
This case highlights the importance of maintaining a high clinical index of suspicion for necrotizing soft-tissue infections after a human bite, as uncommon anaerobes such as Prevotella intermedia can rapidly progress to life-threatening infections requiring early surgical intervention.
Dr. Marc E Walker, Division of Plastic Surgery, University of Mississippi Medical Center, 2500 North State Street, Jackson - 39216, Mississippi, United States. E-mail: mwalker6@umc.edu
Abstract
Introduction: Human bite wounds account for a small proportion of bite injuries but carry a high risk of infection due to polymicrobial inoculation. While most infections present as cellulitis or abscess, necrotizing soft-tissue infections (NSTIs) are rare and potentially fatal.
Case Report: We present the case of a 72-year-old female who developed an NSTI of the forearm after an occlusal human bite. Despite empiric antibiotics, the infection progressed rapidly, and intraoperative cultures grew Prevotella intermedia, an uncommon anaerobe in NSTIs. She required urgent fasciotomy and debridement, followed by targeted antibiotics and wound closure.
Conclusion: This case underscores the importance of early surgical consultation for suspicious bite wounds and highlights P. intermedia as a potential pathogen in upper extremity NSTIs.
Keywords: Human bite, necrotizing soft-tissue infection, Prevotella intermedia, hand infection, anaerobic bacteria.
Human bite wounds account for approximately 3% of all bite injuries seen in emergency departments and carry a high risk of infection due to the polymicrobial flora of the oral cavity. Infected human bites commonly involve both aerobic and anaerobic bacteria. These injuries are typically classified as either occlusal (biting down) or clenched fist (penetrative) bites. In one study of 50 infected human bites, mixed aerobes and anaerobes were isolated from 54% of wounds, aerobes alone from 44%, and anaerobes alone from 2%. Common isolates include Streptococcus anginosus (52%), Staphylococcus aureus (30%), Eikenella corrodens (30%), Fusobacterium nucleatum (32%), and Prevotella melaninogenica (22%) [1]. While most infections result in cellulitis or abscess formation, severe but rare complications such as septic arthritis, osteomyelitis, and necrotizing soft tissue infections (NSTIs) can occur. NSTIs are life-threatening, with high morbidity and mortality if not recognized early [2,3]. This case highlights an unusual anaerobic organism, Prevotella intermedia, as the causative pathogen in an upper extremity NSTI following a human bite.
A 72-year-old Caucasian female with Alzheimer’s dementia, hypertension, hyperlipidemia, and hypothyroidism developed progressive swelling and erythema of the left forearm after being bitten by her adult son. She was initially treated at an outside hospital with empiric antibiotics, but worsened, prompting transfer. On arrival, she was hemodynamically stable. Laboratory findings revealed leukocytosis (white blood cell count of 13.2 cells/mcL), hypophosphatemia (1.5 mg/dL), and elevated C-reactive protein (34.19 mg/dL). Computed tomography demonstrated extensive subcutaneous gas and fluid extending from the distal humerus to the wrist (3.2 × 10.5 cm), concerning for NSTI (Fig. 1).
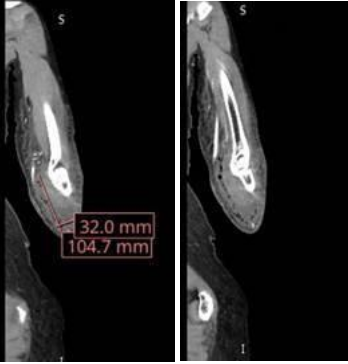
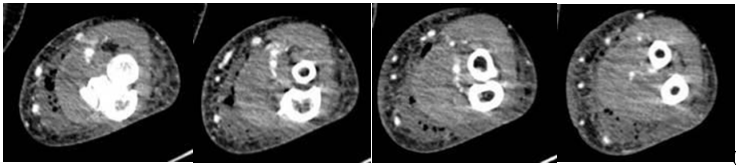
Figure 1: Coronal (a) and axial (b) Computed tomography images of the left forearm demonstrating an extensive subcutaneous fluid collection measuring 3.2 × 10.5 cm and a gas pattern consistent with necrotizing soft-tissue infection. Images progress from proximal to distal.
