
Single stage surgery for the lateral femoral condyle fracture after anterior cruciate ligament reconstruction to manage both fracture and graft should be kept in mind.
Dr. Pushpak Kumar,
Department of Orthopaedics,
Rural Medical College, Pravara Medical Trust,
Loni, Maharashtra, India.
E-mail: dr.pushpak.kumar@gmail.com
Abstract
Introduction: Anterior cruciate ligament (ACL) reconstruction using hamstring tendon graft is a commonly performed orthopedic surgery. Lateral femoral condyle fracture through the femoral tunnel is a rare complication following ACL reconstruction. These cases are reported to be managed in two stages, fracture fixation by open reduction and internal fixation with bone grafting of the femoral tunnel, followed by revision ACL reconstruction after the fracture union.
Case Report: A 41-year-old male Kabaddi player underwent right knee arthroscopic ACL reconstruction following an ACL tear in January 2021, sustained a road traffic accident 7 weeks later and developed a lateral femoral condyle fracture. The graft was intact and trapped into the fracture site making fracture reduction difficult. The graft was lax due to the fixed loop button being trapped in the fracture. The patient was treated in a single stage by arthroscopy assisted fracture reduction and fixation with ACL graft salvage and reinforced suspensory femoral graft fixation to plate suspensory fixation.
Conclusion: This case is a rare presentation of lateral condyle fracture after ACL reconstruction and both the issues are managed in a single stage with the help of detailed surgical planning, using utmost arthroscopy skills and keeping all the options of fixation devices ready on the table during the surgery.
Keywords: Anterior cruciate ligament, anterior cruciate ligament reconstruction, lateral femoral condyle fracture.
Anterior cruciate ligament (ACL) reconstruction is a commonly performed orthopedic surgery. Quadrupled hamstring tendon (HT) is the most widely used autograft option [1]. The common complications of this surgery are anterior knee pain, stiffness, secondary meniscal lesions, ACL re-rupture, infections, and thromboembolic complications, and peri-articular fracture [2]. Peri-articular fractures are an uncommon but devastating complication following ACL reconstruction. Fractures of the patella [3], tibial plateau [4], tibial tubercle [5], supra-condylar femur [6,7], medial femoral condyle [8], and and lateral femoral condyle [9,10,11,12,13] have been reported after primary and revision ACL reconstruction. Lateral femoral condyle fracture through the femoral tunnel is a rare but reported complication following both primary and revision ACL reconstruction at varied postoperative intervals. The femoral tunnel can act as a stress riser facilitating the fracture more so in revision ACL reconstructions [11] and after months to years of primary ACL reconstruction [13]. These cases have been reported to be managed in two stages, fracture fixation by open reduction and internal fixation with bone grafting of the femoral tunnel, followed by revision ACL reconstruction after the fracture union [12]. We report a unique case of lateral femoral condyle fracture involving the femur tunnel, 7 weeks after primary arthroscopic ACL reconstruction which was managed in single-stage by arthroscopy assisted reduction and internal fixation of fracture and ACL graft salvage with reinforcement of cortical suspensory femoral fixation.
A 41-year-old male, Kabaddi player, presented to Pravara Rural Hospital, Loni in January 2021 with right knee instability of 6 months duration, positive Lachman test, complete ACL tear and medial meniscus posterior horn Grade III tear on magnetic resonance imaging (MRI). He was treated with arthroscopic ACL reconstruction using semitendinosus and gracilis (HT) graft fixed with 15 mm closed-loop button on the femur and 25 mm × 8 mm titanium screw on the tibia and medial meniscus balancing. Post-operative radiographs confirmed well-fixed button and good tunnel positions (Fig. 1). The patient was started on knee rehabilitation, closed chain exercises, and full weight-bearing.
