
Total hip arthroplasty is achievable with satisfactory outcomes in resource-limited settings when locally adapted solutions, appropriate patient selection, and experienced surgical teams are implemented.
Dr. Cedrick Sangwa Milindi, Orthopedic and Traumatology Unit, University of Lubumbashi, Lubumbashi, Democratic Republic of Congo. E-mail: cedrickmilindiscotte@gmail.com
Introduction: Total hip arthroplasty (THA) is well established in high-income countries but remains challenging in sub-Saharan Africa due to limited implant availability, inadequate infrastructure, and financial constraints. This study presents a 7 year experience of THA in Lubumbashi, Democratic Republic of Congo, focusing on both clinical outcomes and the strategies developed to overcome local challenges.
Materials and Methods: We retrospectively analyzed 60 THAs performed on 58 patients (mean age 53.8 years) between 2017 and 2024 at Medpark Clinic. The main indication was femoral head osteonecrosis (71.6%), including 11 cases in patients with sickle cell disease. All procedures used a transgluteal approach, with implant choice adapted to bone quality and availability. Rehabilitation emphasized early mobilization despite limited physiotherapy resources.
Results: At a mean follow-up of 4.5 years, functional outcomes improved markedly, with the Postel-Merle d’Aubigné score rising from 6.4 preoperatively to 16.2 at six months. Excellent or good results were achieved in 90.7% of cases. Complications occurred in 17.2% of patients, including dislocations (6.6%), infections (6.6%), periprosthetic fractures (3.3%), aseptic loosening (3.3%), one pulmonary embolism (1.6 %), and two deaths (3.3%). Challenges and solutions: Barriers included high implant costs and irregular supply, addressed through long-term supplier partnerships and flexible payment plans. Infection control limitations were mitigated by strict asepsis protocols, povidone-iodine lavage, and selective use of antibiotic-loaded cement. In the absence of formal rehabilitation centers, structured patient and family education with early weight-bearing protocols facilitated recovery. Socioeconomic barriers were partially alleviated by forfait-based pricing and community financing mechanisms.
Conclusion: Despite significant structural and economic constraints, THA can be safely and effectively implemented in resource-limited African settings when supported by careful surgical planning, tailored implant strategies, strict infection control, and innovative solutions to financial and logistical barriers
Keywords Total Hip Arthroplasty, Avascular Necrosis, Resource-Limited Settings, Sub-Saharan Africa, Surgical Outcomes
Total hip arthroplasty (THA) is the gold standard for managing advanced hip pathologies, offering effective pain relief and durable functional restoration [1]. Common indications include osteoarthritis [1,2], femoral neck fractures [3], and osteonecrosis of the femoral head [4]. While THA is routinely performed in high-income countries [5], its availability in sub-Saharan Africa, including the Democratic Republic of Congo (DRC), remains severely limited [6,7]. In the DRC, several barriers continue to restrict access to THA: insufficient hospital infrastructure, scarcity of trained orthopedic surgeons, high implant costs, and the absence of universal health coverage [8]. In addition, many patients present late due to socioeconomic disparities, long travel distances, and the persistence of traditional therapeutic practices, resulting in advanced joint destruction and technically demanding surgical cases.
Lubumbashi, the second-largest city in the DRC and the capital of the former Katanga mining province [9], serves as a tertiary referral center with expanding surgical capacity. Yet, only a few institutions currently perform joint replacement procedures, and access remains far below population needs.
In this context, the present study reports a seven-year series of 60 total hip arthroplasties performed at Medpark Clinic in Lubumbashi. The objectives were to describe patient demographics and surgical indications, evaluate postoperative complications, assess implant survival, and analyze functional recovery using the Merle d’Aubigné–Postel (PMA) score [10] in a resource-limited environment.
Patients
From February 2017 to March 2024, a total of 60 total hip arthroplasties (THAs) were performed on 58 patients at Medpark Clinic, a level IV referral hospital in Lubumbashi affiliated with the University of Lubumbashi. Established in 2016, the clinic serves as a national reference center for joint replacement and maintains regular collaboration with specialists from Kinshasa and South Africa. The first THA was performed in February 2017, marking Medpark Clinic as a pioneer institution for hip and knee arthroplasty in the region. This cross-sectional descriptive study combined retrospective and prospective components and received approval from the University of Lubumbashi Ethics Committee (Ref. UNILU/CEM/131/2022). Specifically, retrospective data (2017-2021) were extracted from hospital records, while prospective follow-up evaluations (2022-2024) were conducted through scheduled clinical and radiological assessments. Surgical indications were established based on clinical presentation and radiographic criteria (Table 1). Two patients underwent bilateral procedures (Figure 1). The most frequent indication was Ficat stage [11] III-IV osteonecrosis (n = 43), comprising 11 sickle-cell disease cases, three post-traumatic, two HIV-related, and 27 idiopathic etiologies (Figure 2). Additional indications included eight primary osteoarthritis cases, three post-traumatic sequelae, four femoral-neck fractures, and two revision surgeries (one for severe heterotopic ossification, one for aseptic loosening of a Charnley prosthesis). Notable individual cases included one patient with sequelae of childhood sciatic-nerve injury and three obese patients (mean BMI = 36 kg/m²). During the same period, 110 hip-related operations were performed at the institution, with THAs accounting for approximately 66 % of all hip procedures (average 15-16 per year).
