual fashion. Utilizing a navigation-assisted cannulated guide, a guidewire was inserted for the 8.7 mm iFuse TORQ TNT screws (SI-Bone, Santa Clara, CA) in an antegrade fashion along the anterior column under CT-navigated guidance and confirmed to be safely positioned on a repeat O-arm spin. After safe confirmation of the screw in the osseous fixation pathway, a 140 mm iFuse TORQ TNT screw was inserted with satisfactory placement confirmed on C-arm fluoroscopy. A second guidewire was placed in a retrograde fashion along the posterior column using the same technique, with O-arm imaging used to confirm proper positioning before screw placement. A 150 mm TNT screw was placed across the posterior column. Final fluoroscopic and O-arm images confirmed stable fixation with no cortical breaches as seen in Fig. 2a and b.
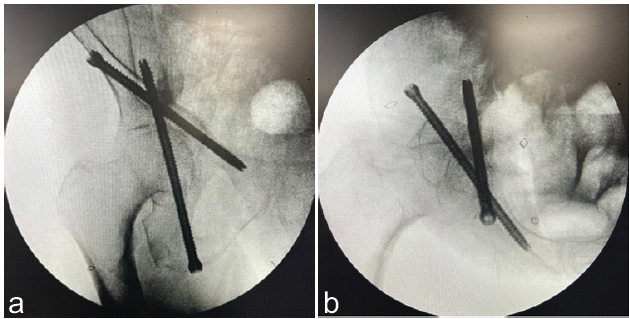
Figure 2: (a and b) Intraoperative fluoroscopy 2 views showing both the anterior column (140 mm) screw and posterior column (150 mm) screw.
Intraoperatively, the bone was noted to be markedly osteopenic. All wires were removed, wounds were irrigated and closed in a layered fashion, and sterile dressings were applied. The patient was hemodynamically stable for the entire duration of the procedure and was transferred to the intensive care unit in stable condition post-operatively. Post-operatively, he received antibiotics according to our institutional protocol and deep vein thrombosis prophylaxis as directed by the primary medical team with Lovenox. He maintained touch down weight bearing (TDWB) as tolerated on the right lower extremity for 6 weeks, with immediate range-of-motion as tolerated (ROMAT) to minimize stiffness. At his first follow-up visit, 4-weeks post-operatively, Judet views of the pelvis demonstrated maintained alignment of the acetabulum with no evidence of hardware loosening or failure as seen in Fig. 3a and b. Incisions were fully healed and the plan was to continue TDWB with ROMAT and follow-up in 3 weeks for repeat imaging.
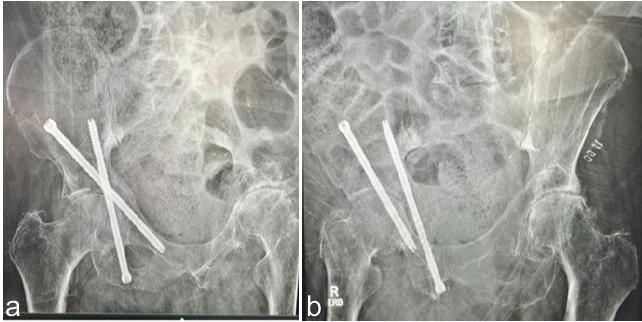
Figure 3: (a and b) 4-week postoperative Judet view radiographs.
At 9-weeks post-operatively, radiographs showed progressive healing of the acetabular fracture. At this point, the patient was instructed to begin physical therapy and continue ambulating unassisted as tolerated. At 6 months post-operatively, radiographs showed a well-aligned and well-healed acetabular fracture with hardware in a stable position. The patient was satisfied with his pain control and back to full hip range of motion in flexion/extension/internal rotation/external rotation, and was back to performing all activities of daily living near his pre-injury level.