Plastic surgery was performed at the bedside, with incision and drainage in the emergency room. The patient was admitted for intravenous antibiotic therapy, and formal operative debridement occurred on hospital day 2. A dorsal and volar fasciotomy exposed a large abscess cavity; purulent material was present in subcutaneous tissue, though muscle and fascia appeared viable.
Anaerobic cultures grew P. intermedia. Antibiotics were escalated to daptomycin and piperacillin–tazobactam, then narrowed to amoxicillin–clavulanate and metronidazole once sensitivities were available. Wound care was managed with dressing changes. No further debridement was required, and delirium precautions helped improve her mental status. On hospital day 7, she underwent delayed wound closure and was discharged home on oral therapy in stable condition. A 72-year-old Caucasian female with Alzheimer’s dementia, hypertension, hyperlipidemia, and hypothyroidism developed progressive swelling and erythema of the left forearm after being bitten by her adult son. She was initially treated at an outside hospital with empiric antibiotics, but worsened, prompting transfer. On arrival, she was hemodynamically stable. Laboratory findings revealed leukocytosis (white blood cell count of 13.2 cells/mcL), hypophosphatemia (1.5 mg/dL), and elevated C-reactive protein (34.19 mg/dL). Computed tomography demonstrated extensive subcutaneous gas and fluid extending from the distal humerus to the wrist (3.2 × 10.5 cm), concerning for NSTI (Fig. 1). Plastic surgery was performed at the bedside, with incision and drainage in the emergency room. The patient was admitted for intravenous antibiotic therapy, and formal operative debridement occurred on hospital day 2. A dorsal and volar fasciotomy exposed a large abscess cavity; purulent material was present in subcutaneous tissue, though muscle and fascia appeared viable. Anaerobic cultures grew P. intermedia. Antibiotics were escalated to daptomycin and piperacillin–tazobactam, then narrowed to amoxicillin–clavulanate and metronidazole once sensitivities were available. Wound care was managed with dressing changes. No further debridement was required, and delirium precautions helped improve her mental status. On hospital day 7, she underwent delayed wound closure and was discharged home on oral therapy in stable condition.
NSTIs from human bites are rare but aggressive. Although human bites represent only 3% of bite injuries, they are often underestimated because the external wounds may appear minor [4]. Occlusal bites, such as in this case, can transmit large volumes of oral flora directly into deep tissue planes [5]. The oral cavity contains over 50 bacterial species and approximately 108 organisms per milliliter of saliva [5]. Frequently isolated aerobes include S. anginosus, S. aureus, and E. corrodens, whereas anaerobes such as Prevotella and Fusobacterium dominate the anaerobic spectrum [1,5]. In one prospective study, mixed aerobes and anaerobes were recovered from over half of infected bites, and many strains produced beta-lactamase, conferring resistance to penicillins [1].
- intermedia, typically associated with periodontal disease, is rarely implicated in NSTIs. P. intermedia is part of the normal oral microbiota but can act as an opportunistic pathobiont within dysbiotic biofilms, contributing to inflammatory tissue destruction and invasive infection when host defenses are compromised [6]. It thrives in anaerobic, inflamed environments and exhibits resistance to penicillins, cephalosporins, and tetracyclines [7]. In our case, the isolate was susceptible to metronidazole, ampicillin–sulbactam, piperacillin–tazobactam, and meropenem, consistent with prior reports [7].
The pathogenicity of P. intermedia is linked to biofilm formation and secretion of virulence factors that stimulate pro-inflammatory mediators such as interleukin (IL)-1β, IL-8, and matrix metalloproteinases, accelerating soft-tissue degradation [7,8]. Immunocompromised patients, including elderly or diabetic individuals, may be especially prone to NSTIs following bite wounds [7]. Empiric management should therefore include broad coverage for aerobes, anaerobes, and methicillin-resistant S. aureus. Infectious Diseases Society of America guidelines recommend vancomycin in combination with piperacillin–tazobactam or a carbapenem, with de-escalation based on culture results [9,10]. Early surgical consultation is crucial when features such as pain out of proportion, rapidly advancing erythema, or subcutaneous gas are present [3,5]. Our patient’s favorable outcome underscores the importance of timely multidisciplinary management, including urgent surgical exploration, culture-directed antibiotic therapy, and supportive care. While Prevotella spp. are uncommon causes of NSTI, they should remain on the differential in bite-associated infections.
