
External Snapping Hip Syndrome caused by a tight iliotibial band or gluteus maximus tendon can persist despite conservative treatment. Open Z-plasty lengthening of the iliotibial band is a safe and effective surgical option for refractory cases, offering reliable symptom relief.
Dr. Pradeep Patel, Department of Orthopedics, Shree Narayana Hospital, Raipur - 492 001, Chhattisgarh, India. E-mail: drpradeep1903@gmail.com
Introduction: Snapping hip syndrome (SHS), particularly its external type, is a condition in which a tight iliotibial band (ITB) or gluteus maximus (G.Max) tendon mechanically “snaps” over the greater trochanter during dynamic hip movements. While often managed conservatively, persistent and painful cases may require surgical intervention. This report presents a case of refractory external SHS in a young female patient treated successfully using an open Z-plasty lengthening of the ITB.
Case Report: A 24-year-old physically active female presented with a 6-month history of audible snapping in the left hip, accompanied by pain for the preceding month. Examination revealed a positive Ober’s test and reproducible snapping with hip flexion. Conservative measures failed. An open Z-plasty release of the ITB and partial G.Max release was performed, resulting in complete resolution of symptoms.
Conclusion: Open Z-plasty is a safe and effective treatment for external SHS unresponsive to conservative management, offering direct visualization and reliable symptom relief.
Keywords: Snapping hip syndrome, iliotibial band, Z-plasty, gluteus maximus release, external coxa saltans.
Snapping hip syndrome (SHS), or coxa saltans, is characterized by an audible, palpable, or visible snapping sensation around the hip joint during specific movements. It is categorized into external, internal, and intra-articular types, each associated with distinct anatomical causes [1,2]. The external type, the most common among active young individuals, is due to the iliotibial band (ITB) or the anterior edge of the gluteus maximus (G.Max) tendon snapping over the greater trochanter (GT) [3]. The pathophysiology involves repetitive friction between a tight ITB and the bony prominence of the GT, particularly during activities involving flexion, extension, or abduction of the hip. Over time, this friction can lead to thickening of the fascia and increased mechanical resistance, making snapping audible or visible and sometimes painful [4]. External SHS may be exacerbated by increased physical activity, anatomic predisposition, or biomechanical abnormalities, such as ITB contracture, leg-length discrepancy, or muscle imbalance [1]. The diagnosis is primarily clinical and often supplemented with imaging to exclude intra-articular pathology. Conservative management includes physical therapy focusing on ITB stretching, non-steroidal anti-inflammatory drugs (NSAIDs), and activity modification. Surgical intervention is considered when symptoms persist despite non-operative management. [1,3]. Various surgical strategies exist, ranging from endoscopic ITB release to open procedures, such as Z-plasty or N-plasty [5,6,7]. Open Z-plasty of the fascia lata, as described by Brignall and Stainsby [8], remains a reliable option, particularly in patients with marked contracture or limited access to arthroscopic techniques.
A 24-year-old female presented to the outpatient orthopedic clinic with a 6-month history of a repetitive, audible snapping sensation in her left hip, which had become troublesome (although painless) over the past month. She was physically active and reported difficulty in activities, such as jumping, sitting cross-legged, entering and exiting vehicles, and jogging. She denied any antecedent trauma or overuse injury. The symptoms were localized to the lateral aspect of the hip, without associated numbness, tingling, or systemic signs.
Clinical examination
Active and passive hip range of motion was full and pain-free, except for the presence of a snapping sound during flexion and extension. Visible and palpable snapping was reproducible with passive adduction followed by flexion to 90° and extension. The patient could voluntarily reproduce the snap during standing hip adduction with circumduction.
Ober’s test was positive, indicating tightness of the ITB. Manual muscle testing was within normal limits. No tenderness was noted along the GT or hip joint. Gait analysis revealed no abnormalities. Neurovascular examination of both lower limbs was intact. Radiographs of the pelvis and lateral hip revealed no osseous abnormalities or structural lesions. Based on the clinical findings, a diagnosis of external SHS secondary to ITB tightness was made. Non-operative treatment, including NSAIDs and ITB stretching, failed to alleviate symptoms over 3 months. Given persistent snapping and pain affecting function, surgical intervention was planned.