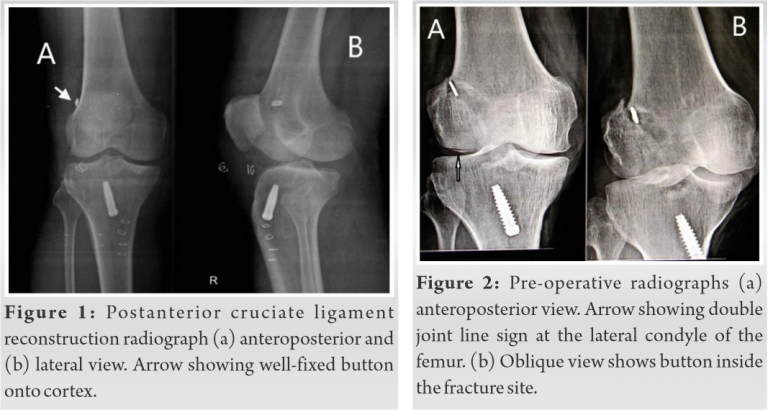
Two months after the surgery, the patient met with a road traffic accident and fell from a moving motorcycle with twisting injury to the same knee. The patient presented to us 7 days later with severe pain, even on slight movement, moderate effusion in the right knee with an inability to bear weight. Lachman and varus and values stress test were positive. An anteroposterior radiograph revealed a double joint line sign of lateral femoral condyle with the button sunk inside the lateral femoral cortex. Oblique radiograph confirmed a fracture passing through the femur tunnel with the button inside the fracture (Fig. 2). MRI showed a spiral displaced fracture of the lateral femoral condyle (Fig. 3), intact but lax graft fibers, and a button artifact inside the fracture line with intact medial collateral ligament and lateral collateral ligament (Fig. 4).
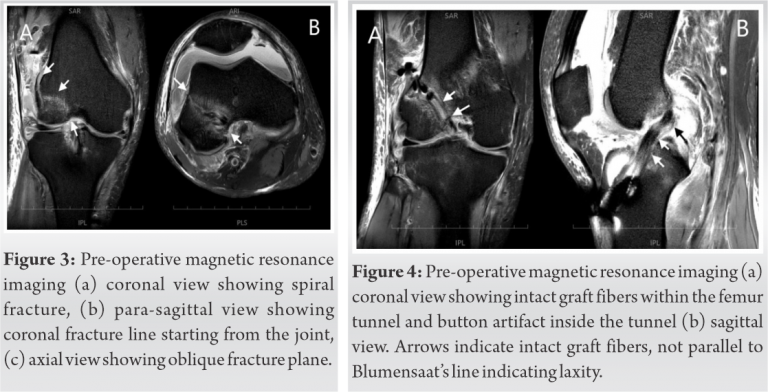
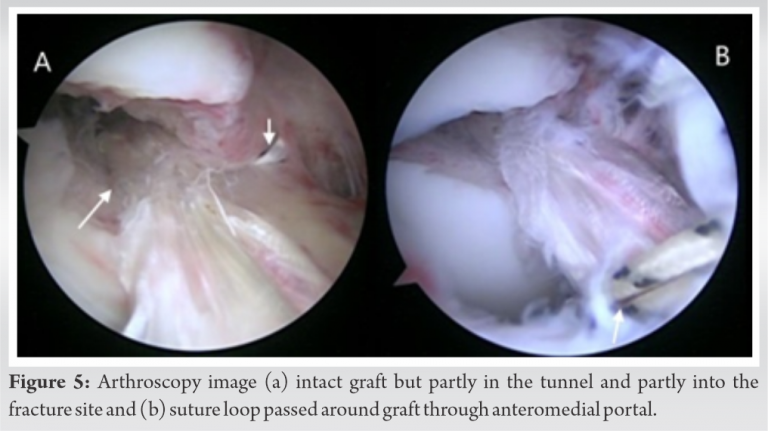
Arthroscopy assisted fracture reduction and internal fixation with an assessment of graft and possible salvage were planned. Arthroscopy revealed an intra-articular spiral fracture of the lateral femoral condyle involving the femur tunnel with intact graft fibers trapped into the fracture site making the fracture reduction difficult. The fracture plane was coronal distally inside the joint (as seen in arthroscopy) then attended para-sagittal orientation as it exited at the lateral cortex (seen after exposure of lateral condyle later). Trapped fibers of graft hindering the reduction of the fracture were pulled by a suture loop passed around the graft introduced through the anteromedial portal (Fig. 5).
