
Survival analysis is essential in orthopaedics for evaluating how long treatments remain effective and for identifying factors that influence implant survival, revision, and patient outcomes. It also shows that methods such as Kaplan-Meier analysis, log-rank testing, Cox regression, and competing risks analysis help clinicians make better long-term, data-driven decisions in joint, fracture, and spine care.
Dr. Arvind J Vatkar, Department of Orthoapedics, MGM Medical College, Navi Mumbai, Maharashtra, India. E-mail: vatkararvind@gmail.com
Abstract
Survival analysis is critical in orthopaedics for determining how long procedures such as joint replacements and spinal operations are successful. Traditional approaches do not account for the timing of events such as implant failure or problems, whereas survival analysis does, allowing surgeons to make informed judgments. Key approaches for assessing risk variables and implant lifetime include Kaplan-Meier curves, log-rank tests, and Cox regression. This approach improves the evaluation of treatments across joint arthroplasty, fracture care, and spine surgery. Despite limitations such as data shortages and model assumptions, combining survival analysis with emerging technologies such as electronic health records and artificial intelligence improves personalised patient care and long-term outcome prediction, eventually leading to better surgical treatment.
Keywords: survival analysis, Kaplan-Meier, orthopaedics, Cox regression
Why survival analysis matters in orthopaedics
Survival analysis, a key component of biostatistics, is an effective method for investigating time-to-event data. In orthopaedics, where treatments such as joint replacements or spinal procedures may last for many years, this technique of survival analysis provides vital insights into long-term efficacy and patient outcomes. Unlike standard statistical methods, which focus on binary outcomes (e.g., success or failure), survival analysis captures when events occur such as implant failure, illness recurrence, or patient mortality [1]. This temporal perspective enables doctors to make data-driven decisions, which improves patient care.
Core techniques in survival analysis
Several techniques underpin survival analysis, each tailored to specific questions in orthopaedics:
Kaplan-Meier analysis
The Kaplan-Meier estimator, a non-parametric approach, calculates the survival function, or the chance of an event not happening over time. The Kaplan-Meier estimator is named after, Edward L. Kaplan and Paul Meier, who collaborated in 1958 to produce a study on analysing time-to-event data. The Kaplan-Meier estimator measures the frequency and number of individuals who survive medical therapy. Kaplan-Meier curves and survival estimates are now preferred methods for analysing cohort studies [2]. The Kaplan Meier estimate is also known as the Product Limit Estimate. The product-limit formula calculates the percentage of organisms or physical objects that survive beyond a given age t, even if some things do not die or fail and the sample size is tiny [3]. In orthopaedics, it is commonly used to plot survival curves for implant lifetime [4]. For example, a 2020 research published in The Journal of Bone and Joint Surgery utilised Kaplan-Meier curves to indicate that ceramic-on-ceramic hip implants had a 95% survival rate at 15 years, compared to 89% for metal-on-metal. These curves are easy to understand and use to compare treatment groups and guide healthcare decisions [5].
Log-rank test
The log-rank test is a statistical method used to compare survival functions of two or more groups, such as treatment and control groups or different treatment groups in a clinical trial. It tests the null hypothesis, which states that populations do not differ in the probability of an event at any time point. The test can be generated using statistical software like Statistical Package for the Social Sciences, SAS, Stata, and R packages. The null hypothesis is rejected when the P-value is less than the alpha level, usually 0.05 or fails to be rejected when the P-value is large. It cannot estimate the size of the difference between confidence intervals and groups [3]. The PearlDiver Research Program analyzed patients undergoing primary occipitocervical or atlanto-axial fusions between 2007 and 2017. Kaplan Meier survival analysis, log rank test and Cox-proportional hazards revealed a greater risk of revision following surgery for occipitocervical fusion, with a higher incidence of complications [6]. (Table 1).
