
[box type=”bio”] Learning Point for the Article: [/box]
TB of isolated radial head without involvement of distal humerus and proximal ulna is rarely reported. Its diagnosis is often misleading and hence mismanagement may occur. A combination of a high index of clinical suspicion based on good history taking, clinical and radiological (including MRI) examination and biopsy is essential to establish the diagnosis. Biopsy allows demonstrating the presence of mycobacterium TB by CB-NAAT (Cartridge Based Nucleic Acid Amplification Test) method and in culture and tuberculoma in histopathology so that early appropriate treatment can be instituted for a painless, stable and normally functioning elbow joint.
Case Report | Volume 8 | Issue 3 | JOCR May – June 2018 | Page 28-32| Naba Pallab Chetia, Aritra Bidyananda, Manabjyoti Talukdar, Munin Borgohain. DOI: 10.13107/jocr.2250-0685.1094
Authors: Naba Pallab Chetia[1], Aritra Bidyananda[1], Manabjyoti Talukdar[2], Munin Borgohain[1]
[1]Department of Orthopaedics, Assam Medical College and Hospital, Dibrugarh, Assam, India.
[2]Department of Orthopaedics, Silchar Medical College and Hospital, Assam, India.
Address of Correspondence:
Dr. Naba Pallab Chetia,
Department of Orthopaedics, Assam Medical College and Hospital, Dibrugarh – 786 002, Assam, India.
E-mail: dr.npchetia11@gmail.com
Abstract
Introduction: Tuberculosis (TB) of isolated radial head is scantily reported in the literature. Nonspecific symptoms and difficulty in interpreting initial screening radiographs often lead to misdiagnosis.
Case Report: We present a case of 42-year-old male elsewhere diagnosed as pyogenic arthritis of left elbow and treated by incisional drainage and broad-spectrum antibiotics, who presented to us 6 months later with multiple non-healing actively discharging sinuses. The repeat radiographs and Magnetic Resonance Imaging (MRI) were reported as chronic osteomyelitis of proximal radius without the involvement of humerus and ulna. The excision of radial head along with sinus tracts was done for clearance of disease and excised tissues, on being subjected to Cartridge Based Nucleic Acid Amplification Test (CB-NAAT), culture and histopathological examination, the diagnosis of TB was established.
Conclusion: The diagnosis of TB of the elbow is generally delayed & mismanagement may occur. Therefore, not only biopsy is essential to demonstrate the presence of mycobacterium TB by CB-NAAT (Cartridge Based Nucleic Acid Amplification Test) method and in culture but also the presence of tuberculoma in histopathology is essential to establish the diagnosis so that early appropriate treatment can be instituted.
Keywords: Tuberculosis, isolated radial head, CBNAAT
Introduction
Tuberculosis (TB) of skeletal system involvement is seen in 1–3% of the patients and 10% of all extra pulmonary TB [1]. The sites most commonly involved are the spine (51%), the pelvis (12%), the hip and femur (10%), the knee and tibia (10%), and the ribs (7%) [2]. Mycobacterial infection of the upper extremities is extremely rare [3, 4]. Elbow is the most frequently involved joint in the upper limb, accounting for 2–5% of all skeletal localizations [5]. In tuberculosis of elbow, the most common site is the proximal ulna followed by distal humerus [5, 6, 7]. However, the incidence of isolated radial head involvement without involving distal humerus and proximal ulna is scantily reported in the literature. Usually, the diagnosis of elbow TB is delayed because of nonspecific symptoms and difficulty in interpreting screening radiographs in the initial stages [6, 8]. Often the clinical presentation closely mimics septic arthritis and is treated accordingly [8]. We report our experience in the challenge of diagnosis and management of a case of TB of isolated radial head without the involvement of distal humerus and proximal ulna in a 42-year-old male patient.
