
[box type=”bio”] Learning Point for the Article: [/box]
It is important for surgeons to be aware of the different variations of the proximal attachment of the long head of the biceps tendon, including the trifurcate origin.
Case Report | Volume 8 | Issue 4 | JOCR July – August 2018 | Page 70-73| Holt S Cutler, Matthew A Tao, Stephen J O’Brien, Samuel A Taylor. DOI: 10.13107/jocr.2250-0685.1166
Authors: Holt S Cutler1, Matthew A Tao2, Stephen J O’Brien2, Samuel A Taylor2
[1]Department of Orthopaedic Surgery, UT Southwestern Medical Center, 5200 Harry Hines Boulevard, Dallas, 75235, Texas, USA.
[2]Department of Orthopaedic Surgery, the Sports Medicine and Shoulder Service, Hospital for Special Surgery, 535 East 70th Street, New York, 10021, USA.
Address of Correspondence:
Dr. Samuel A Taylor,
Department of Orthopaedic Surgery, the Sports Medicine and Shoulder Service, Hospital for Special Surgery, 535 East 70th Street, New York 10021, USA.
E-mail: SamuelTaylor.MD@gmail.com
Abstract
Introduction: Variant anatomy of the intra-articular portion of the long head of the biceps tendon (LHBT) is rare, and its clinical significance is poorly understood. However, these variants are encountered with increasing frequency due to increasing use of shoulder arthroscopy.
Case Report: We report a case of a trifurcate intra-articular LHBT, a variation which, to our knowledge, has not been previously described. The patient was an adult male presenting with chronic atraumatic shoulder pain that worsened with overhead activity. On arthroscopy, the LHBT was found to have three origins from the (1) supraspinatus tendon, (2) superior labrum, and (3) rotator interval that joined together distally within the biceps tunnel. We believe the split tendon may have caused impingement the biceps tunnel; therefore, the patient was treated with subpectoral tenodesis. He also underwent subacromial decompression and rotator cuff debridement.
Conclusion: This case highlights the importance of surgeon and radiologist awareness of split LHBT variant anatomy, such that misdiagnosis and unnecessary treatment may be avoided.
Keywords: Shoulder, biceps tendon, arthroscopy, variant anatomy.
Introduction
Variant anatomy of the biceps brachii has been described in case reports and anatomy atlases [1, 2, 3, 4, 5]. While supernumerary heads of the biceps arising from extra-articular locations appear to be the most commonly observed variation [2, 3], intra-articular variants are of particular interest in the current era of shoulder arthroscopy [6, 7, 8, 9, 10, 11]. Recent classifications have been proposed for variant anatomy of the intra-articular portion of the long head of the biceps tendon (LHBT) [7], and hypotheses linking these variations to disrupted stages of embryological development have been cited as possible etiologies [12]. Intra-articular variants of the LHBT are relatively rare with a frequency of 1.9% in a large series of shoulder arthroscopies [7]. The clinical significance of these variants and their impact on pre-operative and intraoperative decision-making remains largely unclear. The purpose of this study is to describe a case of a trifurcate intra-articular origin of the LHBT encountered during shoulder arthroscopy and to discuss its impact on diagnosis and treatment of a patient with shoulder pain.