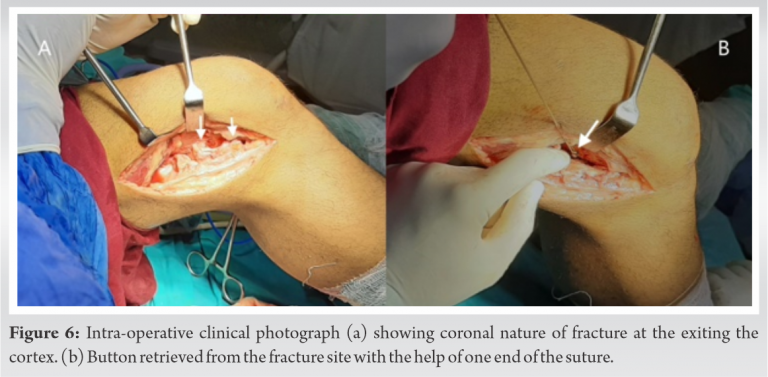
A lateral longitudinal incision was made over the lateral distal femur centered on the supracondylar ridge. Careful dissection was done to expose the lateral end of the fractured femoral tunnel. The fixed loop button attached to the graft was pulled out laterally from the fracture site (Fig. 6). The fixed loop was seen through the fracture site and was intact with graft looping into it. Two sutures were passed through the two outer holes of the button (end sutures). These two end sutures above and Tigerwire (Arthrex, Inc, Naples, Florida) looping the graft below through the anteromedial portal were pulled simultaneously by two assistants. This was done to (a) keep the button over the cortex and (b) keep the graft in tension, to keep it reduced into the femur tunnel, out of fracture site (as seen by the arthroscope).
Then internal fixation with an anteroposterior cannulated cancellous screw was done. Fracture reduction was confirmed by arthroscopy as well as fluoroscopy (Fig. 7). In addition, a 4 hole 3.5 low contact dynamic compression plate (DCP) was contoured and placed on the posterolateral ridge of lateral femoral condyle over the button, with the two end suture of the button, kept one on each side of the plate. The plate was perpendicular to the fracture line buttress the fracture and fixed with screws. Screws are passed in a way avoiding the femur tunnel.
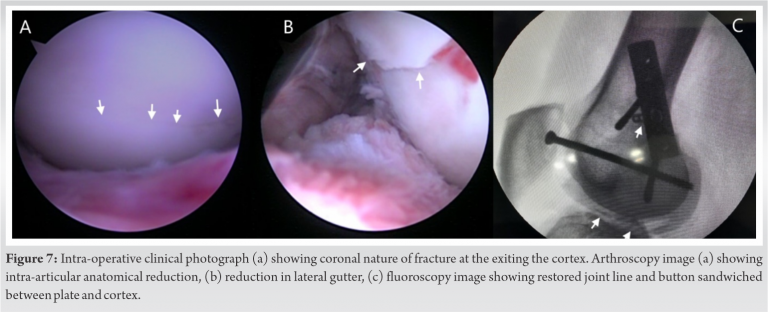
After fracture fixation, the ACL graft was found to be intact and stable on probing. The button end sutures were pulled, tensioned to make the button horizontal, and sandwiched between the plate and the lateral femoral cortex. The button end sutures were then tied over the plate, creating an additional reinforced suspensory femoral fixation of the graft with the plate.