Case Report
A 42-year-old male developed an insidious onset swelling on the ventral aspect of left elbow 6 months back for which he consulted elsewhere. Following radiological and blood investigations, he was diagnosed as pyogenic arthritis for which incision and drainage were performed followed by broad-spectrum antibiotics for 3 weeks. Subsequently, he developed multiple persistent discharging sinuses. He also had pain over the left elbow which was aggravated during movement and activities. Range of movement of his left elbow was restricted. There was no h/o trauma, constitutional symptoms such as fever, night cry, loss of appetite, and body weight. Other joints were not involved. There was no past or contact history of TB. Examination revealed two discharging sinuses; one on the ventral aspect and another on the dorsal aspect of left elbow (Fig. 1). Discharge of pus from the sinuses was evident but no h/o history of bony spicules is coming out. Elbow range of motion was 10°–10°–110° and muscles of arm and forearm were wasted. Epitrochlear and axillary lymph nodes were not palpable. Distal neurovascular status was intact. Plain radiograph of the left elbow joint showed irregularity of proximal radius mainly in the metadiaphyseal region and mild periosteal reaction (Fig. 2). Sinogram of the affected side showed a blind-ending linear tract suggestive of sinus formation (Fig. 3).  Magnetic Resonance Imaging of elbow joint revealed focal widening of medullary cavity of proximal radius affecting metadiaphyseal region and large bony defect (8.2 mm) in the anterolateral cortex of proximal radius communicating with the skin through a well-defined sinus tract which opens on the ventral aspect of elbow (Fig. 4).
Magnetic Resonance Imaging of elbow joint revealed focal widening of medullary cavity of proximal radius affecting metadiaphyseal region and large bony defect (8.2 mm) in the anterolateral cortex of proximal radius communicating with the skin through a well-defined sinus tract which opens on the ventral aspect of elbow (Fig. 4).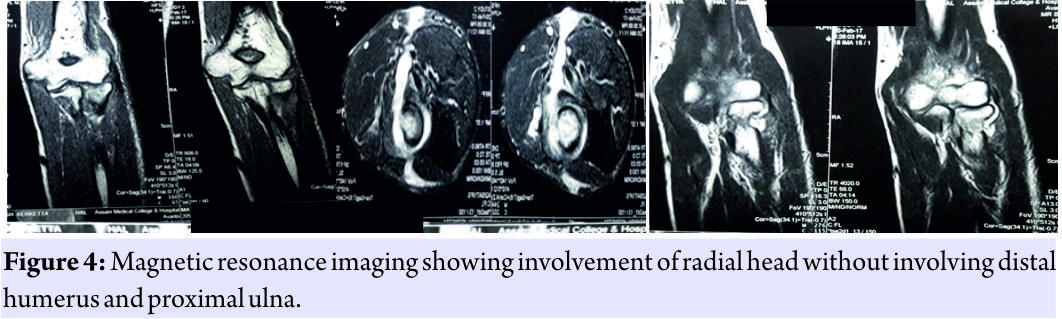 Two sinus tracts, one posteromedially and another laterally directed sinus tracts were noted from the affected radius into the subcutaneous plane. No articular extension and involvement of humerus and ulna were seen.These findings were reported as suggestive of chronic osteomyelitis of upper end of the radius with cloaca formation in the anterolateral cortex with sinus tracts formation. Blood parameters were within normal limit except minimal rise in erythrocyte sedimentation rate (33 mm/1 h) and quantitative C-reactive protein (2.43). Chest X-ray was found to be normal. As the patient was an adult and attained skeletal maturity, he underwent radial head excision following exposure by Kocher’s approach [9] along with excision of sinus tract under GA brachial block. The excised specimen (Fig. 5) was sent for Gram staining, Ziehl-Nielson (Z-N) staining for Acid Fast Bacilli (AFB), Cartridge Based Nucleic Acid Amplification Test (CB-NAAT) examination, culture for pyogenic and tubercle bacilli and histopathology for etiological diagnosis. Although mycobacterium TB was detected by real time Polymerase Chain Reaction (PCR) method on gene expert platform, acid-fast bacilli was not detected in Z N staining. The histopathological examination showed tuberculoma with central caseation (Figure 6).
