
Delayed recognition of a bucket-handle labral tear in the presence of a Fleck sign may result in ir-reversible changes; early detection remains crucial.
Dr. Mattia Blancato, Department of Orthopaedic Surgeon, Ales-sandro Manzoni Hospital, Piazza Cardinal Ferrari 1, 20122 Milan, Lecco, Italy. E-mail: mattia.blancato@unimi.it
Abstract
Introduction: Bucket-handle tears of the acetabular labrum are rare injuries, especially in pediat-ric patients. Typically resulting from high-energy trauma, they are often challenging to diagnose due to subtle clinical signs and non-specific imaging findings.
Case Report: We report the case of a pediatric patient presenting with progressive hip pain and functional limitation after trauma. Advanced imaging revealed a displaced labral fragment con-sistent with a bucket-handle tear and a Fleck sign on computed tomography, indicating a posterior osteochondral avulsion. Arthroscopic exploration confirmed that the labral tissue was fibrotic and calcified, rendering it irreparable. Resection of the lesion and removal of the osteochondral frag-ment were performed, resulting in significant pain relief and functional recovery.
Conclusion: This case underscores the importance of early clinical suspicion and prompt ad-vanced imaging in pediatric hip trauma. Delayed diagnosis may lead to chronic changes that com-promise the feasibility of labral repair.
Keywords: Acetabular labrum, bucket-handle tear, pediatric hip, fleck sign, arthroscopy.
Acetabular labral tears are rare in pediatric patients but clinically relevant due to the labrum’s biomechanical role in joint stability, proprioception, and even load distribution. It increases the articular surface by 22% and volume by 33% [1,2]. Untreated labral lesions may lead to chronic pain, mechanical symptoms, restricted mobility, and early cartilage degeneration [3]. Among lesion patterns such as longitudinal, radial, flap, wave, or avulsion, the bucket-handle type is particularly complex, involving displacement of a torn labral fragment into the joint [4,5,6]. Posterior hip subluxation or dislocation often underlie such injuries [7], with the Fleck sign on computed tomography (CT), a posterior osteochondral fragment, serving as a key radiologic clue [8]. While bucket-handle lesions are well known in meniscal injuries, they are exceptionally rare in the acetabulum, especially in skeletally immature patients [9]. This report presents a 14-year-old patient with a bucket-handle acetabular labrum tear, highlighting diagnosis, surgical management, and clinical recovery.
Clinical history
A 14-year-old boy with no previous pathological history reported hip pain after a traumatic episode during a skiing session. The boy and his mother were skiing when the boy attempted to make a small jump, during the impact, he experienced a sudden “pop” along the hip, a clinical finding typical of an acute subluxation, and immediately afterwards reported sudden groin pain and functional impotence. The traumatic mechanism, therefore, was an axial load acting on the hip, in flexion, with subsequent posterior subluxation.
Symptoms and clinical presentation
The patient presented in orthopedic clinic 3 months after the trauma, because of a long delay to get adequate orientation and imaging. On clinical examination, the patient was able to walk without crutches, but with an antalgic gait. Persistent pain, Visual Analog Scale 6/10, pain during the weight-bearing phase of the walk. Femoral flexion was limited to 90° versus 120° on the contralateral side, and internal rotation in flexion locked at 10° versus 30° on the contralateral side. The flexion, adduction, and internal rotation test was positive and extremely painful. Episodes of joint locking in the post-traumatic weeks are suggestive of probable interposition of the displaced labral fragment between the acetabulum and femoral head.
Imaging
Magnetic resonance imaging (MRI) scans of the left hip in T2 fat-sat, short tau inversion recovery (STIR), proton density and T1 in the sagittal, coronal, and axial planes were performed to obtain a complete evaluation of the cartilaginous and bony structures [10].
The main findings are:
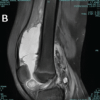
A bucket-handle lesion of the posterior acetabular labrum from 10 o’clock to 6 o’clock with involvement of the transverse ligament and protrusion into the acetabular fossa (Fig. 1).

Figure 1: Bucket-handle lesion: A displaced labral fragment is clearly observed in the posterior portion of the acetabulum, evidenced as a hypointense structure surrounded by hyperintense fluid.
Dislocated labrum fragment as a low-signal (hypointense) structure surrounded by high-signal (hyperintense) fluid in T2 fat-sat and STIR sequences, demonstrating the presence of a free intra-articular mobile fragment, probably the cause of the intermittent joint blocks (Fig. 2).