Method
All patients were admitted one day prior to surgery for preoperative evaluation and digital radiographic planning. Preoperative assessment included femoral canal templating, determination of the osteotomy level, limb-length measurement, and acetabular orientation analysis. Magnetic resonance imaging (MRI) was used selectively, while pelvic computed tomography (CT) was reserved for complex or revision cases. Each patient underwent a pre-anesthetic evaluation and HIV screening. All surgeries were performed under general anesthesia in climate-controlled, aseptic operating rooms. Anticoagulant therapy was discontinued 48 hours before surgery. Tranexamic acid (500 mg IV) was administered at anesthetic induction to minimize intraoperative blood loss. Antibiotic prophylaxis consisted of ceftriaxone 2 g IV combined with gentamicin 240 mg IV, administered within 60 minutes before incision and repeated after 24 hours. Thromboembolic prophylaxis included enoxaparin 40 mg subcutaneously once daily for 10 -14 days, extended up to 28 days in high-risk patients such as those with obesity, sickle-cell disease, or prolonged immobility. A restrictive transfusion policy was applied, with red-blood-cell transfusion reserved for hemoglobin < 8 g/dL or symptomatic anemia, and autologous reinfusion was performed whenever feasible (Table 2). These measures collectively aimed to minimize infection, bleeding, and thromboembolic risks while optimizing perioperative safety within resource limitations. All procedures were performed by the same surgical team using a standardized lateral trans-gluteal (Hardinge) approach with the patient in the supine position (Figure 3). Acetabular preparation systematically preceded femoral implantation (Figures 4 and 5). Implant systems from Meril® (India) and Gruppo Bioimplants® (Italy) were used according to patient anatomy and bone quality. Metal-on-polyethylene bearings predominated, while ceramic heads were reserved for younger or more active patients to enhance wear resistance. Cemented fixation was preferred for elderly or osteoporotic bone, and uncemented fixation for adequate bone stock. Dual-mobility cups and long stems were reserved for complex or revision cases. Implant integrity was verified before each procedure: sterile packaging, color indicators, lot-number traceability, and expiry dates were checked, and any compromised implant was excluded. In revision or infection-suspected cases, intraoperative deep-tissue cultures were obtained; gentamicin-loaded cement and targeted antibiotic therapy (15–30 days) were used according to microbiological results. Negative-pressure wound therapy was applied to selected cases with delayed healing or confirmed infection. Among the 60 hips, 58 (96.7 %) were primary THAs and 2 (3.3 %) were revision procedures, one for aseptic loosening of a Charnley prosthesis and one for severe heterotopic ossification requiring excision and reimplantation. Additionally, two patients with periprosthetic fractures underwent reimplantation, and two unstable implants were temporarily stabilized with anti-dislocation bracing and plaster boots.
Rehabilitation Protocol
Postoperative rehabilitation was initiated on postoperative day 1 under the supervision of a trained physiotherapist. The early phase included ankle-pumping exercises, quadriceps isometric contractions, and sitting-balance training to stimulate venous return and prevent early stiffness. From day 2 to day 3, patients began transfer training and assisted ambulation using crutches or a walking frame, while strictly maintaining hip-precaution measures, avoidance of flexion beyond 90°, adduction past midline, and internal rotation. Full weight-bearing as tolerated was generally authorized from day 3, except in revision or osteoporotic cases, where partial weight-bearing was maintained for approximately six weeks. Before discharge, each patient received a structured home-exercise program, which included active hip abduction, straight-leg raises, and progressive endurance walking performed twice daily. Follow-up physiotherapy visits were scheduled weekly for six weeks to ensure adherence and correct technique.
In the absence of specialized rehabilitation centers, family members were trained to assist patients with daily exercises and postural adjustments. This community-based rehabilitation approach, adapted to local constraints, proved both practical and effective in promoting functional recovery and reintegration.
Evaluation clinic and radiologic
Clinical and radiologic evaluations were performed at 30, 90, and 180 days postoperatively, and annually thereafter. Functional outcomes were assessed using the Merle d’Aubigné–Postel (PMA) score, which evaluates pain, mobility, and gait. Limb-length discrepancy was recorded both pre- and postoperatively, and prosthesis survival was determined by identifying any failures requiring revision surgery. Infections were classified as early (< 3 months) or late (≥ 3 months) according to the Musculoskeletal Infection Society (MSIS) criteria [12], requiring at least one of the following: a positive intra-operative culture, purulent drainage, or a sinus tract communicating with the prosthesis. Dislocation was defined as any postoperative loss of hip reduction confirmed both clinically and radiographically; events occurring within three months of surgery were categorized as early, and those occurring beyond that period as late dislocations. Standardized anteroposterior (AP) pelvic and lateral hip radiographs were obtained at each follow-up. All images were acquired using digital radiography under consistent patient positioning and exposure settings. Acetabular component orientation was considered satisfactory when the inclination angle ranged between 40° and 50° and anteversion between 10° and 20°, with at least 70 % host-bone coverage. Femoral stem alignment was evaluated on AP radiographs, with varus or valgus deviation defined as greater than 3° from the mechanical axis. Aseptic loosening was diagnosed when progressive radiolucent lines ≥ 2 mm appeared in at least two De Lee–Charnley zones (acetabular) [13] or two Gruen zones (femoral) [14], or when component migration ≥ 2 mm was observed compared with immediate postoperative radiographs. Osteolysis was defined as focal endosteal bone loss not attributable to infection or physiological remodeling. All radiographs were independently reviewed by two orthopedic surgeons blinded to the patients’ clinical outcomes. Any discrepancies were resolved through consensus review.
Statistical analysis:
Data were analyzed using Epi Info™ software version 7.2. Continuous variables were expressed as mean ± standard deviation (SD), while categorical variables were summarized as frequencies and percentages.