Case Report
A 42 year-old, right hand dominant male presented with 10 years of atraumatic right shoulder pain, exacerbated by overhead activity and weightlifting. He denied any history of trauma or instability. Physical examination revealed no gross deformities and no tenderness at the acromioclavicular joint or along the bicipital tunnel. Internal rotation was slightly limited compared to his contralateral side. The rotator cuff (RC) demonstrated mild weakness and was easily fatigued. Neer and Hawkins impingement tests were markedly positive. The active compression test (O’Brien Sign) was also positive as indicated by reproduction of the patient’s symptoms – pain deep within the glenohumeral joint – during phase one (thumb down) that were alleviated in phase two (thumb up). Cross-body adduction, speeds, and Yergason tests were all negative, and there was no evidence of shoulder instability. Magnetic resonance imaging demonstrated a partial-thickness articular-sided tearing of the supraspinatus (SS) and degenerative labrum tearing The biceps tendon was noted to have an accessory slip originating from the anterior aspect of the SS.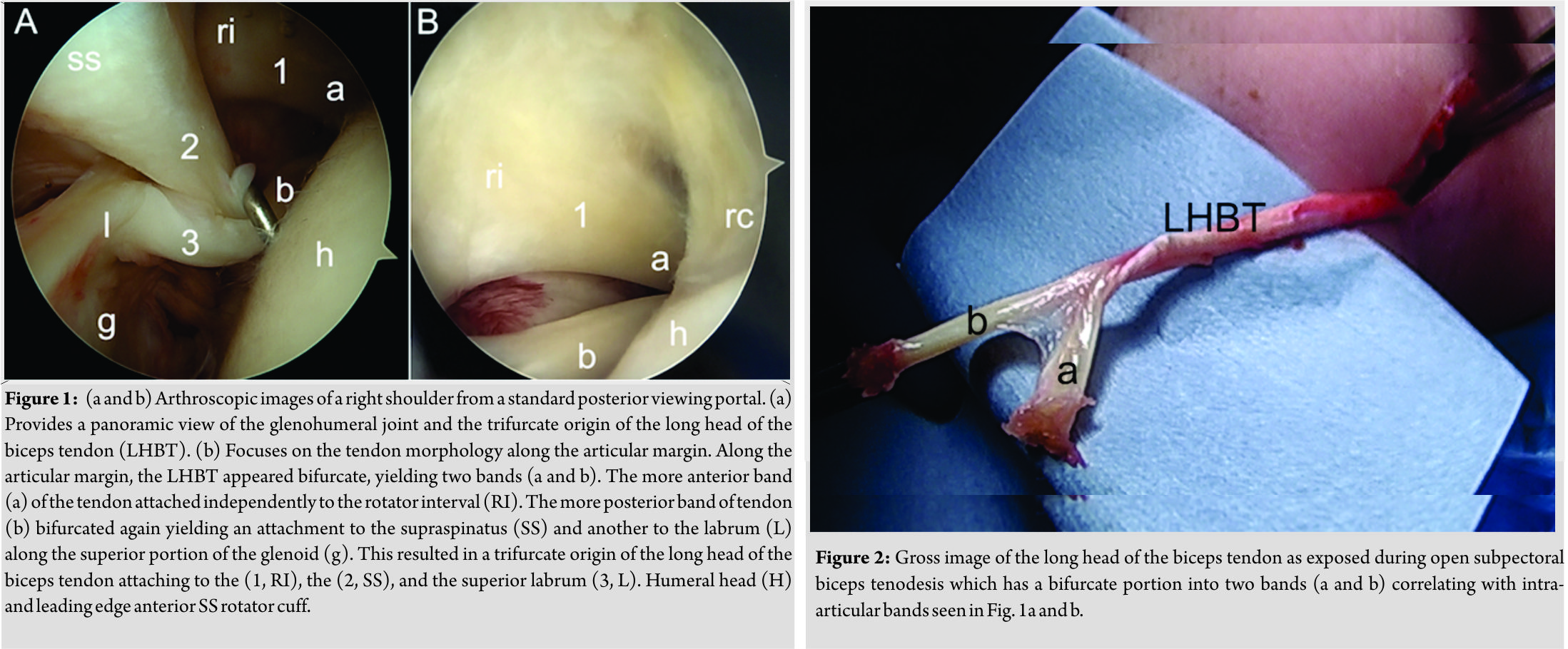 Conservative efforts including oral anti-inflammatories, activity modification, corticosteroid injection, and physical therapy failed to provide longstanding relief. The patient elected to undergo definitive surgical intervention to include labral debridement, subacromial decompression, and biceps tenodesis. During diagnostic arthroscopy, the origin of the LHBT was found to be trifurcate, with origins arising from the SS tendon, superior labrum, and rotator interval (RI). At the articular margin, the LHBT was bifurcate (Fig. 1a). The more anterior of these two structures (2.8 cm) attached to the RI with its fibers blending such that the tendon was grossly indistinguishable from the interval tissue itself and separate from the leading edge of the SS. The more posterior bifurcate portion of the LHBT (3.8 cm) itself bifurcated with one portion attaching directly to the undersurface of the SS, while the remaining band attached to the superior labrum/supraglenoid tubercle (Fig. 1b). No fraying or gross inflammatory changes of the LHBT were appreciated (Fig 2). Tenotomy of all three origins was carried out using a radiofrequency ablation wand with care to avoid damaging either the SS or the RI tissue. Subpectoral biceps tenodesis was selected for definitive management to enable fixation of a single tendon. Postoperatively, the patient was started on early range of motion with limitations of active elbow flexion to less than 1 pound for the first 6 weeks followed by progressive strengthening. By 3 months postoperatively, the patient maintained normal biceps contour, regained full shoulder motion, and was progressing his activities without limitation.