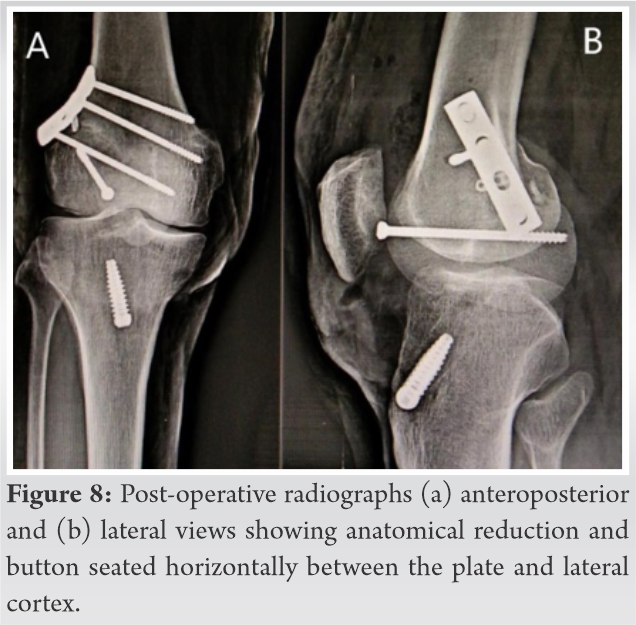
Post-operative radiographs revealed anatomic reduction and fixation of the fracture with a properly placed interference screw and button on plate suspension (Fig. 8). Postoperatively, the patient was started on knee range of motion (heel slides), static quadriceps, and straight leg raising exercises (Fig. 9). The patient was kept non-weight bearing for 6 weeks.

Lateral femoral condylar fracture after arthroscopic ACL reconstruction is a rare occurrence. A review of the literature indicates that most cases occur due to trauma along with possible stress riser at the femoral tunnel; that too after either revision ACL reconstruction or a long time after primary ACL reconstruction due to tunnel widening. This is a unique case where the patient had a high energy trauma (twisting) to the right knee 7 weeks after primary ACL reconstruction leading to a lateral condyle fracture through the femoral tunnel stress riser. The femoral stress riser is increased by sub-optimal tunnel positions, larger tunnel size, and different graft fixation methods [14]. Our patient had an optimally oriented femoral tunnel which was 8 mm in diameter and placed with an intact 2 mm of the posterior femoral cortex. Tunnel wall integrity was checked using the tunnel view test. Our patient presented with a lateral femoral condyle fracture 7 weeks after a primary ACL reconstruction. This is an uncommon presentation as most reported cases were after revision ACL reconstruction or with delayed presentation of primary ACL reconstruction due to tunnel widening. All these cases reported were managed with open reduction and internal fixation of the fracture with or without revision ACL reconstruction. This was a unique case with (a) spiral fracture of lateral femoral condyle passing through femoral tunnel, (b) non-integration of graft in the tunnel (7 weeks post-ACL reconstruction), (c) lax but intact graft fibers, (d) graft fibers trapped in the fracture site making fracture reduction difficult, and (e) intact fixed loop button but trapped into the fracture (compromised femoral fixation). The surgical plan was (a) anatomical reduction and stable internal fixation of the fracture (arthroscopy assisted or open), (b) preservation of the graft fibers by reducing them from fracture site back to femoral tunnel, arthroscopically, (c) re-tensioning and reinforcement of the femoral fixation of the graft, and (d) preferably in a single stage if possible. We managed to do everything in a single stage surgery. Closed loop button fixation of primary ACL reconstruction was reinforced with the loop button tied over the DCP in tension creating an additional plate suspensory fixation.
This case is a rare presentation of lateral condyle fracture after ACL reconstruction and both the issues are managed in single stage with the help of detailed surgical planning, using utmost arthroscopy skills and keeping all the options of fixation devices ready on table during the surgery.
Single stage surgery for the lateral femoral condyle fracture after ACL reconstruction to manage both fracture and graft is always to be kept in mind. For this detailed surgical planning and good arthroscopy skills are required; options of fixation devices should be ready on table during the surgery.