Epidemiological and clinical profile
A total of 58 patients (60 hips) were included in the study. The mean age at surgery was 53.8 years (range 17-79 years), with a clear male predominance (39 men and 21 women; sex ratio = 1.85) (Table 3). The left hip was involved in 33 cases and the right hip in 25. The mean duration of symptoms prior to surgery was 3 years (range 1-10 years). Preoperative limb shortening was present in 50 patients, averaging 2.5 cm (range 1-6 cm). Residual shortening persisted in five patients postoperatively, two of whom required a 2 cm shoe lift to restore gait symmetry. Wound healing was achieved by postoperative day 15 in 48 patients (83 %). The median hospital stay was 10 days (range 5-15 days). The mean follow-up duration was 4.5 years (range 5-72 months). Follow-up completeness was satisfactory throughout the study. At 6 months, 58 of 60 patients (96.7 %) were reviewed; at 1 year, 52 (86.7 %); at 3 years, 48 (80 %); and at 5 years, 45 (75 %). Losses to follow-up were mainly attributed to patient relocation or socioeconomic constraints. Two patients emigrated abroad, but were last seen walking independently without assistive devices (Table 4). Two deaths occurred during the follow-up period. The first involved a 53-year-old man who developed an early postoperative dislocation, requiring revision with gentamicin-loaded cement and cerclage wiring. He subsequently developed a deep periprosthetic infection, progressing to sepsis and death two months after the revision. This event was considered surgery-related. The second death occurred in a 73-year-old dialysis patient who experienced massive gastrointestinal bleeding on postoperative day 5. Despite intensive care management, he succumbed to hypovolemic shock. This event was deemed non-surgery-related, but highlights the fragility of patients with major comorbidities in resource-limited environments.
Implant characteristics (Table 5)
Metal-on-polyethylene bearings were used in 53 hips (88.3 %), while ceramic-on-polyethylene combinations were chosen in 5 hips (8.3 %), mainly in younger or more active patients to improve wear resistance. Dual-mobility cups were used in three high-risk cases, two revision surgeries and one obese patient, to minimize postoperative instability. Femoral head diameters measured 28 mm in 53 cases (88.3 %) and 32 mm in 7 cases (11.7 %). Larger heads were preferred in obese or high-demand patients to enhance joint stability and range of motion. Fixation type was cemented in 17 hips (28 %), predominantly among elderly or osteoporotic patients, and uncemented in 43 hips (72 %) with adequate bone stock. Most femoral stems corresponded to sizes 3-5 with a 125° neck-shaft angle.
Complications (Table 6)
Twelve patients (17.2%) experienced complications. (Table 3)
Dislocations (n=4): One obese female (BMI 38) had two dislocations early on; revision with a dual mobility cup and correction of inclination to 45° was successful. Another patient required femoral neck lengthening during revision. Two others were managed with closed reduction and bed rest. No late dislocations occurred.
Infections (n=4): Two were associated with revision surgery after prior fractures (figure 6), and two were superficial infections in immunocompromised patients (HIV, diabetes), managed with debridement and negative pressure therapy.
Hematoma (n=1): A 72-year-old man developed a hematoma from an unrecognized intraoperative fracture. He underwent osteosynthesis and received a long femoral stem. Deep infection ensued and was managed with vacuum therapy and gentamicin beads.
Pulmonary embolism (n=1): A 68-year-old woman experienced PE on day four. She was admitted to intensive care and recovered after anticoagulant therapy.
Aseptic loosening (n=2): Affected a 26-year-old with sickle cell disease and a 68-year-old man, occurring five- and six-years post-op, respectively (figure 7 a and b).
Functional outcomes
The average PMA score improved from 6.4 preoperatively to 16.2 at six months. Outcomes were excellent in 46 patients (80%), very good in 5 (8.3%), fair in 3 (5%), and poor in 2 (3.3%) (Table 7)
Epidemiological and clinical profile
Over a seven-year period, 60 total hip arthroplasties were performed in Lubumbashi, representing approximately 15% of major orthopaedic procedures at our center. This volume remains modest when compared with global standards and reflects the broader regional realities (Table 8). In the Democratic Republic of Congo, THA activity is concentrated in a limited number of tertiary facilities, mainly in large urban centers, and remains accessible only to a small proportion of the population due to structural, financial, and human-resource constraints [15,16]. Evidence from sub-Saharan Africa further highlights the scarcity of arthroplasty services: a systematic review conducted outside South Africa identified only 606 THAs reported across 12 published studies, underscoring the limited availability of joint replacement surgery in the region [6]. Neighbouring francophone countries such as Burundi and the Republic of the Congo also report low procedural volumes, with THA performed sporadically or replaced by less costly alternatives because of restricted technical capacity and resource limitations [17,18]. In the DRC specifically, recent institutional reports have emphasised the major infrastructural, training, and implant-cost barriers that hinder the establishment and sustainability of THA programmes, even in urban centers [8]. In stark contrast, high-income countries have witnessed a sustained expansion in arthroplasty services over the past decade. In OECD (Organisation for Economic Co-operation and Development) member states, THA incidence is estimated at approximately 190-200 procedures per 100,000 inhabitants per year [5]. In France, utilisation rates have shown a steady upward trend in recent years [19], while in England and Wales the annual number of primary THAs reached approximately 105,306 in 2017 [20]. This continuous growth is largely attributed to population ageing, advancements in surgical techniques, and earlier management of degenerative joint disease, all of which contribute to timely intervention and improved long-term outcomes [21]. In our cohort, the mean age of patients was 53.8 years, which aligns with reports from other sub-Saharan African countries, where the average age at THA is consistently lower than in Western populations, including series from Malawi [7,22], Ghana [23], Cameroon [24,25], Burkina Faso [26], Mali [27-29], Togo [30], Gabon [31], and Senegal [32]. This markedly younger patient profile contrasts with Western series, in which the mean age at primary THA commonly exceeds 70 years [33-35]. The age discrepancy largely reflects the high burden of aseptic osteonecrosis of the femoral head (71.6% of cases in our study), frequently associated with sickle-cell disease, post-traumatic sequelae, or infectious comorbidities such as HIV and tuberculosis [15,22,24,25,28]. A mean diagnostic delay of five years was observed, resulting in advanced joint destruction at presentation and increased surgical complexity. Similar delays ranging from 4 to 7 years have been reported in several African series (Table 8), and are predominantly attributed to limited access to specialist orthopedic care, prohibitive out-of-pocket costs, low levels of public awareness, and prolonged initial reliance on traditional medicine. The male predominance observed in our cohort is consistent with findings from other African studies and may be explained by higher exposure of men to trauma and risk factors for avascular necrosis. Of particular relevance, the high prevalence of sickle-cell disease, a major public health concern in Central Africa, contributes to earlier onset and faster progression of osteonecrosis, compromises bone quality, and negatively influences mid-term arthroplasty outcomes [36,37].