Conservative efforts including oral anti-inflammatories, activity modification, corticosteroid injection, and physical therapy failed to provide longstanding relief. The patient elected to undergo definitive surgical intervention to include labral debridement, subacromial decompression, and biceps tenodesis. During diagnostic arthroscopy, the origin of the LHBT was found to be trifurcate, with origins arising from the SS tendon, superior labrum, and rotator interval (RI). At the articular margin, the LHBT was bifurcate (Fig. 1a). The more anterior of these two structures (2.8 cm) attached to the RI with its fibers blending such that the tendon was grossly indistinguishable from the interval tissue itself and separate from the leading edge of the SS. The more posterior bifurcate portion of the LHBT (3.8 cm) itself bifurcated with one portion attaching directly to the undersurface of the SS, while the remaining band attached to the superior labrum/supraglenoid tubercle (Fig. 1b). No fraying or gross inflammatory changes of the LHBT were appreciated (Fig 2). Tenotomy of all three origins was carried out using a radiofrequency ablation wand with care to avoid damaging either the SS or the RI tissue. Subpectoral biceps tenodesis was selected for definitive management to enable fixation of a single tendon. Postoperatively, the patient was started on early range of motion with limitations of active elbow flexion to less than 1 pound for the first 6 weeks followed by progressive strengthening. By 3 months postoperatively, the patient maintained normal biceps contour, regained full shoulder motion, and was progressing his activities without limitation.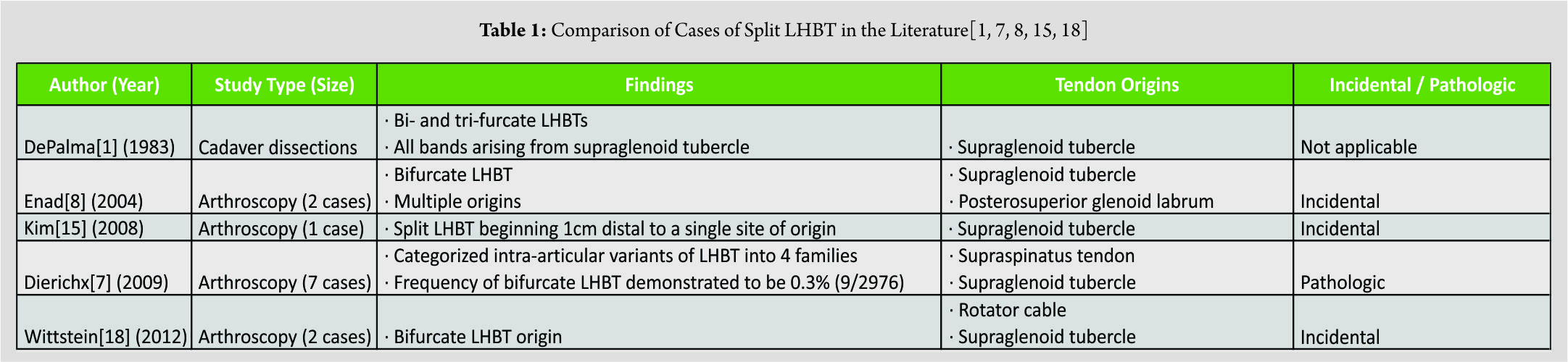
Discussion
To our knowledge, this is the first report of a trifurcate intra-articular origin of the LHBT. Variant origins of the LHBT have been described from the superior labrum, SS, and RI previously yet never simultaneously in a patient. We believe the variant encountered was a congenital anomaly as there was no significant fraying or inflammatory changes of the tendon to suggest either of the accessory bands resulted from scar formation from prior trauma or adhesive capsulitis. Additionally, these alternative scenarios were not consistent with the patient’s history. As utilization of shoulder arthroscopy increases, awareness of aberrant anatomy is important to help surgeons and radiologists avoid misdiagnosis and unnecessary treatment. Anatomic variants of the biceps brachii have been described previously in cadaveric studies [1, 2, 3, 13, 14] and increasingly in the arthroscopic [4, 7, 8, 9, 12, 15, 16, 17, 18] and radiology literature [19, 20]. Greig et al. observed variant anatomy of the biceps brachii in 22% of cadaver specimens with an accessory