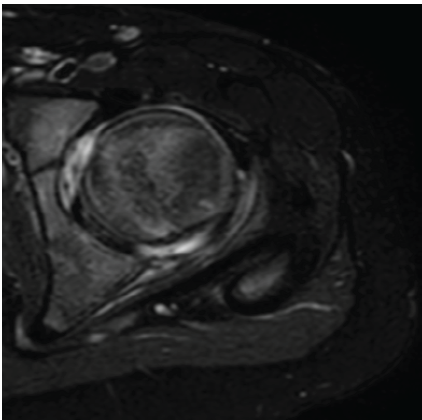
Figure 2: Arthroscopic view showing the bucket-handle lesion posteriorly interposed between the femoral head and the acetabular cartilage.
There are also several indirect signs, such as the fleck sign: avulsed bone fragment (1–2 mm) visible in T1 sequences and TC, characteristic of the corresponding osteochondral avulsion. Subchondral edema along the posterior edge of the acetabulum, suggestive of acute compressive trauma (Fig. 3).
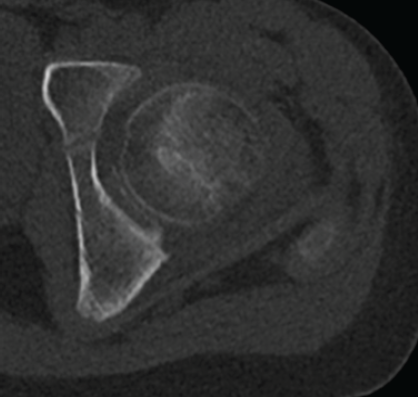
Figure 3: Fleck sign: Small bone fragment (1–2 mm) visible on computed tomography, compati-ble with associated osteochondral avulsion. The finding is located near the postero-inferior margin of the acetabulum, confirming the extent of trauma. Calcification of the acetabular labrum is also visible.
Surgical technique
Hip arthroscopy was performed to confirm the diagnosis and assess the reparability of the labral tear.
In pediatric patients, positioning and traction require special care. The patient was placed supine on a traction table with adequate padding. Minimal traction (<25 pounds) was applied only after fluoroscopic confirmation of joint distraction, avoiding unnecessary force.
Literature suggests that children are better off with less traction time and force because they have greater ligamentous laxity and smaller joint volume.[11] (Byrd and Jones 2015) [12].
With sufficient distraction confirmed (3–5 mm joint space on fluoroscopy), standard portals were established under vision: anterolateral and anteromedial.
After establishing the anteromedial and anterolateral portals, the first step was to perform an inter-portal capsulotomy with posterior extension with the aim of improving intra-articular visualization. Immediately evident inflammation of the anterior recess is noted, indicative of chronic synovitis (Fig. 4).
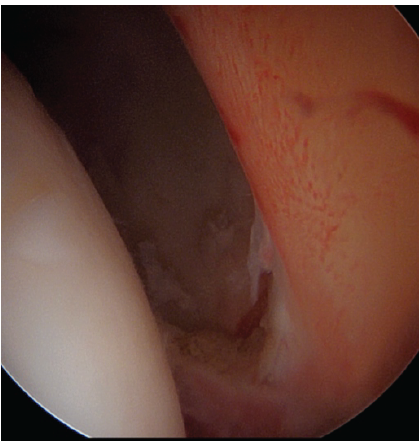
Figure 4: Arthroscopic view of a posterior stable labrum and bucket-handle lesion, with evident synovitis.
Next, the acetabular fossa is explored, where the dislocated chondro-labral fragment is observed. The lesion appears bucket-handled, extending posteriorly to inferiorly from the 10 o’clock to the 6 o’clock position, with involvement of the transverse ligament as well. The lesion involves a calcific portion of the labrum and a cartilaginous component, which extends into the acetabular fossa (Fig. 5).
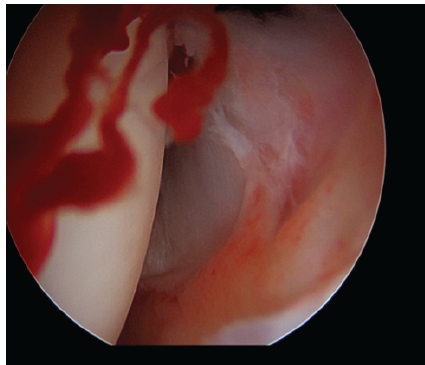
Figure 5: Clear labral tear with separation from the acetabular rim, irregular labral margins, ex-posed subchondral bone, and active intra-articular bleeding.