This case illustrates the successful use of navigated percutaneous fixation for a comminuted anterior column and posterior hemitransverse acetabular fracture in a polytrauma osteopenic patient utilizing large diameter screws. Open reduction and internal fixation (ORIF) of displaced acetabular fractures can be associated with increased surgical risks, including greater blood loss, prolonged operative time, and risk of neurovascular injury [2,4,5]. In this case, the patient’s advanced age, poor bone quality, and multiple associated injuries made a minimally invasive approach more favorable to reduce his relative operative risks. The SI-Bone iFuse TORQ TNT implants used for fixation in this case are unique. These are 3D printed 8.7 mm porous threaded titanium screws, designed for sacroiliac joint fusions and pelvic fracture fixation in geriatric patients, as well as revision settings. Conventionally, smaller 6.5 mm, 7.3 mm, and 8.0 mm diameter cannulated screws have been used for percutaneous acetabular fixation [6,7]. The larger 8.7 mm diameter and porous design may be advantageous for stronger fracture fixation and pull-out strength, particularly in osteoporotic bone. With the larger implant size, intraoperative navigation was critical to achieving safe screw placement and minimizing the risk of cortical breach or neurovascular injury. In this case, the estimated blood loss was only 15 mL. This is substantially lower than previously reported values for open fixation of acetabular fractures [8]. While blood loss can vary based on patient factors and fracture complexity, this case supports existing evidence that percutaneous fixation is associated with reduced intraoperative blood loss, shorter operative times, and less soft tissue trauma compared to ORIF [3,9]. Other studies support that percutaneous fixation can yield equivalent reduction and functional outcomes to ORIF with low rates of infections and other complications [3,9,10,11]. Qi et al. found that Harris Hip Scores were not significantly different between percutaneous fixation compared to ORIF at 6-months post-operatively (82.28 vs. 84.78, P = 0.075) [11]. Einhorn et al. found that patients undergoing percutaneous screw fixation for acetabular fractures had a shorter length of hospital stay (P = 0.009), blood loss (P < 0.001), complications (P = 0.029) compared to similar patients undergoing ORIF [9]. They also found no significant difference in Harris Hip Scores at (P = 0.87) [9]. Our findings are consistent with prior studies demonstrating the efficacy of percutaneous fixation in elderly patients. Intraoperative navigation for pelvic screw placement has emerged as a valuable alternative to traditional fluoroscopic guidance. Navigated screws are common, particularly in spine surgery, where they have been shown to be safe and allow accurate screw placement [12]. For pelvic fracture fixation, navigated screws have become increasingly popular and have demonstrated accurate screw placement with good clinical outcomes [13,14]. A recent study comparing O‑arm navigation to conventional fluoroscopy for pelvic fragility fractures showed fewer screw perforations when using O‑arm navigation [15]. While both fluoroscopic and navigated methods can yield good clinical outcomes, navigation offers particular advantages for patients with poor bone quality or in scenarios where fluoroscopy may be challenging due to obesity, abdominal gas, stool, or complex fracture patterns. This case highlights how navigation was used to safely place larger 8.7 mm screws in an elderly patient with poor bone quality. To our knowledge, this is among the first published cases using navigation-assisted SI-Bone iFuse TORQ TNT implants for anterior and posterior column fixation in an acetabulum fracture. The patient achieved a satisfactory clinical outcome without significant complications. At 6-months post-operatively, radiographs confirmed fracture union with stable hardware. Functionally, he was ambulating without restrictions and reported minimal pain. This application of the implant demonstrates its potential use for select patients, especially polytrauma or elderly patients who may not tolerate open fixation. Future studies with larger sample sizes and longer follow-up are needed to determine the effectiveness, long-term outcomes, and long-term durability of this implant for its use in acetabular fixation.
This case demonstrates a unique use of navigated SI-Bone iFuse TORQ screws for percutaneous fixation of an anterior column and posterior hemitransverse acetabular fracture in an elderly polytrauma patient. The patient showed radiographic union and functional recovery at 6 months without complications. This technique, utilizing larger porous 3D-printed screws, offers a promising minimally invasive alternative to traditional open fixation for acetabular fractures, especially for elderly patients with osteoporosis. This case adds to the evidence supporting navigated percutaneous acetabular fixation and the potential for adapting implant technology to address complex orthopedic trauma.
For orthopedic trauma surgeons, achieving stable fixation in osteoporotic acetabular fractures can be challenging. Navigation-assisted percutaneous fixation using large porous screws may improve screw placement accuracy and fixation strength while reducing perioperative risks, making it a minimally invasive option for elderly polytrauma patients.