extra-articular heads of the biceps being most common (14%) [3]. Intra-articular variants appear to be far less common. Dierickx et al. showed their frequency to be 1.9% in a large series of nearly 3000 shoulder arthroscopies [7]. In the normal adult shoulder, the LHBT originates from the supraglenoid tubercle and posterosuperior labrum [13, 14] as a single tendon and traverses through the RI as a free intra-articular structure before descending into the biceps tunnel. Historically, it was thought that during embryologic development the LHBT migrated from an extra-articular location along the coracoid to its free intra-articular location in the adult shoulder based on comparative anatomy studies by Welcker [21]. However, more recent embryological evidence indicates that the LHBT lies between the fibrotic capsule and synovial layer in its earliest form before migrating to a free intra-articular position by approximately 20 weeks of gestation [12, 22, 23, 24, 25]. Rarely, arthroscopic case reports have observed the LHBT to be absent [7], embedded in the capsule [4, 7, 12], or loosely connected to the capsule by a mesotenon [7]. Combining embryologic and arthroscopic observations, Audenaert et al. theorized that these congenital abnormalities represent disruptions in the progressive migration of the LHBT during development[12]. Descriptions of split or bifurcate LHBTs are fewer in number, and no theories have been proposed to explain their embryological development (Table 1). De Palma first described a split LHBT in cadaver dissections [1]. Two or three distinct bands of the LHBT were seen originating from the supraglenoid tubercle. In contrast, the trifurcate LHBT origin represented in this case had three distinct sites of origin at the superior labrum, SS, and RI. Enad first described a bifurcate LHBT in an arthroscopic case [8], and other similar reports have appeared since [7, 18]. Split LHBTs with a single site of origin are also described [15]. The best estimate of the frequency of bifurcate LHBTs is 0.3% in Dierickx’s study of 2976 shoulder arthroscopies [7]. The significance of these variants is unclear, and there is no agreement within the literature as to whether these variants are pathologic or incidental findings, a determination that is likely case-specific. One of the bifurcations in our case was more distal than those previously reported, introducing the possibility of impingement within the biceps tunnel. Our study is limited by the sample size of one patient. Additionally, the possibility that the anatomic variant described resulted from trauma rather than a congenital abnormality cannot be excluded. As the patient also underwent subacromial decompression and RC debridement, we cannot assuredly say this anatomic variation contributed to his clinical symptoms.