In this area, a posterior osteochondral fragment, corresponding to the lesion previously identified on the preoperative CT scan (Fleck sign), was clearly visualized. The fragment originated from the posterior rim of the acetabulum, consistent with an avulsion at the capsulolabral junction. However, it appeared deteriorated, irregular, and partially degenerated, with poor tissue integrity, precluding any possibility of secure fixation. The chronic inflammatory environment and poor quality of the avulsed tissue rendered anatomical reintegration unfeasible.
After a correct and accurate visualization of the lesion, the injured labral tissue was initially cauterized using a radiofrequency probe to reduce inflammation and bleeding. A debridement with a shaver was then performed to smooth the irregularities of the labrum rim and remove the diseased fibrocartilage. Finally, a grasper was used to remove the remaining calcified fragments with meticulous precision, without compromising the integrity of the surrounding structures (Fig. 6).
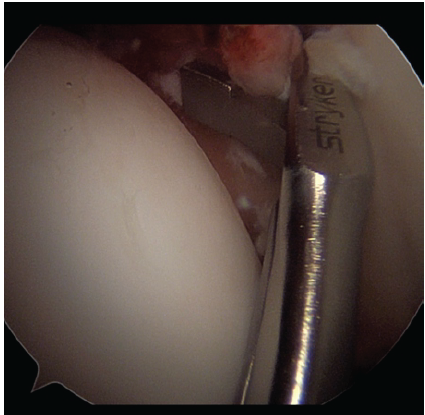
Figure 6: The remaining labral fragment was removed using a grasper, allowing precise excision of both soft tissue and calcified portions.
Complete labrum defect present from 10 to 6 o’clock with exposure of the transverse ligament and grade II Chondropathy of the overlying acetabulum according to Outerbridge calcification [13].
Evaluation of the reduction
After releasing traction, joint congruence was restored without residual fragments. Post-opearive care included partial weight-bearing for 2–4 weeks, personalized pain control, and early physiotherapy from day 0. Return to daily activities was expected within a month, based on recovery progress.
Mechanism of injury and diagnostic clues
Bucket-handle injuries of the acetabular labrum are usually the result of high-energy trauma, which can cause posterior dislocation or subluxation of the hip [14]. In these situations, the injured labrum flips back into the joint and, trapping itself, acts as a mechanical block. The presence of the “fleck sign” is a crucial radiologic clue to suspecting this pathology. Although initially described in the pediatric setting, it is now also considered significant in adults [8], Blanchard et al., 2016, [15] Rizkallah et al., 2019.
Delay in diagnosis and its consequences
In our case, the diagnosis was delayed because advanced imaging (MRI and CT) was done more than 2 months after the trauma. It is possible that the low-energy trauma did not raise concern initially. Although clinical signs such as pain, joint locking, and reduced range of motion were present, they were not initially recognized as indicative of intra-articular pathology. By the time the Fleck sign was identified on CT and the labral lesion confirmed on MRI, the pathology had already progressed: The labral tissue was fibrotic, calcified, and no longer repairable. Once the diagnosis was established, the main question was:
Was it possible to repair the lip, or was removal of the fragment the only viable option?
An alternative, which would have been evaluable only in the presence of favorable tissue conditions, would have been reinsertion of the labrum, with open or arthroscopic surgery.
Intraoperative findings and surgical decision
At surgery, the labrum fragment was small, degenerated, and morphologically irregular, ruling out the possibility of secure fixation. In addition, the lesion appeared chronic, a factor that further reduces the likelihood of successful anatomical reintegration. The literature indicates that labrum repair is contraindicated in the presence of poor tissue quality, incarceration of the fragment, or risk of post-operative impingement [16] Hwang et al., 2016. For this reason, we decided to proceed with an arthroscopic resection, which is considered the safest and most suitable solution to address the mechanical conflict and restore joint congruence.