Two sinus tracts, one posteromedially and another laterally directed sinus tracts were noted from the affected radius into the subcutaneous plane. No articular extension and involvement of humerus and ulna were seen.These findings were reported as suggestive of chronic osteomyelitis of upper end of the radius with cloaca formation in the anterolateral cortex with sinus tracts formation. Blood parameters were within normal limit except minimal rise in erythrocyte sedimentation rate (33 mm/1 h) and quantitative C-reactive protein (2.43). Chest X-ray was found to be normal. As the patient was an adult and attained skeletal maturity, he underwent radial head excision following exposure by Kocher’s approach [9] along with excision of sinus tract under GA brachial block. The excised specimen (Fig. 5) was sent for Gram staining, Ziehl-Nielson (Z-N) staining for Acid Fast Bacilli (AFB), Cartridge Based Nucleic Acid Amplification Test (CB-NAAT) examination, culture for pyogenic and tubercle bacilli and histopathology for etiological diagnosis. Although mycobacterium TB was detected by real time Polymerase Chain Reaction (PCR) method on gene expert platform, acid-fast bacilli was not detected in Z N staining. The histopathological examination showed tuberculoma with central caseation (Figure 6). 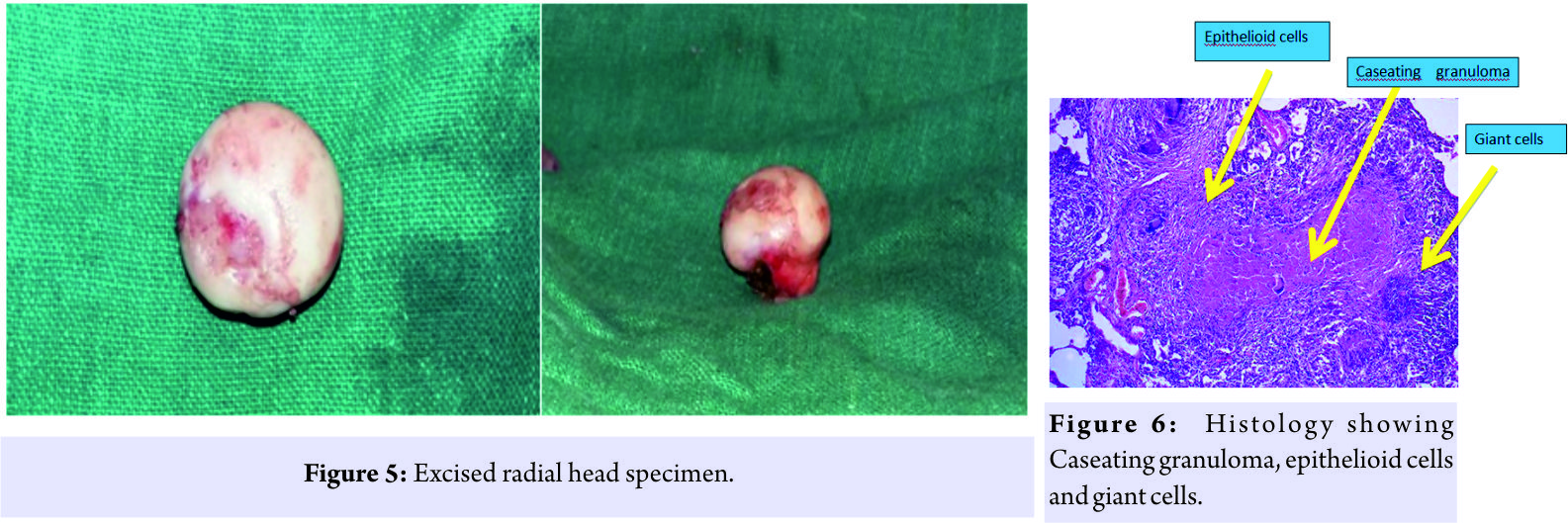 Rifampicin resistance was not detected. A baseline Liver Function Test (LFT) was done which showed normal parameters. Multidrug antitubercular therapy was started under category 1 under directly observed treatment short course which includes intensive phase of 2 months of isoniazid, rifampicin, ethambutol, and pyrazinamide; continuation phase of 7 months of isoniazid and rifampicin. Elbow was splinted for 2 weeks until subsidence of pain and spasm and then weaned for active and assisted range of motion exercises within pain limits.
Rifampicin resistance was not detected. A baseline Liver Function Test (LFT) was done which showed normal parameters. Multidrug antitubercular therapy was started under category 1 under directly observed treatment short course which includes intensive phase of 2 months of isoniazid, rifampicin, ethambutol, and pyrazinamide; continuation phase of 7 months of isoniazid and rifampicin. Elbow was splinted for 2 weeks until subsidence of pain and spasm and then weaned for active and assisted range of motion exercises within pain limits.