Conclusion
Intra-articular variants of the LHBT are rare but increasingly encountered as greater numbers of shoulder arthroscopies are performed. The case presented here is the first report of a trifurcate LHBT encountered arthroscopically. The case highlights the importance of surgeon and radiologist awareness of anatomical variants of the intra-articular portion of the LHBT in order to avoid misdiagnosis and unnecessary treatment.
Clinical Message
It is important for surgeons to be aware of the different variations of the proximal attachment of the long head of the biceps tendon, including the trifurcate origin.
References
1. De Palma AF. Surgery of the Shoulder. 3rd ed. Philadelphia: JB Lippincott; 1983. p. 33-53.
2. Bergman RA, Thompson SA, Afifi AK, Saadeh FA. Compendium of Human Anatomic Variation. Baltimore, MD: Urban and Schwarzenberg; 1988. p. 11, 279.
3. Greig HW, Anson BJ, Budinger JM. Variations in the form and attachments of the biceps brachii muscle. Q Bull Northwest Univ Med Sch 1952;26:241-4.
4. Hyman JL, Warren RF. Extra-articular origin of Biceps brachii. Arthroscopy 2001;17:E29.
5. Warner JJ, McMahon PJ. The role of the long head of the biceps brachii in superior stability of the glenohumeral joint. J Bone Joint Surg Am Vol 1995;77:366-72.
6. Andreoli CV, Esteves LR, Figueiredo E, Belangero PS, de Castro Pochini A, Ejnisman B. Tendon of the long head of the biceps originating from the rotator cuff – An uncommon anatomical variation: case report. Rev Bras Ortop 2016;51:96-9.
7. Dierickx C, Ceccarelli E, Conti M, Vanlommel J, Castagna A. Variations of the intra-articular portion of the long head of the biceps tendon: A classification of embryologically explained variations. J Shoulder Elbow Surg 2009;18:556-65.
8. Enad JG. Bifurcate origin of the long head of the biceps tendon. Arthroscopy 2004;20:1081-3.
9. Ghalayini SR, Board TN, Srinivasan MS. Anatomic variations in the long head of biceps: Contribution to shoulder dysfunction. Arthroscopy 2007;23:1012-8.
10. Jeong JY, Park SM, Park YE, Yoo JC. Morphological classification of anatomical variants of the intra-articular portion of the long head of the biceps brachii tendon and analysis of the incidence and the relationship with shoulder disease for each subtype. J Orthop Surg (Hong Kong) 2017;25:2309499017742207.
11. Morris D, Guettler J, Morris S. Bilateral superior labrum anterior to posterior (SLAP) tears with abnormal anatomy of biceps tendon. Am J Orthop (Belle Mead NJ) 2015;44:E275-7.
12. Audenaert EA, Barbaix EJ, Van Hoonacker P, Berghs BM. Extraarticular variants of the long head of the biceps brachii: A reminder of embryology. J Shoulder Elbow Surg 2008;17:114S-7S.
13. Pal GP, Bhatt RH, Patel VS. Relationship between the tendon of the long head of biceps brachii and the glenoidal labrum in humans. Anat Rec 1991;229:278-80.
14. Vangsness CT Jr., Jorgenson SS, Watson T, Johnson DL. The origin of the long head of the biceps from the scapula and glenoid labrum. An anatomical study of 100 shoulders. J Bone Joint Surg Br Vol 1994;76:951-4.
15. Kim KC, Rhee KJ, Shin HD, Kim YM. Biceps long head tendon revisited: A case report of split tendon arising from single origin. Arch Orthop Trauma Surg 2008;128:495-8.
16. Lang JE, Vinson EN, Basamania CJ. Anomalous biceps tendon insertion into the rotator cable: A case report. J Surg Orthop Adv 2008;17:93-5.