Implant-related challenges and adaptive strategies
Limited implant availability remains one of the major constraints to the development of total hip arthroplasty in the DRC. The absence of local manufacturing and the reliance on imported devices lead to high acquisition costs, recurrent stock shortages, and logistical delays, making arthroplasty accessible only to a privileged socio-economic minority [15]. In response to these systemic barriers, Medpark Clinic implemented a collaborative procurement model through a strategic partnership with Meril® and Gruppo Bioimplants®, which secured a more reliable supply of implants adapted to local morphologies. This initiative illustrates how locally driven strategies can reinforce equity of access to THA in low-resource settings [38]. Technical decisions were guided by a pragmatic and patient-centered approach, considering both evidence-based practice and contextual limitations. The anterolateral (transgluteal) approach was systematically adopted, consistent with its reported safety and reproducibility in similar African settings [15,22,25,27]. Metal-on-polyethylene bearings were preferred for their durability [39] and cost-effectiveness, while ceramic-on-polyethylene was selectively used in younger patients to optimize long-term survivorship. Fixation strategies were individualized: cemented implants were used in elderly patients with poor bone quality, whereas uncemented designs were favored in younger individuals with satisfactory bone stock. Progressive adaptations included the selective use of antibiotic-loaded cement, particularly in high-risk patients [40], and the introduction of dual-mobility cups to reduce instability in risk patients.
Complications
A total of twelve complications were recorded, representing an overall rate of 17.2%, which is comparable to that reported in other African series (15-20%) [15,22,24,25,27], but remains higher than the rates typically observed in high-income countries (5-8%) [41]. This discrepancy reflects contextual challenges inherent to low-resource environments, including delayed presentation, fragile bone quality, higher infection risk, and limited access to specialized rehabilitation services.
Dislocations (6.6 %)
Our dislocation rate was lower than those reported by Soulama et al. in Mali (12.1%) [27] and Ibrahim et al. in Cameroun (14.7 %) [25], suggesting that standardization of surgical technique and structured postoperative protocols may have contributed to improved stability. First-episode dislocations were successfully managed with closed reduction, while recurrent cases required revision surgery. The selective use of dual-mobility components in revision or high-risk patients illustrates progressive adaptation to complex cases, consistent with current evidence supporting dual-mobility implants as an effective strategy to reduce instability, particularly in resource-constrained settings and high-risk populations [42,43].
Infections (6.6%)
Postoperative infections were predominantly observed in immunocompromised patients, including those with HIV infection or diabetes mellitus. Although slightly lower than the African average (~10%), this rate remained higher than those reported in high-income countries (0.4–1.5%) [41]. These findings highlight ongoing contextual barriers, such as limited microbiology laboratory capacity, constraints in sterilization systems, and challenges in implementing comprehensive infection-prevention bundles. Our infection protocol relied on reinforced perioperative measures, including preoperative skin preparation, povidone-iodine cleansing, double gloving, sterile disposable drapes, and targeted antibiotic prophylaxis. Early infections were managed with irrigation and debridement combined with pathogen-directed systemic antibiotics, in line with accepted treatment algorithms.
Periprosthetic fractures (3.3%)
These complications occurred following postoperative trauma and were managed through osteosynthesis and/or revision arthroplasty, in accordance with current recommendations [44]. This rate is consistent with other reports from sub-Saharan Africa, where periprosthetic fractures are often linked to poor bone quality, limited access to physiotherapy, and high early postoperative mobility demands.
Aseptic loosening (3.3%)
Both early and late aseptic loosening were observed, including in a 21-year-old patient with sickle-cell disease. This reinforces the well-documented structural bone fragility and compromised vascularity associated with hemoglobinopathies, which predispose to early implant failure in this subgroup [32]. When interpreted through Delaunay’s classification [45], these failures were predominantly related to pre-existing bone deficits and technical constraints, factors frequently reported in African and international studies involving young patients with osteonecrosis.
Thromboembolic events (1.6%)
One case of pulmonary embolism occurred despite adequate pharmacologic prophylaxis, reaffirming that venous thromboembolism risk persists even under optimal preventive strategies [46]. This finding underscores the need for context-adapted thromboprophylaxis protocols, particularly in patients with limited mobility, comorbidities, or delays in rehabilitation [47].
Functional outcomes and clinical relevance
Functional recovery after total hip arthroplasty was remarkable. The Merle d’Aubigné–Postel score improved from a preoperative mean of 6.4 to 16.2 at six months, reflecting marked pain relief, restoration of mobility, and improved gait. The PMA score was chosen for its simplicity, reproducibility, and long-standing validation in francophone orthopedic practice, particularly within African settings where patient-reported outcome measures such as WOMAC (Western Ontario and McMaster Universities Osteoarthritis Index) [48] or HOOS (Hip disability and Osteoarthritis Outcome Score) [49] are not yet culturally adapted.