References
- 1. Park KC, Oh CW, Kim JW, Oh HK, Shon HC, Kim JJ, et al. Acetabular fractures in elderly. J Orthop Sci 2023;28:376-9. [Google Scholar] [PubMed]
- 2. Crowl AC, Kahler DM. Closed reduction and percutaneous fixation of anterior column acetabular fractures. Comput Aided Surg 2002;7:169-78. [Google Scholar] [PubMed]
- 3. Bozzio AE, Wydra FB, Mitchell JJ, Ackerson RM, Mauffrey C. Percutaneous fixation of anterior and posterior column acetabular fractures. Orthopedics 2014;37:675-8. [Google Scholar] [PubMed]
- 4. Krappinger D, Freude T, Stuby F, Lindtner RA. Acetabular fractures in geriatric patients: Epidemiology, pathomechanism, classification and treatment options. Arch Orthop Trauma Surg 2024;144:4515-24. [Google Scholar] [PubMed]
- 5. Wan Y, Yao S, Chen K, Zeng L, Zhu F, Sun T, et al. Treatment of anterior column posterior hemitransverse fracture with supra-ilioinguinal approach. J Int Med Res 2021;49:300060520982824. [Google Scholar] [PubMed]
- 6. Wong JM, Bewsher S, Yew J, Bucknill A, De Steiger R. Fluoroscopically assisted computer navigation enables accurate percutaneous screw placement for pelvic and acetabular fracture fixation. Injury 2015;46:1064-8. [Google Scholar] [PubMed]
- 7. Caviglia H, Mejail A, Landro ME, Vatani N. Percutaneous fixation of acetabular fractures. EFORT Open Rev 2018;3:326-34. [Google Scholar] [PubMed]
- 8. Ravanbod H, Alikhani B, Baniasadi M, Masoumi H. Comparative analysis of surgical approaches in acetabular fractures: Blood loss and procedural efficiency. J Orthop 2024;61:61-5. [Google Scholar] [PubMed]
- 9. Einhorn S, Höch A, Osterhoff G, Josten C, Kleber C, Pieroh P. Comparison of percutaneous screw fixation to open reduction and internal fixation in acetabular fractures: A matched pair study regarding the short-term rate of conversion to total hip arthroplasty and functional outcomes. J Clin Med 2023;12:1163. [Google Scholar] [PubMed]
- 10. Gary JL, VanHal M, Gibbons SD, Reinert CM, Starr AJ. Functional outcomes in elderly patients with acetabular fractures treated with minimally invasive reduction and percutaneous fixation. J Orthop Trauma 2012;26:278-83. [Google Scholar] [PubMed]
- 11. Qi X, Zhang X, Zhang Q, Zhang Y, Huang S, Lv Y, et al. Clinical efficacy and biomechanical analysis of robotic internal fixation with percutaneous screws in the treatment of both-column acetabular fractures. Sci Rep 2025;15:22908. [Google Scholar] [PubMed]
- 12. Matur AV, Palmisciano P, Duah HO, Chilakapati SS, Cheng JS, Adogwa O. Robotic and navigated pedicle screws are safer and more accurate than fluoroscopic freehand screws: A systematic review and meta-analysis. Spine J 2023;23:197-208. [Google Scholar] [PubMed]
- 13. Ciolli G, Caviglia D, Vitiello C, Lucchesi S, Pinelli C, De Mauro D, et al. Navigated percutaneous screw fixation of the pelvis with O-arm 2: Two years’ experience. Med Glas (Zenica) 2021;18:309-15. [Google Scholar] [PubMed]
- 14. Florio M, Capasso L, Olivi A, Vitiello C, Leone A, Liuzza F. 3D – navigated percutaneous screw fixation of pelvic ring injuries – a pilot study. Injury 2021;52:1103. [Google Scholar] [PubMed]
- 15. Mizutani M, Kotani T, Ogawa R, Yano S, Kishida S, Okuwaki S, et al. Comparison of the O-arm-based navigation system with conventional fluoroscopy for percutaneous screw fixation in patients with fragility fractures of the pelvis. Eur J Trauma Emerg Surg 2025;51:221. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 A Case Report on Unclassified Anatomical Sciatic Nerve Variant in Acetabulum Fracture
March 1, 2026 A Case Report on Unclassified Anatomical Sciatic Nerve Variant in Acetabulum Fracture February 1, 2026 Arthroscopic-Assisted Removal of Incarcerated Fragment following Manual Reduction of Posterior Hip Dislocation in Acute Polytrauma Patient: A Case Report
February 1, 2026 Arthroscopic-Assisted Removal of Incarcerated Fragment following Manual Reduction of Posterior Hip Dislocation in Acute Polytrauma Patient: A Case Report December 1, 2025 The use of an Antiprotrusio Cage in Acetabular Reconstruction for Periprosthetic Transverse Fracture through a Direct Anterior Approach: A Case Report
December 1, 2025 The use of an Antiprotrusio Cage in Acetabular Reconstruction for Periprosthetic Transverse Fracture through a Direct Anterior Approach: A Case Report December 1, 2025 Total Hip Arthroplasty for Neglected Hip Dislocation – Surgical Technique and Results
December 1, 2025 Total Hip Arthroplasty for Neglected Hip Dislocation – Surgical Technique and Results