Surgical technique
Under spinal anesthesia, the patient was positioned lateral on the operating table to aid exposure. The hip was draped and prepared in a sterile fashion. All the landmarks and structures were marked centering GT (Fig 1a). A longitudinal skin incision approximately 8–10 cm in length was made over the posterolateral aspect of the GT, starting just above the trochanteric prominence and extending proximally along the line of the ITB.

Figure 1: (a) Demonstrating surface markings of patient: GT: Greater trochanter, G.Max: Gluteus maximus, FL: Fascia lata, STP: Superior trochanteric portal, and ITP: Inferior trochanteric portal (used for endoscopic release). (b) IT band exposed, marked structure representing thickened band over GT, (c) marking of planned Z-shaped incision.
Upon dissection through the subcutaneous tissues, the ITB was exposed (Fig. 1b). A curved osteotome can be used to clear the fatty tissue gently over ITB. Z-shaped incision is marked, and a longitudinal incision was made through the thickened fascia lata approximately 1–1.5 cm anterior to the tightest palpable portion of the band. This incision served as the central limb of the planned Z-plasty. Two additional transverse limbs were created. The proximal limb was directed anteriorly and distally. The distal limb was directed posteriorly and proximally, forming a classic Z-pattern (Fig. 1c). The flaps created were carefully mobilized to allow lengthening of the contracted fascia (Fig. 2a and b). Upon elevation of flap trochanteric bursa is visualized and thickened part is excised (Fig. 2c). Thickened fascia was trimmed a bit and care was taken not to injure the underlying vastus lateralis (Fig. 3a). Fibers of G.Max were also found tight so partial release of the G.Max tendon also performed (Fig. 3b). The transposed flaps were aligned in a lengthened configuration (Fig. 4b), ensuring adequate release of the tight ITB, and were then secured with polyglactin (Vicryl no 1) absorbable sutures to maintain the corrected position (Fig. 4b). The Z-plasty allowed an approximate 2–3 cm lengthening of the tight fascia. Hemostasis was ensured, and a closed suction drain was placed. Layered wound closure was performed, and a sterile dressing was applied.

Figure 2: (a) Raising the proximal pointing flap anteriorly, (b) raising the distal pointing flap posteriorly, (c) demonstrating thickened bursa excision.

Figure 3: (a) Trimming (thining) of thickened fascia over the greater trochanter, (b) partial release of the gluteus maximus tendon.

Figure 4: (a) Demonstrating Z-shaped release, (b) position of flaps after transposition to achieve iliotibial band (ITB) lengthening, (c) ITB post-closure.
Post-operative protocol
The hip was kept in abduction with minimal movement for 10 days. The drain was removed after 48 h. At 2 weeks, the patient began partial weight-bearing with a wide-based crutch-assisted gait. Full weight-bearing was resumed at 6 weeks. Strengthening and flexibility exercises for the hip abductors and ITB were initiated thereafter.
Outcome
At the 2-month follow-up, the patient reported complete resolution of pain and snapping. She regained full range of motion and had returned to her routine physical activities, including recreational running, without restrictions. At 6 months, she remained asymptomatic, with no recurrence of snapping or hip instability.
External SHS is most commonly caused by tight or thickened components of the ITB or anterior G.Max tendon snapping over the GT [1,2]. While often benign, it can become symptomatic, especially in active individuals or athletes, where the repetitive movement increases tension and frictional forces across the GT region. Conservative measures are first-line and include stretching of the ITB and hip external rotators, gait retraining, core strengthening, and anti-inflammatory therapy [9]. Persistent symptoms for >3 months, mechanical dysfunction, or failed therapy warrant surgical treatment. Multiple surgical techniques have been described for ITB release. Endoscopic ITB release is gaining popularity due to its minimally invasive nature, with lower soft tissue trauma and faster recovery [5]. However, these techniques require specialized equipment and expertise, and outcomes may vary. Moreover, recurrence has been documented in a subset of patients, sometimes requiring revision surgery. N-plasty and fan-like releases have been developed as modifications, aiming to provide controlled lengthening and reduce recurrence rates [6,7]. Despite these innovations, the open Z-plasty technique, as originally described by Brignall and Stainsby, remains a highly effective, reproducible, and accessible method, especially in resource-limited settings. The Z-plasty allows controlled lengthening of the fascia, reducing mechanical tension and eliminating the snapping phenomenon. Direct visualization ensures that the tightest fibers are effectively released. This technique is less technically demanding and rewarding [8,10]. In our case, the patient had excellent functional recovery with complete symptom resolution and no complications. This reinforces that, when executed meticulously, open Z-plasty provides predictable outcomes with low risk of recurrence.