The minimal clinically important difference (MCID) [50] for the PMA total score, estimated at approximately 2 points, was exceeded in more than 90% of patients, indicating that the improvement observed was not only statistically significant but also clinically relevant.
Referral bias and case complexity
The predominance of osteonecrosis and sickle-cell disease mirrors the regional epidemiologic profile, contrasting with Western cohorts dominated by primary osteoarthritis. As a tertiary referral center, Medpark manages advanced and technically demanding cases, explaining the higher baseline risk of complications and the limited external comparability of outcomes.
Strengths, Limitations, and Future Perspectives
This study provides valuable mid-term outcome data on THA in the DRC, where evidence remains scarce. Strengths include a relatively homogeneous cohort, mainly young patients with advanced osteonecrosis, managed with a standardized surgical technique, a coordinated multidisciplinary approach, and a follow-up exceeding four years, allowing reliable evaluation of clinical outcomes and complications in a low-resource setting. However, its single-center urban design limits generalizability to other regions, particularly rural areas with fewer resources. Intermittent implant supply, despite the partnership model, occasionally affected standardization of fixation and bearing choices. Limited microbiology capacity also constrained optimal infection management. Future development of THA services in the DRC should prioritize the creation of a national arthroplasty registry, strengthening of specialized training, improved rehabilitation and microbiology services, and innovative financing models to reduce patient costs. Expanding pooled procurement systems and regional partnerships could further enhance affordability and equitable access to joint replacement across the country [51,52].
Our experience highlights not only the feasibility of THA in Lubumbashi but also the specific challenges of practicing in a resource-limited environment. By implementing cost-reduction measures, strict infection control, adaptive implant strategies, and strong institutional partnerships, we were able to achieve functional outcomes comparable to regional series. These lessons may guide other low-resource centers in sub-Saharan Africa seeking to establish or expand arthroplasty programs.
Total hip arthroplasty is feasible and yields encouraging functional outcomes in resource-limited African settings, provided that careful planning and adapted protocols are implemented.
References
- 1. Zhu X, Zeng Y. [2024 American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guideline: Management of Osteoarthritis of the Hip (summary) interpretation]. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2025 Oct 15;39(10):1325-1332. Chinese. doi: 10.7507/1002-1892.202507104. PMID: 41093799; PMCID: PMC12528243. [Google Scholar] [PubMed] [CrossRef]
- 2. Hannon CP, Goodman SM, Austin MS, and al. 2023 American College of Rheumatology and American Association of Hip and Knee Surgeons Clinical Practice Guideline for the Optimal Timing of Elective Hip or Knee Arthroplasty for Patients With Symptomatic Moderate-to-Severe Osteoarthritis or Advanced Symptomatic Osteonecrosis With Secondary Arthritis for Whom Nonoperative Therapy Is Ineffective. Arthritis Care Res (Hoboken). 2023 Nov;75(11):2227-2238. doi: 10.1002/acr.25175. Epub 2023 Sep 25. PMID: 37743767. [Google Scholar] [PubMed] [CrossRef]
- 3. Kazley J, Bagchi K. Femoral Neck Fractures. [Updated 2023 May 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537347. [Google Scholar] [PubMed]
- 4. George G, Lane JM. Osteonecrosis of the Femoral Head. J Am Acad Orthop Surg Glob Res Rev. 2022 May 1;6(5):e21.00176. doi: 10.5435/JAAOSGlobal-D-21-00176. PMID: 35511598; PMCID: PMC9076447. [Google Scholar] [PubMed] [CrossRef]
- 5. Backes J, Pabinger C, Lothaller H, Geissler A. Utilization rates of hip arthroplasty in OECD countries revised. Osteoarthritis Cartilage. 2025 Sep 19:S1063-4584(25)01160-4. doi: 10.1016/j.joca.2025.09.012. Epub ahead of print. PMID: 40976362. [Google Scholar] [PubMed] [CrossRef]
- 6. Davies PS, Graham SM, Maqungo S, Harrison WJ. Total joint replacement in sub-Saharan Africa: a systematic review. Trop Doct. 2019 Apr;49(2):120-128. doi: 10.1177/0049475518822239. Epub 2019 Jan 12. PMID: 30636518; PMCID: PMC6535807. [Google Scholar] [PubMed] [CrossRef]
- 7. Graham SM, Howard N, Moffat C, Lubega N, Mkandawire N, Harrison WJ. Total Hip Arthroplasty in a Low-Income Country: Ten-Year Outcomes from the National Joint Registry of the Malawi Orthopaedic Association. JB JS Open Access. 2019 Dec 5;4(4):e0027. doi: 10.2106/JBJS.OA.19.00027. PMID: 32043050; PMCID: PMC6959913. [Google Scholar] [PubMed] [CrossRef]