Cox proportional hazards model
The Cox model quantifies how factors such as age, body mass index, and implant type influence the hazard rate (risk of an occurrence). The proportional hazards assumption means that the ratio of risk (hazard) between different groups always stays the same over time, no matter when you measure it. This makes it possible to compare survival rates and confidently estimate the effect of treatments or risk factors. If the assumption is broken, the results from Cox regression may not be accurate or reliable [7]. All-cause revision, a common outcome in total joint replacement research, includes all causes of revision, such as infection, loosening, and periprosthetic fracture, highlighting the varying susceptibility of diseases and the need for a more comprehensive understanding of these factors [8]. A study in 2023 by Stan et al., examines the survivorship and dislocation rate of a semi-retentive cemented acetabular cup as a primary implant with Cox multiple regression model. The study suggests that the semi-constrained design may cause frequent damage to the polyethylene liner, leading to failure. The implant may be beneficial for elderly patients with low-demanding lifestyles and low compliance with hip prosthetic behavior [9].
Competing risks analysis
In orthopaedics, conflicting events, such as death prior to implant failure, might distort results. This is addressed through the examination of competing hazards. For example, The study in European spine journal employed competing risk analysis to evaluate postoperative complications and reoperations after spinal surgery in multiple myeloma patients. Factors like decompression surgery type, steroid use, and clinical parameters affected complication incidence and retreatment risk, highlighting the importance of comprehensive risk modeling for optimized surgical management in this high-risk cohort [10].
Time-dependent covariates
Orthopaedic conditions evolve. For example, a patient’s weight-bearing capacity following fracture surgery varies over time. Betz et al in their study used time-dependent variables collected up to 6 months post-knee replacement to improve chronic postsurgical pain prediction. Incorporating dynamic clinical and patient-reported outcomes enhanced model accuracy compared to preoperative data alone, demonstrating the value of longitudinally monitored variables for better individualized prognosis in orthopedic pain management [11].
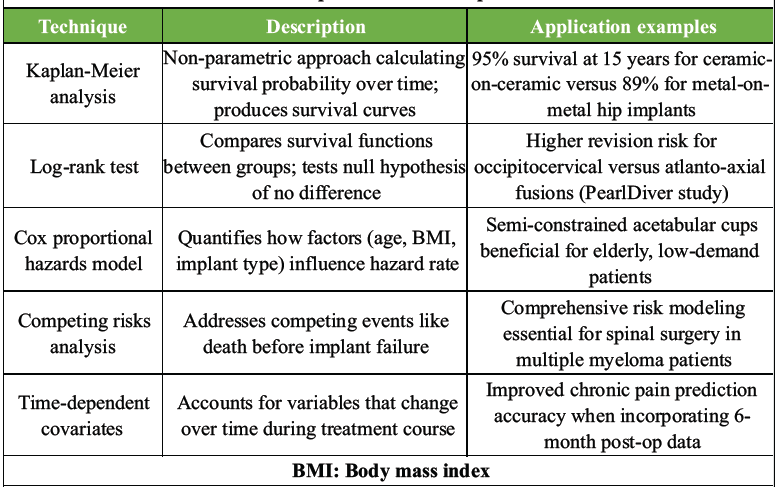
Table 1: The table shows the various core techniques used in survival analysis in orthopaedics with examples
Real-world applications
Survival analysis transforms orthopaedic research across domains:
- Joint arthroplasty: The article in the journal of arthroplasty in March 2025, used Kaplan-Meier survivorship analysis to estimate implant survival free of revision or reoperation after ceramic-on-highly crosslinked polyethylene total hip arthroplasty in 5,536 cases. The method provided 5-year survivorship estimates of 97% for revision-free and 96% for reoperation-free outcomes, demonstrating excellent midterm implant durability. Common failure causes were also identified. Kaplan-Meier helped track implant longevity and failure timing over follow-up [12]
- Fracture management: A multicenter study used Kaplan-Meier survival analysis to evaluate 12-month mortality in patients with unstable intertrochanteric hip fractures treated with three implant types. It demonstrated lower mortality with cephalomedullary nails compared to sliding hip screws and provided survival probability estimates critical for comparing implant efficacy in trauma care [13]
- Spinal surgery: A study used Kaplan-Meier survival analysis to evaluate revision surgery rates following primary fusion in adult idiopathic scoliosis patients. The analysis showed a linear increase in revision risk, nearing 20% at 10 years. Fusion length and lower fusion limit were identified as key independent risk factors for revision surgery [14]
- Oncological orthopaedics: A study used Kaplan–Meier survival analysis to evaluate survival in 110 patients with femoral metastases treated by nailing or resection. Results showed better survival with impending fractures versus actual fractures and higher survival after resection than nailing, highlighting pathological fracture impact on prognosis and treatment choice [15]
- Survival analysis in this study clarified that patients with solitary or limited resectable skeletal metastases from renal cell carcinoma have better survival outcomes. Kaplan-Meier curves showed significantly higher survival in these groups, supporting surgery as the preferred treatment over ineffective radiation and chemotherapy for improving local control and survival [16].