This case highlights that open Z-plasty remains a safe, effective, and durable surgical option for external SHS unresponsive to conservative management. While endoscopic and minimally invasive techniques are evolving, traditional open methods should not be overlooked, especially in scenarios where simplicity, cost-effectiveness, and direct control are valued.
Open Z-plasty of the ITB is a safe, effective, and reproducible surgical option for refractory external SHS. It offers direct anatomical correction, especially in cases where conservative therapy fails, and should be considered in young, active patients with persistent symptoms.
References
- 1. Musick SR, Varacallo MA. Snapping Hip syndrome. 2023 Aug 4. In: StatPearls.J Treasure Island, (FL): StatPearls Publishing; 2025 Jan-. PMID: 28846235. [Google Scholar] [PubMed]
- 2. Walker P, Ellis E, Scofield J, Kongchum T, Sherman WF, Kaye AD. Snapping hip syndrome: A comprehensive update. Anesth Pain Med 2021;13:130-8. [Google Scholar] [PubMed]
- 3. Ilizaliturri VM Jr., Martinez-Escalante FA, Chaidez PA, Camacho-Galindo J. Endoscopic iliotibial band release for external snapping hip syndrome. Arthroscopy 2006;22:505-10. [Google Scholar] [PubMed]
- 4. Brignall CG, Stainsby GD. The snapping hip. Treatment by Z-plasty. J Bone Joint Surg Br 1991;73:253-4. [Google Scholar] [PubMed]
- 5. Mange TR, Pasko KB, Wang D. Endoscopic treatment of external coxa saltans (snapping hip) in the supine position. Arthrosc Tech 2021;10:e359-64. [Google Scholar] [PubMed]
- 6. Mak CY, Lui TH. Endoscopic treatment of recurred external snapping hip after iliotibial band release. Arthrosc Tech 2018;7:e267-72. [Google Scholar] [PubMed]
- 7. Park JS, Kim WJ, Lee DW, Soh JW, Won SH, Lee SW, et al. External snapping hip treated by effective designed N-plasty of the iliotibial band. Clin Orthop Surg 2014;6:173-7. [Google Scholar] [PubMed]
- 8. Randelli F. Surgical interventions for external snapping hip syndrome. Knee Surg Sports Traumatol Arthrosc 2013;21:1095-6. [Google Scholar] [PubMed]
- 9. Sanchez-Alvarado A, Bokil C, Cassel M, Engel T. Effects of conservative treatment strategies for iliotibial band syndrome on pain and function in runners: A systematic review. Front Sports Act Living 2024;6:1386456. [Google Scholar] [PubMed]
- 10. Provencher MT, Hofmeister EP, Muldoon MP. The surgical treatment of external coxa saltans (the snapping hip) by Z-plasty of the iliotibial band. Am J Sports Med 2004;32:470-6. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2025 Single-stage reconstruction without grafting for neglected flexor pollicis longus tendon laceration in a child – A case report
March 1, 2025 Single-stage reconstruction without grafting for neglected flexor pollicis longus tendon laceration in a child – A case report December 1, 2024 Correlation of Detachment of Proximal Tibia Superficial Medial Collateral Ligament and Medial Meniscus Extrusion with Knee Osteoarthritis
December 1, 2024 Correlation of Detachment of Proximal Tibia Superficial Medial Collateral Ligament and Medial Meniscus Extrusion with Knee Osteoarthritis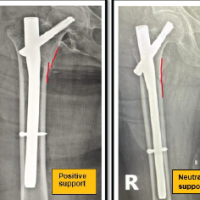 July 1, 2025 Assessing the Importance of Anteromedial Cortical Support in Fixing Pertrochanteric Fractures: A Comprehensive Study
July 1, 2025 Assessing the Importance of Anteromedial Cortical Support in Fixing Pertrochanteric Fractures: A Comprehensive Study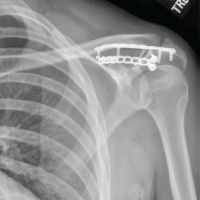 January 1, 2025 Subacromial Distal Clavicle Dislocation with Associated Scapular Spine Fracture: A Case Report
January 1, 2025 Subacromial Distal Clavicle Dislocation with Associated Scapular Spine Fracture: A Case Report