
This article highlights the evolving role of unilateral biportal endoscopy (UBE) from a decompression technique to a comprehensive minimally invasive approach for fusion and advanced spinal procedures.It emphasizes that while UBE offers enhanced visualization, tissue preservation, and minimally invasive advantages, its success depends on proper training, patient selection, and evidence-based adoption. The future of UBE lies in balancing innovation with reproducibility, safety, and long-term clinical validation.
Dr Akashdeep Singh Bali, Department of Neurosurgery, All India Institute of Medical Sciences (AIIMS), New Delhi, India. Email – Akashdeep.bali@aiims.edu
Abstract
Unilateral biportal endoscopy (UBE) has rapidly evolved from a decompression technique to a versatile minimally invasive platform capable of addressing complex spinal pathologies, including fusion procedures. By combining dual-portal endoscopic visualization with conventional surgical instrumentation, UBE offers enhanced ergonomics, improved visualization, reduced tissue disruption, and faster recovery. Recent advances in navigation and robotic assistance have further expanded its precision and applicability. However, the growing enthusiasm for UBE must be balanced against technical challenges, learning-curve-related complications, and the current lack of robust long-term evidence. Careful patient selection, structured training, and high-quality prospective studies remain essential. The future of UBE depends on achieving reproducible, evidence-based outcomes while continuing to drive innovation in minimally invasive spine surgery.
Keywords: Endoscopic spine , Biportal , UBE , Dual portal spine endoscopy, surgical