Challenges and pitfalls
Survival analysis has strengths but also limitations. Missing follow-up data can bias results, and inconsistent definitions (e.g., of implant failure) complicate comparisons. The Cox model’s assumption that risks stay constant over time may be violated, leading to wrong conclusions. Also, statistical significance doesn’t always mean clinical importance—small differences might not justify costlier treatments [17].
The future of survival analysis
Advancements in data collection through electronic health records and wearable devices are transforming survival analysis by providing continuous, rich longitudinal data. Smart implants can monitor real-time load bearing, enhancing time-to-event data quality. Integration of machine learning with traditional survival models enables higher accuracy in predicting outcomes. This article studied survival in stage I–III breast cancer patients using SEER-Medicare data (1991–2016). Unlike older models based only on diagnosis, our deep learning model also included later factors like treatments, side effects, other illnesses, and aging. This reduced prediction errors from 30% to under 10%, enabling personalized survival estimates [17,18].
Survival analysis is a key component of orthopaedics, providing insight into the long-term efficacy of therapies and patient outcomes. Researchers may understand the intricacies of time-to-event data by using methodologies such as Kaplan-Meier, Cox models, and competing risks analysis. As technology advances, combining survival analysis with artificial intelligence and real-time data will improve our capacity to provide personalised, effective treatment, altering patients’ lives one at a time.
References
- 1. Gillam MH, Ryan P, Graves SE, Miller LN, De Steiger RN, Salter A. Competing risks survival analysis applied to data from the Australian orthopaedic association national joint replacement registry. Acta Orthop 2010;81:548-55. [Google Scholar] [PubMed]
- 2. Etikan I, Abubakar S, Alkassim R. The kaplan meier estimate in survival analysis. Biom Biostat Int J 2017;5:55-9. [Google Scholar] [PubMed]
- 3. Kaplan EL, Meier P. Non-parametric Estimation from Incomplete Observations. J Am Stat Assoc 1958;53:457-81. [Google Scholar] [PubMed]
- 4. Lacny S, Wilson T, Clement F, Roberts DJ, Faris PD, Ghali WA, et al. Kaplan-meier survival analysis overestimates the risk of revision arthroplasty: A meta-analysis. Clin Orthop Relat Res 2015;473:3431-42. [Google Scholar] [PubMed]
- 5. Howard DP, Wall PD, Fernandez MA, Parsons H, Howard PW. Ceramic-on-ceramic bearing fractures in total hip arthroplasty: An analysis of data from the National Joint Registry. Bone Joint J 2017;99-B:1012-9. [Google Scholar] [PubMed]
- 6. Yang DS, Patel SA, DiSilvestro KJ, Li NY, Daniels AH. Postoperative complication rates and hazards-model survival analysis of revision surgery following occipitocervical and atlanto-axial fusion. N Am Spine Soc J 2020;3:100017. [Google Scholar] [PubMed]
- 7. Deo SV, Deo V, Sundaram V. Survival analysis-part 2: Cox proportional hazards model. Indian J Thorac Cardiovasc Surg 2021;37:229-33. [Google Scholar] [PubMed]