Limits and implications of resection
This case confirms what has already been highlighted in the literature: a delay in diagnosis can critically compromise the chance of achieving anatomical and functional labral repair. Prompt clinical recognition and early imaging are essential to preserve the integrity of the labrum and maintain reconstructive options. In patients presenting with post-traumatic mechanical symptoms, the presence of Fleck’s sign should lead not only to a rapid diagnosis but also to equally rapid surgical planning [8,17]. In addition, the literature emphasizes that the ideal goal is preservation of the labrum, although this is not always possible. Several authors have highlighted that attempting to force repair in the presence of a non-reducible or unstable fragment may compromise the result, increasing the risk of impingement or joint stiffness [16] Hwang et al., 2016. In our case, we had to remove the posterolateral portion of the acetabular labrum, a crucial area for load transmission and joint stability [18,19]. Although in a young patient, removal of this area could theoretically increase the risk of early degeneration, the surgery resulted in satisfactory functional recovery and, in the short term, there were no clinical signs of instability. This highlights the importance of accurately assessing tissue quality during surgery, when repair is not feasible, removing the unstable fragment is often the safest and most effective option [20]. This case report offers interesting insights into the management of complex labral injuries. Fleck’s sign proves to be a useful radiologic marker for both diagnosis and prognosis, often related to joint instability and the need for surgery [15,17]. Even in younger patients, resection of the labrum fragment may be the best choice when tissue conditions do not allow safe and effective repair [20]. It is crucial that, after early diagnosis, prompt surgical planning is performed so as not to miss the opportunity to preserve the acetabular labrum and improve the functional outcome [21,22]. In addition to the technical-surgical aspects, this case is distinguished by its clinical rarity: in fact, it is a bucket-handle lesion of the acetabular labrum in a pediatric patient, an already exceptional condition. Making this case even more unique is the simultaneous presence of Fleck’s sign, documented by CT.
This case illustrates the diagnostic and therapeutic challenges of bucket-handle labral tears in pediatric patients. Although rare, delayed recognition can lead to joint instability, persistent pain, and early osteoarthritis. Arthroscopic synovectomy, radiofrequency ablation, and labral resection allowed safe removal of unstable, calcified tissue while preserving healthy structures. Early mobilization and tailored rehabilitation remain key for recovery. Prompt diagnosis and timely surgery are essential to preserve hip function. Future studies should explore long-term outcomes and labral healing potential in young patients.
Bucket-handle tears of the acetabular labrum in pediatric patients are exceptionally rare but should be systematically considered. In the setting of low-energy trauma with persistent symptoms such as hip pain, mechanical clicking, or locking, thorough clinical evaluation combined with advanced imaging modalities – particularly MRI and CT – is essential to establish an accurate diagnosis. Delayed presentation is not uncommon and warrants a high index of suspicion to avoid misdiagnosis or prolonged morbidity. In chronic cases resulting from delayed recognition, arthroscopic resection of the bucket-handle fragment is technically feasible and represents a safe therapeutic option, with encouraging short-term clinical outcomes. Further studies are needed to assess long-term results, particularly with respect to the potential risk of early onset osteoarthritic degeneration.
References
- 1. Mughal A, Vukanic D, Murphy EP, Crozier-Shaw G, Mahapatra A. Labral tear is associated with increased risk of osteoarthritis – a cross-sectional study. J Orthop Rep 2023;23:100185. [Google Scholar] [PubMed]
- 2. Seldes RM, Tan V, Hunt J, Katz M, Winiarsky R, Fitzgerald RH Jr. Anatomy, histologic features, and vascularity of the adult acetabular labrum. Clin Orthop Relat Res 2001;382:232-40. [Google Scholar] [PubMed]
- 3. Harris JD. Hip labral repair: Options and outcomes. Curr Rev Musculoskelet Med 2016;9:361-7. [Google Scholar] [PubMed]
- 4. Tzaveas A, Villar R. Acetabular labral and chondral pathology. Open Sports Med J 2010;4:64-74. [Google Scholar] [PubMed]
- 5. Blankenbaker DG, De Smet AA, Keene JS, Fine JP. Classification and localization of ace-tabular labral tears. Skeletal Radiol 2007;36:391-7. [Google Scholar] [PubMed]