References
- 1.Cerulli G, Placella G, Sebastiani E, Tei MM, Speziali A, Manfreda F. ACL reconstruction: Choosing the graft. Joints 2013;1:18-24. [Google Scholar | PubMed]
- 2.Rousseau R, Labruyere C, Kajetanek C, Deschamps O, Makridis KG, Djian P. Complications after anterior cruciate ligament reconstruction and their relation to the type of graft: A prospective study of 958 cases. Am J Sports Med 2019;47:2543-9. [Google Scholar | PubMed]
- 3.Stein DA, Hunt SA, Rosen JE, Sherman OH. The incidence and outcome of patella fractures after anterior cruciate ligament reconstruction. Arthroscopy 2002;18:578-83. [Google Scholar | PubMed]
- 4.Moen KY, Boynton MD, Raasch WG. Fracture of the proximal tibia after anterior cruciate ligament reconstruction: A case report. Am J Orthop 1998;27:629-30. [Google Scholar | PubMed]
- 5.Acton KJ, Dowd GS. Fracture of the tibial tubercle following anterior cruciate ligament reconstruction. Knee 2002;9:157-9. [Google Scholar | PubMed]
- 6.Mithoefer K, Gill TJ, Vrahas MS. Supracondylar femoral fracture after arthroscopic reconstruction of the anterior cruciate ligament. A case report. J Bone Joint Surg Am 2005;87:1591-6. [Google Scholar | PubMed]
- 7.Noah J, Sherman OH, Roberts C. Fractures of the supracondylar femur after anterior cruciate ligament reconstruction using patellar tendon and iliotibial band tenodesis. A case report. Am J Sports Med 1992;20:615-8. [Google Scholar | PubMed]
- 8.Montgomery CO, Evans RP. Arthroscopic reduction and internal fixation of a medial femoral condylar fracture after anterior cruciate ligament reconstruction. A case report. J Bone Joint Surg Am 2008;90:863-8. [Google Scholar | PubMed]
- 9.Ternes JP, Blasier RB, Alexander AH. Fracture of the femur after anterior cruciate ligament reconstruction with a GORE-TEX prosthetic graft. A case report. Am J Sports Med 1993;21:147-9. [Google Scholar | PubMed]
- 10.Berg EE. Lateral femoral condyle fracture after endoscopic anterior cruciate ligament reconstruction. Arthroscopy 1994;10:693-5. [Google Scholar | PubMed]
- 11.Coobs BR, Spiridonov SI, LaPrade RF. Intra-articular lateral femoral condyle fracture following an ACL revision reconstruction. Knee Surg Sports Traumatol Arthrosc 2010;18:1290-3. [Google Scholar | PubMed]
- 12.Keyhani S, Vaziri AS, Shafiei H, Mardani-Kivi M. Femoral condyle fracture during revision of anterior cruciate ligament reconstruction: Case report and a review of literature. Arch Bone Jt Surg 2015;3:137-40. [Google Scholar | PubMed]
- 13.Julien TP, Ramappa AJ, Rodriguez EK. Femoral condylar fracture through a femoral tunnel eleven years after anterior cruciate ligament reconstruction: A case report. J Bone Joint Surg Am 2010;92:963-7. [Google Scholar | PubMed]
- 14.Wilson TC, Kantaras A, Atay A, Johnson DL. Tunnel enlargement after anterior cruciate ligament surgery. Am J Sports Med 2004;32:543-9. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 November 10, 2021 Novel Multimodal Treatment Regimen for the Management of Primary Sacrococcygeal Cystic Echinococcosis
November 10, 2021 Novel Multimodal Treatment Regimen for the Management of Primary Sacrococcygeal Cystic Echinococcosis June 1, 2025 Management of Ipsilateral Pilon with Calcaneal Fractures: A Rare Case Report
June 1, 2025 Management of Ipsilateral Pilon with Calcaneal Fractures: A Rare Case Report April 10, 2016 Reviewers Acknowledgement & Photo-gallery April – June 2016
April 10, 2016 Reviewers Acknowledgement & Photo-gallery April – June 2016 March 10, 2020 Reviewers Acknowledgement & Photo-gallery March – April 2020
March 10, 2020 Reviewers Acknowledgement & Photo-gallery March – April 2020