Patient was followed up regularly by clinical examination, blood investigations like Hemoglobin %, blood cell count, LFT etc. and radiographs of left elbow. No drug related ad verse effect was reported by the patient during treatment. At final follow up on completion of antitubercular drugs, the sinuses healed (Figure 9), elbow became painless with full range of motion (Figure 8) and normal functional ability.
Discussion
TB of the elbow, like pyogenic arthritis, is characteristically a monoarticular disease, although multifocal osteoarticular TB does occur [5, 10, 11]. Although elbow joint is most frequently involved in the upper extremity followed by shoulder joint [6, 12], the available information on TB of elbow is scarce as only a few cases are seen annually even in centers located in TB endemic zones [1]. TB of isolated proximal radius without concurrent involvement of distal humerus and proximal ulna is even rarer in literature. Aggrawal and Dhammi reported 8 cases of concurrent proximal radius involvement out of 48 TB elbow in their series [6]. Agarwal reported 3 cases of concurrent proximal radius involvement out of 10 TB elbow in children in their series [1]. The diagnosis of TB of the elbow is generally delayed because the lesion is relatively uncommon and there is a lack of awareness among clinicians, especially in non-endemic areas [2]. TB should be considered in the diagnosis of monoarthritis in developing countries [13]. Osteoarticular TB should be suspected in patients of South Asian and African origin presenting with bony and soft tissue infective lesions [1]. Early diagnosis and treatment are possible through a combination of good history taking, clinical and radiological examination and a high degree of clinical suspicion [2]. Usually, due to the late presentation and/or delay in diagnosis, the significant osteoarticular damage is already present [2, 5]. The onset is usually insidious [5, 10, 11]. Symptoms are usually nonspecific [14, 15]. Although pain is the most common symptom [6], edema, redness, warmth, and limitation of motion can be seen [14, 15]. Fever, malaise, anorexia, weight loss, night sweats, and tachycardia may also occur [14, 16, 17]. Patients from the Indian subcontinent predominantly have a higher prevalence of exudative disease with or without discharging sinuses and often have advanced disease at the time of presentation [13, 18]. The incidence of sinus formation is 10 to 30% [3, 19]. As a general rule, the cold abscesses and the subsequent sinuses, originating from the joint, are situated on the lateral, posterolateral or posterior aspect of the joint. On the other hand, cold abscesses and sinuses, originating from the supratrochlear lymph node, are situated on the medial aspect. One-third of the elbows (33.3%) had one or more discharging sinuses in the case series reported by Aggarwal and Dhammi [6]. A long history of symptoms, a lack of constitutional symptoms (unless multifocal), a poor response to commonly used broad-spectrum antibiotics, and non-healing ulcers may necessitate a careful workup for the presence of TB; in such cases, a cautious approach should be considered regarding joint drainage for the mistaken diagnosis of septic arthritis [1]. Aggarwal and Dhammi reported that out of 48 cases of TB elbow, 10 patients had a wrongfully performed drainage procedure for the treatment of a misdiagnosed pyogenic joint [6]. Many patients have higher erythrocyte sedimentation, but this is not diagnostic [14, 16, 17]. From a radiographical view-point, tuberculous arthritis is normally characterized by periarticular osteoporosis, peripherally located osseous erosions and gradual narrowing of the cartilage space (Phemister triad) [2, 10, 11]. However, according to Haygood and Williamson [20], there is no single pathognomonic finding that allows making the diagnosis of skeletal TB. The radiological findings are non-specific in the early stages and the initial lesions can be easily missed. Joint effusion with soft tissue edema may be one of the earliest signs of tuberculous arthritis [20]. Periarticular osteoporosis is a common manifestation of tuberculous arthritis and may be more common in the weight-bearing joints of the lower extremities than in the upper extremities. However, the detection of periarticular osteoporosis on plain radiographs is subjective [20]. Para-articular round or oval lytic lesions with poorly defined margins are common findings in extremity TB [1, 6]. In patients, with elbow TB, the proximal part of the ulna is the most common site of involvement [6] and ‘‘ice cream scoop’’ appearance of the proximal part of the ulna