- 6. Vendittoli PA, Young DA, Stitson DJ, Wolfe R, Del Buono A, Maffulli N. Acetabular rim lesions: Arthroscopic assessment and clinical relevance. Int Orthop 2012;36:2235-41. [Google Scholar] [PubMed]
- 7. Clement RC, Carpenter DP, Cuomo AV. Spontaneous healing of a bucket-handle posterior labral detachment after hip dislocation in a five-year-old child: A case report. JBJS Case Connect 2018;8:e28. [Google Scholar] [PubMed]
- 8. Blanchard C, Kushare I, Boyles A, Mundy A, Beebe AC, Klingele KE. Traumatic, posterior pediatric hip dislocations with associated posterior labrum osteochondral avulsion: Recog-nizing the acetabular “Fleck” sign. J Pediatr Orthop 2016;36:602-7. [Google Scholar] [PubMed]
- 9. Stabile KJ, Neumann JA, Mannava S, Howse EA, Stubbs AJ. Arthroscopic treatment of bucket-handle labral tear and acetabular fracture. Arthrosc Tech 2014;3:e283-7. [Google Scholar] [PubMed]
- 10. Shang XL, Zhang JW, Chen JW, Li YX, Chen SY. Features of acetabular labral tears on X-ray, magnetic resonance imaging and hip arthroscopy – the observational pilot study. Arch Med Sci 2013;2:297-302. [Google Scholar] [PubMed]
- 11. Byrd JW, Jones KS. Prospective analysis of hip arthroscopy with 2-year follow-up. Ar-throscopy. 2000;16:578-87. [Google Scholar] [PubMed]
- 12. Philippon MJ, Maxwell RB, Johnston TL, Schenker M, Briggs KK. Clinical presentation of femoroacetabular impingement. Knee Surg Sports Traumatol Arthrosc 2007;15:1041-7. [Google Scholar] [PubMed]
- 13. Kaya M, Uysal M, Turgut A, Ozturk H, Seyahi A, Erturk C, et al. Evaluation of acetabular cartilage lesions in patients undergoing hip arthroscopy using the Outerbridge classifica-tion system. Acta Orthop Traumatol Turc 2014;48:520-4. [Google Scholar] [PubMed]
- 14. Dameron TB Jr. Bucket-handle tear of acetabular labrum accompanying posterior disloca-tion of the hip. Clin Orthop Relat Res 2003;406:8-10. [Google Scholar] [PubMed]
- 15. Rizkallah M, Haddad M, Haykal G. Femoral head fracture in an adult patient with isolated posterior labrum avulsion recognized through the ‘fleck’ sign: Technical tips. J Hip Preserv Surg 2019;6:86-90. [Google Scholar] [PubMed]
- 16. Hwang JM, Hwang DS, Lee WY, Noh CK, Zheng L. Hip arthroscopy for incarcerated ace-tabular labrum following reduction of traumatic hip dislocation: Three case reports. Hip Pelvis 2016;28:164-8. [Google Scholar] [PubMed]
- 17. Chen S, Tulchin-Francis K, Gaines D, Kadado A, Smith C, Klingele K. Acetabular “fleck” sign: Outcomes of surgical repair. J Pediatr Orthop 2024;44:e433-8. [Google Scholar] [PubMed]
- 18. Field RE, Rajakulendran K. The labro-acetabular complex. J Bone Jt Surg 2011;93:22-7. [Google Scholar] [PubMed]
- 19. Burnett RS, Della Rocca GJ, Prather H, Curry M, Maloney WJ, Clohisy JC. Clinical presentation of patients with tears of the acetabular labrum. J Bone Joint Surg Am 2006;88:1448-57. [Google Scholar] [PubMed]
- 20. Sozen YV, Ozkan K, Goksan SB, Çiftçi F, Mutlu S, Uzer G. Arthroscopic diagnosis and treatment of an acetabular labrum bucket handle tear: A case report. Arch Orthop Trauma Surg 2005;125:649-52. [Google Scholar] [PubMed]
- 21. McCarthy JC, Noble PC, Schuck MR, Wright J, Lee J. The watershed labral lesion: Its rela-tionship to early arthritis of the hip. J Arthroplasty 2001;16:81-7. [Google Scholar] [PubMed]
- 22. Martin RL, Enseki KR, Draovitch P, Trapuzzano T, Philippon MJ. Acetabular labral tears of the hip: Examination and diagnostic challenges. J Orthop Sports Phys Ther 2006;36:503-15. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Post-traumatic Hemosiderotic Synovitis Mimicking Pigmented Villonodular Synovitis in a Non-hemophilic Child: First Reported Case from the United Arab Emirates
July 1, 2026 Post-traumatic Hemosiderotic Synovitis Mimicking Pigmented Villonodular Synovitis in a Non-hemophilic Child: First Reported Case from the United Arab Emirates June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study
June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study June 1, 2026 Standardized Preparation and Multi-Site Application of Leukocyte-Poor Platelet-Rich Plasma in Arthroscopic Anterior Cruciate Ligament Reconstruction: A Technical Note with Early Functional Outcomes
June 1, 2026 Standardized Preparation and Multi-Site Application of Leukocyte-Poor Platelet-Rich Plasma in Arthroscopic Anterior Cruciate Ligament Reconstruction: A Technical Note with Early Functional Outcomes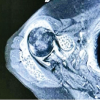 June 1, 2026 Secondary Synovial Chondromatosis of the Shoulder Associated with Rotator Cuff Tear: Diagnostic Challenge and Arthroscopic Management – A Case Report
June 1, 2026 Secondary Synovial Chondromatosis of the Shoulder Associated with Rotator Cuff Tear: Diagnostic Challenge and Arthroscopic Management – A Case Report