Unilateral biportal endoscopy (UBE) has become a trending minimally invasive approach to spine surgery. Early work was started in East Asian centers such as South Korea. The technique has progressed from simple lumbar decompression procedures to other surgical procedures such as discectomy, bilateral decompression through unilateral approaches, interbody fusion, and even some cervical and thoracic spine surgeries. The ever-expanding indication tells us a growing interest in surgical approaches that minimize tissue disruption while preserving or enhancing clinical outcomes.[1]
Spine surgery has evolved over the years toward approaches that limit tissue damage while still achieving adequate neural decompression and maintaining stability. UBE achieves this using two separate portals, one for viewing and the other for instrumentation, allowing endoscopic visualization alongside the familiarity of standard surgical tools (Fig. 1). This dual-portal setup helps overcome some of the ergonomic challenges of uniportal and tubular techniques while preserving the principles of minimally invasive surgery.[2]
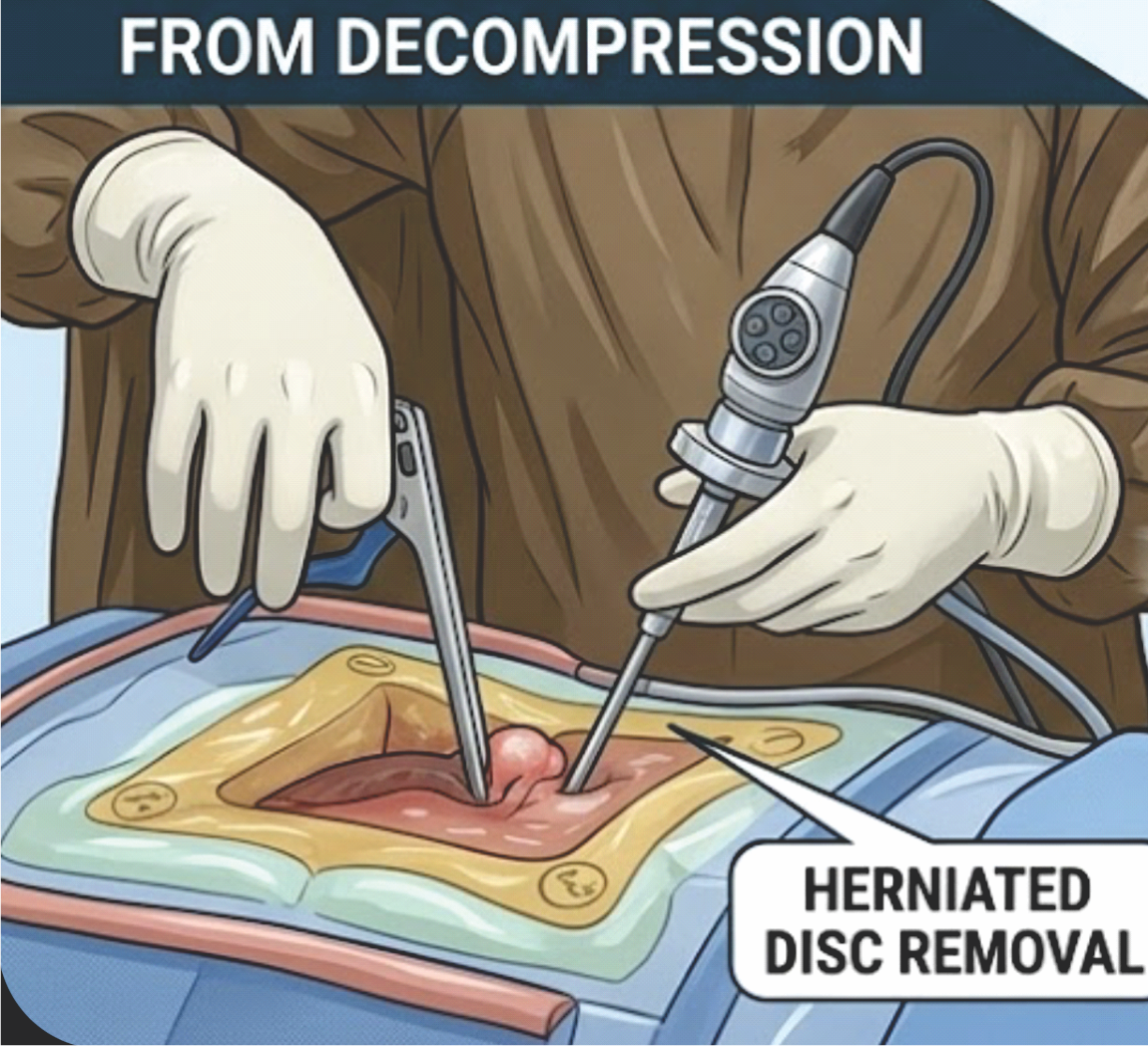
Figure 1: Unilateral biportal endoscopy, a right-handed surgeon has an instrument on right hand and the endoscope on left hand.
Continuous saline irrigation provides a clear operative field, along with endoscopic visualization, which eases access to contralateral and anatomically concealed regions. In addition, the preservation of posterior musculoligamentous structures may contribute to reduced post-operative pain and faster recovery. Early studies have illustrated promising outcomes in terms of blood loss, hospital stay, and functional recovery, particularly in lumbar decompression procedures.