should prompt an investigation for TB [1]. Ultrasound shows synovial thickening with joint effusion. Computed tomography (CT) can be used to evaluate the degree of bone destruction, soft tissue extension and sequestrum formation [7]. Magnetic resonance imaging (MRI) features include bone marrow changes indicating osteomyelitis or bone marrow edema, bone erosions, synovial thickening, and joint effusion. Synovial thickening associated with osteoarticular TB is hypo intense on T2-weighted MRI images, distinguishing this from other proliferating synovial arthropathies [7]. Radiological findings in osteoarticular TB are non-specific and may require aspiration or synovial biopsy for definitive diagnosis [7]. Despite the presence of TB infection, aspiration material is not stained or reproductive [14, 15]. Microscopy and cultures of synovial fluid yield positive results in up to 80% of patients with osteoarticular TB and remainder diagnosed through synovial or bone biopsies [7]. Hence, performing a biopsy is important for diagnosis. Histology shows Caseating granulomas even when a Ziehl-Nielsen stain is negative [7]. In our present case, surgical resection of radial head along with sinus tract helped in biological clearance of the disease as well as for obtaining adequate amount of tissue for various diagnostic tools. Detection of mycobacterium TB by Cartridge Based Nucleic Acid Amplification Test (CB-NAAT), in culture and presence of tuberculoma in histopathology in surgically resected tissue proved to be diagnostic. After the diagnosis of TB, treatment should be initiated very quickly and maintained for adequate duration. In total, 90–95% of the patients will recover if treatment is started in the early period [14, 15, 17]. In cases of advanced TB, extensive loss of elbow motion may occur with residual deformity [21]. Usually, within 3 weeks after the start of antitubercular treatment, the pain subsides, and the patient can start physiotherapy [1].
Aggrawal and Dhammi reported 8 cases of concurrent proximal radius involvement out of 48 TB elbow in their series [6]. Agarwal reported 3 cases of concurrent proximal radius involvement out of 10 TB elbow in children in their series [1]. The diagnosis of TB of the elbow is generally delayed because the lesion is relatively uncommon and there is a lack of awareness among clinicians, especially in non-endemic areas [2]. TB should be considered in the diagnosis of monoarthritis in developing countries [13]. Osteoarticular TB should be suspected in patients of South Asian and African origin presenting with bony and soft tissue infective lesions [1]. Early diagnosis and treatment are possible through a combination of good history taking, clinical and radiological examination and a high degree of clinical suspicion [2]. Usually, due to the late presentation and/or delay in diagnosis, the significant osteoarticular damage is already present [2, 5]. The onset is usually insidious [5, 10, 11]. Symptoms are usually nonspecific [14, 15]. Although pain is the most common symptom [6], edema, redness, warmth, and limitation of motion can be seen [14, 15]. Fever, malaise, anorexia, weight loss, night sweats, and tachycardia may also occur [14, 16, 17]. Patients from the Indian subcontinent predominantly have a higher prevalence of exudative disease with or without discharging sinuses and often have advanced disease at the time of presentation [13, 18]. The incidence of sinus formation is 10 to 30% [3, 19]. As a general rule, the cold abscesses and the subsequent sinuses, originating from the joint, are situated on the lateral, posterolateral or posterior aspect of the joint. On the other hand, cold abscesses and sinuses, originating from the supratrochlear lymph node, are situated on the medial aspect. One-third of the elbows (33.3%) had one or more discharging sinuses in the case series reported by Aggarwal and Dhammi [6]. A long history of symptoms, a lack of constitutional symptoms (unless multifocal), a poor response to commonly used broad-spectrum antibiotics, and non-healing ulcers may necessitate a careful workup for the presence of TB; in such cases, a cautious approach should be considered regarding joint drainage for the mistaken diagnosis of septic arthritis [1]. Aggarwal and Dhammi reported that out of 48 cases of TB elbow, 10 patients had a wrongfully performed drainage procedure for the treatment of a misdiagnosed pyogenic joint [6]. Many patients have higher erythrocyte sedimentation, but this is not diagnostic [14, 16, 17]. From a radiographical view-point, tuberculous arthritis is normally characterized by periarticular osteoporosis, peripherally