17. Richards DP, Schwartz M. Anomalous intraarticular origin of the long head of biceps brachii. Clin J Sport Med Off J Can Acad Sport Med 2003;13:122-4.
18. Wittstein J, Lassiter T Jr., Taylor D. Aberrant origin of the long head of the biceps: A case series. J Shoulder Elbow Surg 2012;21:356-60.
19. Gaskin CM, Golish SR, Blount KJ, Diduch DR. Anomalies of the long head of the biceps brachii tendon: Clinical significance, MR arthrographic findings, and arthroscopic correlation in two patients. Skeletal Radiol 2007;36:785-9.
20. Yeh L, Pedowitz R, Kwak S, Haghighi P, Muhle C, Trudell D, et al. Intracapsular origin of the long head of the biceps tendon. Skeletal Radiol 1999;28:178-81.
21. Welcker H. Die einwanderung der bicepssehne in das schultergelenk. nebst notizen uber ligamentum interarticulare humeri und ligamentum teres femoris. Arch Anat Physiol 1878;1:20-42.
22. Fealy S, Rodeo SA, Dicarlo EF, O’Brien SJ. The developmental anatomy of the neonatal glenohumeral joint. J Shoulder Elbow Surg 2000;9:217-22.
23. Gardner E, Gray DJ. Prenatal development of the human shoulder and acromioclavicular joints. Am J Anat 1953;92:219-76.
24. Tena-Arregui J, Barrio-Asensio C, Viejo-Tirado F, Puerta-Fonolla J, Murillo-Gonzalez J. Arthroscopic study of the knee joint in fetuses. Arthroscopy 2003;19:862-8.
25. Neale RM. The alleged transmigration of the long tendon of the biceps brachii. Anat Rec 1937;67:205-18.
 |
 |
 |
 |
| Dr. Holt S Cutler | Dr. Matthew A Tao | Dr. Stephen J O’Brien | Dr. Samuel A Taylor |
| How to Cite This Article: Cutler H S, Tao M A, O’Brien S J, Taylor S A. Trifurcate Origin of Long Head of Biceps Brachii: A Case Report and Literature Review. Journal of Orthopaedic Case Reports 2018 Jul-Aug; 8(4): 70-73 |
[Full Text HTML] [Full Text PDF] [XML]
[rate_this_page]
Dear Reader, We are very excited about New Features in JOCR. Please do let us know what you think by Clicking on the Sliding “Feedback Form” button on the <<< left of the page or sending a mail to us at editor.jocr@gmail.com
Related Articles in Journal of Orthopaedic Case Reports
 November 10, 2019 Arthroscopic Treatment ofPrimary Synovial Chondromatosis of the Subscapular Bursa: A Case Report
November 10, 2019 Arthroscopic Treatment ofPrimary Synovial Chondromatosis of the Subscapular Bursa: A Case Report May 10, 2019 Arthroscopic Repair of an Isolated Infraspinatus Tear in a Contact Athlete: A Case Report
May 10, 2019 Arthroscopic Repair of an Isolated Infraspinatus Tear in a Contact Athlete: A Case Report March 10, 2017 Intra-articular Loose Body with Concomitant Bankart Lesion after a Traumatic Shoulder Dislocation: A Case Report Jason B T Lim1, Andrew H C Tan1
March 10, 2017 Intra-articular Loose Body with Concomitant Bankart Lesion after a Traumatic Shoulder Dislocation: A Case Report Jason B T Lim1, Andrew H C Tan1 November 1, 2025 Outcome of Non-thumb Metacarpal Shaft Fractures Treated by Two Different Techniques – K Wire and Herbert Screw Fixation: A Comparative Single Centre Study
November 1, 2025 Outcome of Non-thumb Metacarpal Shaft Fractures Treated by Two Different Techniques – K Wire and Herbert Screw Fixation: A Comparative Single Centre Study