[2,3] These factors have led to the increasing use of UBE across a range of spinal procedures. However, the potential of UBE is beyond decompression only. Fusion procedures have a critical role in spine surgery, requiring precise endplate preparation, adequate disc clearance, accurate cage placement, and stable fixation. The application of UBE to transforaminal lumbar interbody fusion marks an important step in this direction (Fig. 2). Preliminary studies suggest that UBE-assisted fusion can achieve satisfactory clinical and radiological outcomes, with the added benefits of reduced perioperative morbidity compared to traditional open approaches.[4,5]
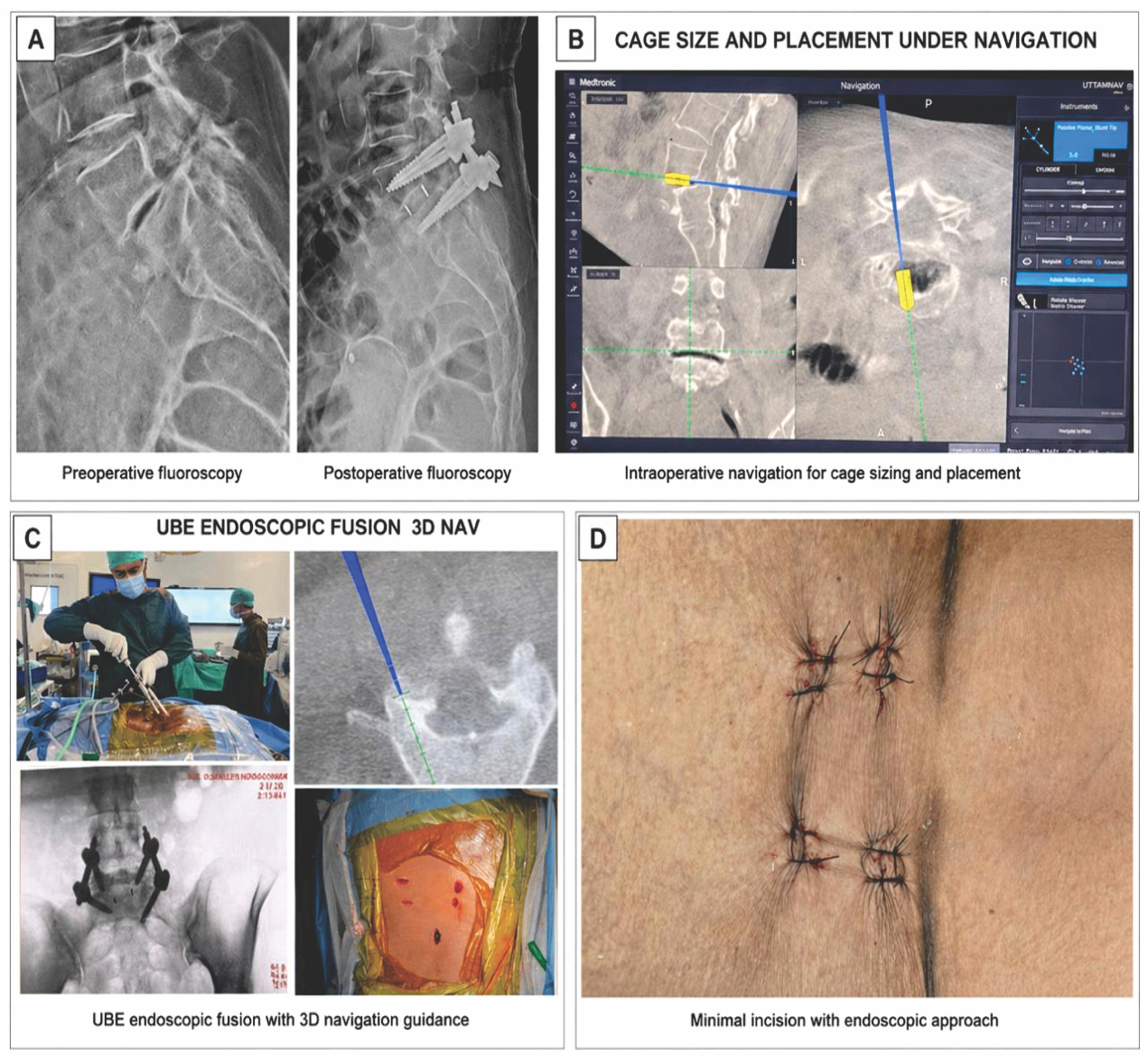
Figure 2: Well-prepared endplate with bleeding bone and cage position is visualized.
It is this evolution toward comprehensive minimally invasive spine surgery that UBE may be considered a “trailblazer.” Rather than serving as a temporary or transitional technique, UBE is leading to a meaningful shift in surgical practice, comparable to the move from open to laparoscopic surgery. By combining endoscopic visualization with the familiarity and flexibility of conventional instruments, it has the potential to influence how spinal procedures are approached.[2]
Despite its advantages, UBE is not without limitations. Continuous saline irrigation, while essential for maintaining a clear operative field, can increase epidural pressure and, if not carefully managed, may lead to fluid extravasation or post-operative neurological symptoms.[6]
Equally important is the risk of overextension of its indications. With growing interest in minimally invasive techniques, there is a tendency to apply UBE in situations where conventional approaches may still be more appropriate. In such settings, issues such as incomplete decompression, excessive facet removal, or suboptimal implant positioning can arise, particularly during the early phase of the learning curve. These concerns underscore the need for careful case selection and structured training to ensure safe and effective use of the technique.