- 8. Mambu Vangu A, Kambu MN, Mfundu Mbuangi J, Leather AJM, Tissingh EH. Health systems strengthening in the Democratic Republic of Congo: the importance of surgical data. BMJ Glob Health. 2025 Sep 4;10(9):e017759. doi: 10.1136/bmjgh-2024-017759. PMID: 40908031; PMCID: PMC12414223. [Google Scholar] [PubMed] [CrossRef]
- 9. https://files.acquia.undp.org/public/migration/cd/UNDP-CD-Profil-PROVINCE-Katanga.pdf. [Google Scholar] [PubMed]
- 10. Merle d’Aubigné R, Postel M. Functional results of hip arthroplasty with acrylic prosthesis. J Bone Joint Surg [Br]. 1954;36-B(3):451-475. [Google Scholar] [PubMed]
- 11. Ficat R. P. Idiopathic bone necrosis of the femoral head: early diagnosis and treatment. The Journal of Bone and Joint Surgery – British Volume, 1985; 67(1): 3–9. https://doi.org/10.1302/0301-620x.67b1.3155745. [Google Scholar] [PubMed] [CrossRef]
- 12. Parvizi J, Gehrke T, Chen AF. Proceedings of the International Consensus Meeting on Periprosthetic Joint Infection. J Arthroplasty. 2018;33(10):2992-2997. doi: 10.1016/j.arth.2018.09.015. [Google Scholar] [PubMed] [CrossRef]
- 13. DeLee JG, Charnley J. Radiological demarcation of cemented sockets in total hip replacement. Clin Orthop Relat Res. 1976;(121):20–32. [Google Scholar] [PubMed]
- 14. Gruen TA, McNeice GM, Amstutz HC. “Modes of failure” of cemented stem-type femoral components: a radiographic analysis of loosening. Clin Orthop Relat Res. 1979;(141):17–27. [Google Scholar] [PubMed]
- 15. Barro V, Carbonell-Rosell C, Ribera J, Villalonga A, Martin-Domínguez L, Soza D, Plomer M, Aguilar M, Sevil R, José Echarri J. [Translated article] Challenges in implementing a total hip arthroplasty program in a developing country: Our experience at Monkole Hospital in the Democratic Republic of Congo. Rev Esp Cir Ortop Traumatol. 2025 Feb 14:S1888-4415(25)00034-7. English, Spanish. doi: 10.1016/j.recot.2025.02.005. Epub ahead of print. PMID: 39956360. [Google Scholar] [PubMed] [CrossRef]
- 16. Ciza Musimwa P, Kaguku Nfundiko A, Kitumaini Munyahali J, Tubura Valery A, Zihindula Buhendwa F, Berg U.Total hip arthroplasty in a resource-limited setting: retrospective analysis of a series of ten cases at Panzi Hospital, Bukavu, Democratic Republic of the Congo. Kivu Medical Journal. 2025;3(2):1–5. doi:10.64263/kmj.v3i2.69. [Google Scholar] [PubMed] [CrossRef]
- 17. Ndayizeye G, Niyondiko JC, Manirakiza S, Baramburiye CP, Carter C. Treatment of Fracture Dislocation of the Femoral Head in a Resource Limited Country (Burundi). Open Journal of Orthopedics. 2020 Dec 18;10(12):384–94. [Google Scholar] [PubMed]
- 18. Monka M, Omboumahou Bakale FE, Ngatse-Oko A, Bilongo-Bouyou A, Moyikoua A. [Google Scholar] [PubMed]
- 19. Cervicocephalic arthroplasty for femoral neck fracture in Brazzaville: anatomical and functional outcomes at 28-month follow-up. African Journal of Orthopaedics and Trauma. 2016;1(1):36–40. [Google Scholar] [PubMed]
- 20. Erivan R, Villatte G, Dartus J, Reina N, Descamps S, Boisgard S. Progression and projection for hip surgery in France, 2008-2070: Epidemiologic study with trend and projection analysis. Orthop Traumatol Surg Res. 2019 Nov;105(7):1227-1235. doi: 10.1016/j.otsr.2019.07.021. Epub 2019 Oct 9. PMID: 31606338. [Google Scholar] [PubMed] [CrossRef]
- 21. Lenguerrand E, Ben-Shlomo Y, Rangan A, Beswick A, Whitehouse MR, Deere K, Sayers A, Blom AW, Judge A. Inequalities in provision of hip and knee replacement surgery for osteoarthritis by age, sex, and social deprivation in England between 2007-2017: A population-based cohort study of the National Joint Registry. PLoS Med. 2023 Apr 27;20(4):e1004210. doi: 10.1371/journal.pmed.1004210. PMID: 37104268; PMCID: PMC10138460. [Google Scholar] [PubMed] [CrossRef]
- 22. Matharu GS, Culliford DJ, Blom AW, Judge A. Projections for primary hip and knee replacement surgery up to the year 2060: an analysis based on data from The National Joint Registry for England, Wales, Northern Ireland and the Isle of Man. Ann R Coll Surg Engl. 2022 Jun;104(6):443-448. doi: 10.1308/rcsann.2021.0206. Epub 2021 Dec 23. PMID: 34939832; PMCID: PMC9157920. [Google Scholar] [PubMed] [CrossRef]
- 23. Lubega N., Mkandawire N. C., Sibande G. C., et al. Joint replacement in Malawi: establishment of a National Joint Registry. The Journal of Bone and Joint Surgery – British Volume, 2009; 91(3): 341–343. https://doi.org/10.1302/0301-620x.91b3.21706. [Google Scholar] [PubMed] [CrossRef]
- 24. George A, Ofori-Atta P. Joint replacement surgery in Ghana (West Africa)-an observational study. Int Orthop. 2019 May;43(5):1041-1047. doi: 10.1007/s00264-019-04286-1. Epub 2019 Jan 24. PMID: 30680518; PMCID: PMC6470119. [Google Scholar] [PubMed] [CrossRef]