Human bite wounds can progress rapidly to NSTI. Prompt recognition by both surgical and medical teams, broad-spectrum empiric coverage, and early surgical management are essential. Rare anaerobes such as P. intermedia should be considered in refractory or severe cases.
Human bite wounds can progress rapidly to necrotizing soft-tissue infection despite an initially benign appearance. Early recognition, prompt surgical evaluation, and broad-spectrum antimicrobial coverage are essential to positively impact mortality following NSTIs. Anaerobic oral flora, including Prevotella intermedia, should be considered potential pathogens in bite-associated infections in order to ensure proper coverage with antibiotics.
References
- 1. Talan DA, Abrahamian FM, Moran GJ, Citron DM, Tan JO, Goldstein EJ, et al. Clinical presentation and bacteriologic analysis of infected human bites in patients presenting to emergency departments. Clin Infect Dis 2003;37:1481-9. [Google Scholar] [PubMed]
- 2. Bunzli WF, Wright DH, Hoang AT, Dahms RD, Hass WF, Rotschafer JC. Current management of human bites. Pharmacotherapy 1998;18:227-34. [Google Scholar] [PubMed]
- 3. Sikora CA, Spielman J, Macdonald K, Tyrrell GJ, Embil JM. Necrotizing fasciitis resulting from human bites: A report of two cases of disease caused by group A streptococcus. Can J Infect Dis Med Microbiol. 2005 Jul;16(4):221-4. doi: 10.1155/2005/706238. [Google Scholar] [PubMed] [CrossRef]
- 4. Elkamch H, Mesbahi A, Brahmi A, Hafidi J, Gharib N, Abassi A, et al. Management of necrotizing fasciitis due to a human bite: Case report. Int Surg J 2024;11:1147-51. [Google Scholar] [PubMed]
- 5. Merriam CV, Fernandez HT, Citron DM, Tyrrell KL, Warren YA, Goldstein EJ. Bacteriology of human bite wound infections. Anaerobe 2003;9:83-6. [Google Scholar] [PubMed]
- 6. Könönen E, Fteita D, Gursoy UK, Gursoy M. Prevotella species as oral residents and infectious agents with potential impact on systemic conditions. J Oral Microbiol 2022;14:2079814. [Google Scholar] [PubMed]
- 7. Maniscalco K, Edens MA. Human bites. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/nbk430764, Last Accessed 03/01/2026 [Google Scholar] [PubMed]
- 8. Karched M, Bhardwaj RG, Qudeimat M, Al-Khabbaz A, Ellepola A. Proteomic analysis of the periodontal pathogen Prevotella intermedia secretomes in biofilm and planktonic lifestyles. Sci Rep 2022;12:5636. [Google Scholar] [PubMed]
- 9. Patil PD, Panchabhai TS, Galwankar SC. Managing human bites. J Emerg Trauma Shock 2009;2:186-90. [Google Scholar] [PubMed]
- 10. Brook I. Management of human and animal bite wounds: An overview. Adv Skin Wound Care 2005;18:197-203. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Management of Naja kaouthia Envenomation at a Quaternary Urban Medical Center: A Case Report
May 1, 2026 Management of Naja kaouthia Envenomation at a Quaternary Urban Medical Center: A Case Report February 1, 2026 National Demographic and Treatment Patterns of Finger Cellulitis, Paronychias, and Felons
February 1, 2026 National Demographic and Treatment Patterns of Finger Cellulitis, Paronychias, and Felons October 1, 2025 Exclusion of Necrotizing Soft-tissue Infection in a Patient with Malpositioned Intraosseous Access: A Case Report
October 1, 2025 Exclusion of Necrotizing Soft-tissue Infection in a Patient with Malpositioned Intraosseous Access: A Case Report June 1, 2025 Necrotizing Fasciitis Caused by Gas-producing Methicillin-sensitive Staphylococcus aureus: A Case Report
June 1, 2025 Necrotizing Fasciitis Caused by Gas-producing Methicillin-sensitive Staphylococcus aureus: A Case Report