Recent advances in intraoperative guidance are further expanding the capabilities of UBE. Conventional two-dimensional (2D) endoscopic visualization, although effective, can limit depth perception and spatial orientation during complex decompression, revision surgery, and instrumentation. The introduction of three-dimensional (3D) navigation systems has addressed some of these limitations by providing real-time anatomical guidance and improved accuracy. Navigation-assisted UBE has been shown to enhance intraoperative precision, facilitate targeted decompression, and improve safety, particularly in anatomically challenging regions.[7]
In addition, 3D navigation-guided UBE techniques have demonstrated the ability to preserve facet integrity while achieving adequate decompression, with improved visualization of foraminal pathology and more accurate localization of disc fragments. The integration of robotic-assisted platforms with navigation further builds on this concept by enhancing the accuracy of pedicle screw placement, reducing radiation exposure, and improving procedural reproducibility. While these technologies are still evolving, they represent an important step toward greater precision and standardization in minimally invasive spine surgery.[8,9]
Despite its growing appeal, the expansion of UBE has outpaced the development of robust supporting evidence. Much of the current literature is retrospective and single-center experiences, often from high-volume centers with considerable expertise. While these reports offer useful early insights, they are subject to selection bias and have limited generalizability.[6] Comparative data against established minimally invasive and open techniques remain limited, and long-term outcomes, particularly regarding fusion rates, recurrence, and revision surgery, are not yet well reported.
The learning curve of UBE should not be underestimated. Despite being familiar in concept to surgeons with open or microscopic experience, it requires skill in endoscopy, fluid control, and bimanual handling. Early experience may be associated with longer operative times and complications such as dural tears, incomplete decompression, epidural hematoma, or excessive facet resection, and results from specialized centers may not be readily reproducible in general practice.[10,11,12]
A measured approach is necessary when extending the indications of UBE. The technical feasibility of performing increasingly complex procedures using UBE should not be equated with clinical superiority. Careful patient selection and adherence to established surgical principles remain essential.[13]
At the same time, it would be premature to dismiss UBE as a transient trend. The evolution of spine surgery has historically been characterized by incremental advances rather than abrupt paradigm shifts. Its ability to combine familiar surgical ergonomics with enhanced visualization offers a unique platform for further innovation.
Looking ahead, the role of endoscopic techniques in spine surgery is likely to extend beyond conventional decompression and fusion. Emerging applications, such as endoscopic rhizotomy for chronic pain syndromes, point toward a broader therapeutic scope, particularly where direct visualization may enhance the precision of treatment.[14] However, definitive progress will depend not only on technological advancement but also on careful validation, appropriate patient selection, and structured training.
The future of UBE will ultimately be determined by the strength of the evidence supporting its use. Prospective multicenter studies, standardized outcome reporting, and long-term follow-up are essential to define its role alongside established techniques and to ensure consistent, reproducible results.
In this context, UBE represents both an opportunity and a responsibility. While it offers the potential to reduce surgical morbidity and expand the reach of minimally invasive spine surgery, its continued evolution must remain grounded in rigorous scientific evaluation rather than enthusiasm alone. Its position as a trailblazer will depend not only on innovation, but on evidence, reproducibility, and sustained clinical benefit.