located osseous erosions and gradual narrowing of the cartilage space (Phemister triad) [2, 10, 11]. However, according to Haygood and Williamson [20], there is no single pathognomonic finding that allows making the diagnosis of skeletal TB. The radiological findings are non-specific in the early stages and the initial lesions can be easily missed. Joint effusion with soft tissue edema may be one of the earliest signs of tuberculous arthritis [20]. Periarticular osteoporosis is a common manifestation of tuberculous arthritis and may be more common in the weight-bearing joints of the lower extremities than in the upper extremities. However, the detection of periarticular osteoporosis on plain radiographs is subjective [20]. Para-articular round or oval lytic lesions with poorly defined margins are common findings in extremity TB [1, 6]. In patients, with elbow TB, the proximal part of the ulna is the most common site of involvement [6] and ‘‘ice cream scoop’’ appearance of the proximal part of the ulna should prompt an investigation for TB [1]. Ultrasound shows synovial thickening with joint effusion. Computed tomography (CT) can be used to evaluate the degree of bone destruction, soft tissue extension and sequestrum formation [7]. Magnetic resonance imaging (MRI) features include bone marrow changes indicating osteomyelitis or bone marrow edema, bone erosions, synovial thickening, and joint effusion. Synovial thickening associated with osteoarticular TB is hypo intense on T2-weighted MRI images, distinguishing this from other proliferating synovial arthropathies [7]. Radiological findings in osteoarticular TB are non-specific and may require aspiration or synovial biopsy for definitive diagnosis [7]. Despite the presence of TB infection, aspiration material is not stained or reproductive [14, 15]. Microscopy and cultures of synovial fluid yield positive results in up to 80% of patients with osteoarticular TB and remainder diagnosed through synovial or bone biopsies [7]. Hence, performing a biopsy is important for diagnosis. Histology shows Caseating granulomas even when a Ziehl-Nielsen stain is negative [7]. In our present case, surgical resection of radial head along with sinus tract helped in biological clearance of the disease as well as for obtaining adequate amount of tissue for various diagnostic tools. Detection of mycobacterium TB by Cartridge Based Nucleic Acid Amplification Test (CB-NAAT), in culture and presence of tuberculoma in histopathology in surgically resected tissue proved to be diagnostic. After the diagnosis of TB, treatment should be initiated very quickly and maintained for adequate duration. In total, 90–95% of the patients will recover if treatment is started in the early period [14, 15, 17]. In cases of advanced TB, extensive loss of elbow motion may occur with residual deformity [21]. Usually, within 3 weeks after the start of antitubercular treatment, the pain subsides, and the patient can start physiotherapy [1].
Conclusion
This case report highlights the clinical and radiological manifestations of rarely reported TB of isolated radial head without involvement of distal humerus and proximal ulna. Its diagnosis is often misleading and hence mismanagement may occur. Therefore, a biopsy is essential to demonstrate the presence of mycobacterium TB by CB-NAAT (Cartridge Based Nucleic Acid Amplification Test) method and in culture, and tuberculoma in histopathology to establish the diagnosis so that early appropriate treatment can be instituted.
Clinical Message
The diagnosis of TB of the elbow is generally delayed. A combination of a high index of clinical suspicion based on good history taking, clinical and radiological examination and biopsy for various tests allow early diagnosis and treatment of rarely occurring tuberculosis of isolated radial head for a painless, stable and normally functioning elbow joint.
References
1. Agarwal A. Tuberculosis of the elbow joint in children: A review of ten patients who were managed conservatively. J Bone Joint Surg Am 2010; 92:436-441.
2. Wang CT, Sun JS, Hou SM. Mycobacterial infection of the upper extremities. J Formos Med Assoc 2000; 99:710-715.
3. Chen WS, Wang CJ, Eng HL. Tuberculous arthritis of the elbow. Int Orthop 1997; 21:367-370.
4. Martini M, Benkeddache Y, Medjani Y, Gottesman H. Tuberculosis of the upper limb joints. Int Orthop 1986; 10:17-23.
5. Tuli SM. Tuberculosis of the Skeletal System. 2nd ed. Delhi: Jaypee Brothers Medical Publishers; 1997. p. 132-140.
6. Aggarwal A, Dhammi I. Clinical and radiological presentation of tuberculosis of the elbow. Acta Orthop Belg 2006; 72:282-287.