- 25. Essomba R, Mondji S, Mbonda AN, Tochie JN, Abogo S, Lekina F, Nonga BN. An 8-year audit of the clinical profile, surgical indications and therapeutic outcomes of total hip arthroplasty in a sub-Saharan Africa setting: a retrospective cohort study. J Xiangya Med 2022;7:6. [Google Scholar] [PubMed]
- 26. Ibrahima F, Fokam P, Ngongang F-O, et al. Preliminary results of total hip arthroplasties performed in a low-resource African country. Orthopaedics & Traumatologic Surgery Review. 2014;100(3):264-268. doi:10.1016/j.rcot.2014.02.017. [Google Scholar] [PubMed] [CrossRef]
- 27. Kaboré F, Sougué C, Zongo Y, Sompougoudou C, Tiendrébéogo B, Zabsonré-Tiendrébéogo W, et al. Diagnostic and therapeutic aspects of hip osteoarthritis in a hospital setting in Ouagadougou (Burkina Faso). African Francophone Rheumatology. 2022 Oct 9;2(2):10-14. Available from: https://www.rhumatoafrique.org/index.php/raf/article/view/20. [Google Scholar] [PubMed]
- 28. Soulama M, Diallo M, Kangoyé R, Tankoano AI, Ouédraogo S, Sidibé A, Dakouré PW. Total hip replacements in a country with limited resources: evaluation of medium-term results. Mali Med. 2021;36(4):23-27. PMID: 38200719. [Google Scholar] [PubMed]
- 29. Diaby H, Total hip arthroplasty: short-term epidemiological, clinical, and therapeutic outcomes (thesis). Bamako, Mali: University Teaching Hospital of Mali (CHU of Mali); 2023. [Google Scholar] [PubMed]
- 30. Ayouba G, Kombate N, Bakriga B, Dellanh Y, Towoezim T, Walla A, Abalo A. Clinical, therapeutic and outcome characteristics of patients operated on with dual-mobility total hip arthroplasty in Togo: a multicenter study of 147 cases. Health Sciences and Disease. 2021;22(11). doi:10.5281/hsd.v22i11.3097. [Google Scholar] [PubMed] [CrossRef]
- 31. Kalifa C., Sanogo C. O., Coulibaly M., et al. Anatomical and functional outcomes of total hip arthroplasties at Kati University Hospital. Mali Médical, 2023 ; 38(1). ISSN 0464-7874. [Google Scholar] [PubMed]
- 32. Bombah F, Nguiabanda L, Diawara M-G E, Mikiela A. Total hip arthroplasty: epidemiology, surgical technique, and seven-year results of practice in Libreville. Health Sciences and Disease. 2023;24(2). doi:10.5281/hsd.v24i2.4187. [Google Scholar] [PubMed] [CrossRef]
- 33. Trop Med. Total hip arthroplasty for aseptic osteonecrosis in sickle-cell disease in Senegal: a series of 48 hip prostheses. Médecine Tropicale. 2009;69(6):573-576. [Google Scholar] [PubMed]
- 34. Erivan R, Villatte G, Dartus J, Reina N, Descamps S, Boisgard S. Evolution and projection of hip surgery in France from 2008 to 2070: an epidemiological study with trend analysis and projection. Orthopaedics & Traumatologic Surgery Review. 2019;105(7):803-812. doi:10.1016/j.otsr.2019.07.021. [Google Scholar] [PubMed] [CrossRef]
- 35. Evans JT, Evans JP, Walker RW, Blom AW, Whitehouse MR, Sayers A. How long does a hip replacement last? A systematic review and meta-analysis of case series and national registry reports with more than 15 years of follow-up. Lancet. 2019 Feb 16;393(10172):647-654. doi: 10.1016/S0140-6736(18)31665-9. Epub 2019 Feb 14. PMID: 30782340; PMCID: PMC6376618. [Google Scholar] [PubMed] [CrossRef]
- 36. Jasvinder A. Singh, Shaohua Yu, Lang Chen and John D. Cleveland, Rates of Total Joint Replacement in the United States: Future Projections to 2020–2040 Using the National Inpatient Sample, The Journal of Rheumatology April 2019, jrheum.170990; DOI: https://doi.org/10.3899/jrheum.170990. [Google Scholar] [PubMed] [CrossRef]
- 37. Naseer ZA, Bachabi M, Jones LC, Sterling RS, Khanuja HS. Osteonecrosis in Sickle Cell Disease. South Med J. 2016 Sep;109(9):525-30. doi: 10.14423/SMJ.0000000000000516. PMID: 27598354. [Google Scholar] [PubMed] [CrossRef]
- 38. Almarzooq O, Alhassan M, Alansari L, Alanazi T, Madan FH. Cemented Versus Uncemented Total Hip Arthroplasty in Sickle Cell Disease Patients: A Retrospective Study. Cureus. 2023 Mar 14;15(3):e36138. doi: 10.7759/cureus.36138. PMID: 37065305; PMCID: PMC10101182. [Google Scholar] [PubMed] [CrossRef]
- 39. Ahmed A. Khalifa, Mohamed A. Mahran2 , Ahmed M. Abdelaal2, Economic solutions for primary and total hip arthroplasty revision from the egyptian experience. Revista Cubana de Ortopedia y Traumatología. 2024;38:e790. [Google Scholar] [PubMed]
- 40. Urban JA, Garvin KL, Boese CK, Bryson L, Pedersen DR, Callaghan JJ, Miller RK. Ceramic-on-polyethylene bearing surfaces in total hip arthroplasty. Seventeen to twenty-one-year results. J Bone Joint Surg Am. 2001 Nov;83(11):1688-94. doi: 10.2106/00004623-200111000-00011. PMID: 11701792. [Google Scholar] [PubMed] [CrossRef]