- 8. Kuitunen I, Ponkilainen VT, Uimonen MM, Eskelinen A, Reito A. Testing the proportional hazards assumption in cox regression and dealing with possible non-proportionality in total joint arthroplasty research: Methodological perspectives and review. BMC Musculoskelet Disord 2021;22:489. [Google Scholar] [PubMed]
- 9. Stan G, Roman MD, Orban H, Georgeanu VA, Deculescu RS, Brinduse LA, et al. Survival analysis and failure modes of total hip arthroplasty using a cemented semi-retentive acetabular cup. J Clin Med 2023;12:7506. [Google Scholar] [PubMed]
- 10. Zijlstra H, Pierik RJ, Crawford AM, Tobert DG, Wolterbeek N, Oosterhoff JH, et al. Analysis of complications and revisions after spine surgery in 270 multiple myeloma patients with spinal involvement. Eur Spine J 2023;32:4335-54. [Google Scholar] [PubMed]
- 11. Betz U, Clarius M, Krieger M, Konradi J, Kuchen R, Schollenberger L, et al. Time-dependent prediction models for individual prognosis of chronic postsurgical pain following knee replacement based on an extensive multivariable data set. J Clin Med 2024;13:862. [Google Scholar] [PubMed]
- 12. Hannon CP, Salmons HI, Trousdale RT, Lewallen DG, Berry DJ, Abdel MP. Why are contemporary primary ceramic-on-highly crosslinked polyethylene total hip arthroplasties failing? An analysis of over 5,500 cases. J Arthroplasty 2025;40:711-7. [Google Scholar] [PubMed]
- 13. Tucker A, Donnelly KJ, Rowan C, McDonald S, Foster AP. Is the best plate a nail? A review of 3230 unstable intertrochanteric fractures of the proximal femur. J Orthop Trauma 2018;32:53-60. [Google Scholar] [PubMed]
- 14. Riouallon G, Bouyer B, Wolff S. Risk of revision surgery for adult idiopathic scoliosis: A survival analysis of 517 cases over 25 years. Eur Spine J 2016;25:2527-34. [Google Scholar] [PubMed]
- 15. Mavrogenis AF, Pala E, Romagnoli C, Romantini M, Calabro T, Ruggieri P. Survival analysis of patients with femoral metastases. J Surg Oncol 2012;105:135-41. [Google Scholar] [PubMed]
- 16. Fottner A, Szalantzy M, Wirthmann L, Stähler M, Baur-Melnyk A, Jansson V, et al. Bone metastases from renal cell carcinoma: Patient survival after surgical treatment. BMC Musculoskelet Disord 2010;11:145. [Google Scholar] [PubMed]
- 17. Moncrieff J, Jakobsen JC, Bachmann M. Later is not necessarily better: Limitations of survival analysis in studies of long-term drug treatment of psychiatric conditions. BMJ Evid Based Med 2022;27:246-50. [Google Scholar] [PubMed]
- 18. Adam N, Wieder R. AI survival prediction modeling: The importance of considering treatments and changes in health status over time. Cancers (Basel) 2024;16:3527. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2025 Elevating Orthopaedic Care through Materiovigilance
June 1, 2025 Elevating Orthopaedic Care through Materiovigilance June 1, 2025 Ilizarov-Assisted Reduction of Femoral Condyle Locked in Tibial Fracture: A Case Report
June 1, 2025 Ilizarov-Assisted Reduction of Femoral Condyle Locked in Tibial Fracture: A Case Report March 1, 2025 Simultaneous Bilateral Knee Extensor Mechanism Injury in a Young Male: A Clinical Diagnosis and Literature Review
March 1, 2025 Simultaneous Bilateral Knee Extensor Mechanism Injury in a Young Male: A Clinical Diagnosis and Literature Review January 1, 2025 Safe Surgery is Everyone’s Responsibility
January 1, 2025 Safe Surgery is Everyone’s Responsibility