7. Vishwanath T Thimmaiah, Deepashree. Unusual presentation of tuberculosis of elbow joint: A case report. Res Rev J Med Health Sci 2013; 2(4): 17-20.
8. Dix-Peek SI, Vrettos BC, Hoffman EB. Tuberculosis of the elbow in children. J Shoulder Elbow Surg 2003; 12:282-286.
9. Terry S, Canale JH. Campbell’s Operative Orthopaedics. 12th ed. Memphis: Elsevier; 2013.
10. Domingo A, Nomdedeu M, Tomás X, García S. Elbow tuberculosis: An unusual location and diagnostic problem. Arch Orthop Trauma Surg 2005; 125:56-58.
11. George JC, Buckwalter KA, Braunstein EM. Case report 824: Tuberculosis presenting as a soft tissue forearm mass in a patient with a negative tuberculin skin test. Skeletal Radiol 1994; 23:79-81.
12. Sdillon Aea M. Tuberculosis of elbow A clinicoradiological correlation. Indian J Orthop 2012; 46:200-205.
13. Yazici A, Kayan G, Yaylaci S, Demir MV, Karakeçe E, Tamer A*, et al. Tuberculous arthritis of the elbow joint: A case report. Case report. Eur J Rheumatol 2016; 3:142-143.
14. Erdem H, Baylan O, Simsek I, Dinc A, Pay S, Kocaoglu M, et al. Delayed diagnosis of tuberculous arthritis. Jpn J Infect Dis 2005; 58:373-375.
15. Tuli SM. General principles of osteoarticular tuberculosis. Clin Orthop Relat Res 2002; 398:11-9.
16. Jung SS, Lee MK, Lim SH, Kwon YM, Choi SS. Elbow pain proven to be tuberculous arthritis -A case report-. Korean J Anesthesiol 2010; 58:211-214.
17. Sagoo RS, Lakdawala A, Subbu R. Tuberculosis of the elbow joint. JRSM Short Rep 2011; 2:17.
18. Gupta SK. The treatment of synovial tuberculosis of the knee by a method with unrestricted activities. Ind J Orthop 1962; 16:14-18.
19. Haygood TM, Williamson SL. Radiographic findings of extremity tuberculosis in childhood: Back to the future? Radiographics 1994; 14:561-570.
20. Ludwig B. Musculoskeletal tuberculosis. Dis Mon 2007; 53:39-45.
21. Vohra R, Kang HS. Tuberculosis of the elbow. A report of 10 cases. Acta Orthop Scand 1995; 66:57-58.
 |
 |
 |
 |
| Dr. Naba Pallab Chetia | Dr. Aritra Bidyananda | Dr. Manabjyoti Talukdar | Dr. Munin Borgohain |
| How to Cite This Article: Chetia N P, Bidyananda A, Talukdar M, Borgohain M. A Case Report of Tuberculosis of Isolated Radial Head – A Rare Location with Diagnostic Dilemma. Journal of Orthopaedic Case Reports 2018. May- June; 8(3):28-32. |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Case Report of Post-Traumatic Monoarticular Tuberculosis of the Knee in a Healthy Young Adult: Diagnostic and Therapeutic Challenges in a Non-Endemic Setting
February 1, 2026 Case Report of Post-Traumatic Monoarticular Tuberculosis of the Knee in a Healthy Young Adult: Diagnostic and Therapeutic Challenges in a Non-Endemic Setting May 1, 2025 A Rare Case of Shoulder Tuberculosis Managed with Anti-tuberculosis Treatment and Antibiotic Coated Cement Spacer
May 1, 2025 A Rare Case of Shoulder Tuberculosis Managed with Anti-tuberculosis Treatment and Antibiotic Coated Cement Spacer May 1, 2025 Burkholderia pseudomallei-induced Oligoarticular Septic Arthritis Masquerading as Tuberculosis in a Non-Diabetic Host from Northern Kerala
May 1, 2025 Burkholderia pseudomallei-induced Oligoarticular Septic Arthritis Masquerading as Tuberculosis in a Non-Diabetic Host from Northern Kerala March 1, 2025 Tubercular Synovitis of Knee presenting with Diabetic Ketoacidosis in a patient with multiple comorbidities
March 1, 2025 Tubercular Synovitis of Knee presenting with Diabetic Ketoacidosis in a patient with multiple comorbidities