- 41. Cao Y, Tang P, Chai H, Ma W, Lin B, Zhu Y, Abdirahman A, Xiao W, Zhang J, Li Y, Liu S, Wen T. The application of antibiotic-loaded bone cement in preventing periprosthetic joint infection: an umbrella review. J Orthop Traumatol. 2025 Apr 18;26(1):23. doi: 10.1186/s10195-025-00839-w. PMID: 40249535; PMCID: PMC12008095. [Google Scholar] [PubMed] [CrossRef]
- 42. Fontalis A, Berry DJ, Shimmin A, Slullitel PA, Buttaro MA, Li C, Malchau H, Haddad FS. Prevention of early complications following total hip replacement. SICOT J. 2021;7:61. doi: 10.1051/sicotj/2021060. Epub 2021 Nov 30. PMID: 34851264; PMCID: PMC8634898. [Google Scholar] [PubMed] [CrossRef]
- 43. Hernigou P, Auregan JC, Potage D, Roubineau F, Flouzat Lachaniette CH, Dubory A. Dual-mobility implants prevent hip dislocation following hip revision in obese patients. Int Orthop. 2017 Mar;41(3):469-473. doi: 10.1007/s00264-016-3316-y. Epub 2016 Oct 20. PMID: 27761631. [Google Scholar] [PubMed] [CrossRef]
- 44. Patil N, Deshmane P, Deshmukh A, Mow C. Dual Mobility in Total Hip Arthroplasty: Biomechanics, Indications and Complications-Current Concepts. Indian J Orthop. 2021 Oct 13;55(5):1202-1207. doi: 10.1007/s43465-021-00471-w. PMID: 34824721; PMCID: PMC8586128. [Google Scholar] [PubMed] [CrossRef]
- 45. Ricci WM. Periprosthetic femur fractures. J Orthop Trauma. 2015 Mar;29(3):130-7. doi: 10.1097/BOT.0000000000000282. PMID: 25699540. [Google Scholar] [PubMed] [CrossRef]
- 46. Delaunay, C., Cazeau, C., Et Kapandji, A. I. Cementless primary total hip replacement. International Orthopaedics, 1998, vol. 22, no 1, p. 1-5. [Google Scholar] [PubMed]
- 47. Almegren MO, Alhedaithy AA, Alomri AS, Albawardy NF, Mesmar RS, Al Qahtani MA. Venous thromboembolism after total knee and hip arthroplasty. A retrospective study. Saudi Med J. 2018 Nov;39(11):1096-1101. doi: 10.15537/smj.2018.11.23545. PMID: 30397708; PMCID: PMC6274659. [Google Scholar] [PubMed] [CrossRef]
- 48. Eikelboom JW, Quinlan DJ, Douketis JD. Extended-duration prophylaxis against venous thromboembolism after total hip or knee replacement: a meta-analysis of the randomised trials. Lancet. 2001 Jul 7;358(9275):9-15. doi: 10.1016/S0140-6736(00)05249-1. PMID: 11454370. [Google Scholar] [PubMed] [CrossRef]
- 49. Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol. 1988 Dec;15(12):1833-40. PMID: 3068365. [Google Scholar] [PubMed]
- 50. Nilsdotter AK, Lohmander LS, Klässbo M, Roos EM. Hip disability and osteoarthritis outcome score (HOOS)–validity and responsiveness in total hip replacement. BMC Musculoskelet Disord. 2003 May 30;4:10. doi: 10.1186/1471-2474-4-10. Epub 2003 May 30. PMID: 12777182; PMCID: PMC161815. [Google Scholar] [PubMed] [CrossRef]
- 51. Solomito MJ, Carangelo R, Makanji H. The Minimal Clinically Important Difference (MCID) for Total Joint Arthroplasty Outcome Measures Varies Substantially by Calculation Method. J Bone Joint Surg Am. 2025 May 7;107(9):994-999. doi: 10.2106/JBJS.24.00916. Epub 2025 Mar 20. PMID: 40112037. [Google Scholar] [PubMed] [CrossRef]
- 52. Dworkin M, Woolley PM, Shahab F, Noe MC, Barry R, Chomba D, et al. Access to Orthopaedic Devices in Low and Middle-Income Countries: Challenges and Opportunities. The Journal of Bone and Joint Surgery 107(10):p 1154-1160, May 21, 2025. | DOI: 10.2106/JBJS.24.00997. [Google Scholar] [PubMed] [CrossRef]
- 53. Pedneault C, St George S, Masri BA. Challenges to Implementing Total Joint Replacement Programs in Developing Countries. Orthop Clin North Am. 2020 Apr;51(2):131-139. doi: 10.1016/j.ocl.2019.11.001. Epub 2020 Jan 16. PMID: 32138851. [Google Scholar] [PubMed] [CrossRef]






Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Day-Care Direct Anterior Total Hip Arthroplasty in Urban India: Patient Education, Apprehensions, and Outcomes
March 1, 2026 Day-Care Direct Anterior Total Hip Arthroplasty in Urban India: Patient Education, Apprehensions, and Outcomes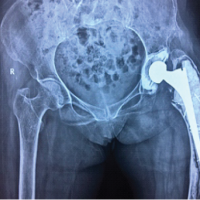 February 1, 2025 Complex Revisions in Total Hip Arthroplasty Amidst COVID-19 Delays: A Case Report
February 1, 2025 Complex Revisions in Total Hip Arthroplasty Amidst COVID-19 Delays: A Case Report March 1, 2026 Managing Hip Arthritis in an Above-Knee Amputee: A Case Report of Total Hip Arthroplasty with Surgical Technique and Rehabilitation Considerations
March 1, 2026 Managing Hip Arthritis in an Above-Knee Amputee: A Case Report of Total Hip Arthroplasty with Surgical Technique and Rehabilitation Considerations March 1, 2026 Evaluation of Spine Hip Relation and its Correlation as a Guide to Total Hip Arthroplasty
March 1, 2026 Evaluation of Spine Hip Relation and its Correlation as a Guide to Total Hip Arthroplasty