References
- 1. Mohamed KS, Kurapatti M, Yang E, Alasadi H, Ahmed W, Lamidi RA, et al. Biportal endoscopic spine surgery: Evolution of techniques, indications, and influential literature. J Clin Med 2026;15:1843. [Google Scholar] [PubMed]
- 2. Kim JE, Choi DJ, Park EJJ, Lee HJ, Hwang JH, Kim MC, et al. Biportal endoscopic spinal surgery for lumbar spinal stenosis. Asian Spine J 2019;13:334-42. [Google Scholar] [PubMed]
- 3. Xu WB, Kotheeranurak V, Zhang HL, Chen ZX, Wu HJ, Chen CM, et al. Is biportal endoscopic spine surgery more advantageous than uniportal for the treatment of lumbar degenerative disease? A meta-analysis. Medicina (Mex) 2022;58:1523. [Google Scholar] [PubMed]
- 4. Heo DH, Son SK, Eum JH, Park CK. Fully endoscopic lumbar interbody fusion using a percutaneous unilateral biportal endoscopic technique: technical note and preliminary clinical results. Neurosurg Focus 2017;43:E8. [Google Scholar] [PubMed]
- 5. Park CW, Anzar AM, Yoo BS, Yoon JE, Kim JH, Park WM. Clinical and radiologic outcomes of biportal endoscopic lumbar interbody fusion with a long polyetheretherketone cage. J Minim Invasive Spine Surg Tech 2023;8(Suppl 1):S62-71. [Google Scholar] [PubMed]
- 6. Santander XA, Stienen MN, Motov S, Quintanilla HU, Pérez EG. Complications and their prevention in unilateral biportal endoscopy: A systematic review with narrative insights and practical management algorithms. Acta Neurochir (Wien) 2026;168:27. [Google Scholar] [PubMed]
- 7. Hadgaonkar S, Nagpal S, Bhute A, Sancheti P. A prospective pilot study on navigation-guided unilateral biportal endoscopic spine surgery: Feasibility, workflow, and early outcomes. J Clin Orthop Trauma 2025;70:103206. [Google Scholar] [PubMed]
- 8. Hadgaonkar S, Shah PK, Sancheti PK. 3D-Navigation guided sublaminar contralateral unilateral biportal endoscopy (UBE) for migrated foraminal disc in the lumbar spine: A technical note and case series. Surg Neurol Int 2026;17:76. [Google Scholar] [PubMed]
- 9. Hagan MJ, Remacle T, Leary OP, Feler J, Shaaya E, Ali R, et al. Navigation techniques in endoscopic spine surgery. BioMed Res Int 2022;2022:8419739. [Google Scholar] [PubMed]
- 10. Xu J, Wang D, Liu J, Zhu C, Bao J, Gao W, et al. Learning curve and complications of unilateral biportal endoscopy: Cumulative sum and risk-adjusted cumulative sum analysis. Neurospine 2022;19:792-804. [Google Scholar] [PubMed]
- 11. Choi DJ, Choi CM, Jung JT, Lee SJ, Kim YS. Learning curve associated with complications in biportal endoscopic spinal surgery: Challenges and strategies. Asian Spine J 2016;10:624. [Google Scholar] [PubMed]
- 12. Kim JE, Yoo HS, Choi DJ, Hwang JH, Park EJ, Chung S. Learning curve and clinical outcome of biportal endoscopic‐assisted lumbar interbody fusion. BioMed Res Int 2020;2020:8815432. [Google Scholar] [PubMed]
- 13. Chen KT, Kim JS, Huang APH, Lin MHC, Chen CM. Current indications for spinal endoscopic surgery and potential for future expansion. Neurospine 2023;20:33-42. [Google Scholar] [PubMed]
- 14. Du R, Xu G, Bai X, Li Z. Facet joint syndrome: Pathophysiology, diagnosis, and treatment. J Pain Res 202;15:3689-710. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Establishing Minimal Clinically Important Difference and Patient Acceptable Symptom State Thresholds for Patient-Reported Outcome Measures in Acromioclavicular Joint Arthropathy: A Prospective Cohort Study
May 1, 2026 Establishing Minimal Clinically Important Difference and Patient Acceptable Symptom State Thresholds for Patient-Reported Outcome Measures in Acromioclavicular Joint Arthropathy: A Prospective Cohort Study March 10, 2024 Extra-oral, Non-mucosal Approach for Oncologic Resections of the Mandible: A Case Series
March 10, 2024 Extra-oral, Non-mucosal Approach for Oncologic Resections of the Mandible: A Case Series March 11, 2017 Modified Nicoll’s Graft for Treatment of Gap Non-union of Ulna: A Rare Case Report
March 11, 2017 Modified Nicoll’s Graft for Treatment of Gap Non-union of Ulna: A Rare Case Report January 10, 2018 Evidence Based Medicine: What is it true value in clinical practice?
January 10, 2018 Evidence Based Medicine: What is it true value in clinical practice?