
Trevor disease around the ankle can have an aggressive course, with prompt recognition and timely surgical excision can prevent morbidity, instability and deformity.
Dr. Siddhartha Sharma, Department of Orthopedics, Foot and Ankle Biomechanics, Experimentation and Research Laboratory, Postgraduate Institute of Medical Education and Research, Chandigarh, India. E-mail: sids82@gmail.com
Abstract
Introduction: Dysplasia epiphysealis hemimelica, also known as Trevor disease, is a rare skeletal development disorder of childhood, characterized by asymmetric growth of the epiphyseal cartilage in childhood. The disease can be locally aggressive at the ankle, and can result in deformity or instability. We present a case of Trevor disease involving the lateral aspect of distal tibia and talus in a 9-year-old patient, and of highlight its clinical and radiological presentation, treatment, and outcomes.
Case Report: A 9-year-old male presented with a painful swelling over the lateral aspect of the dorsum of right ankle and foot swelling for the past 1.5 years. Radiographs and computed tomography scan revealed exostoses arising from the lateral distal tibial epiphysis and talar dome. Skeletal survey revealed cartilaginous exostoses in distal femoral epiphyses, confirming the diagnosis. Wide resection was done, and the patients were asymptomatic and recurrence-free at 8 months follow-up.
Conclusion: Trevor disease around the ankle can have an aggressive course. Prompt recognition and timely surgical excision can prevent morbidity, instability, and deformity.
Keywords: Trevor disease, dysplasia epiphysealis hemimelica, ankle, exostosis, resection.
Dysplasia epiphysealis hemimelica, also known as Trevor disease, is a rare skeletal development disorder of childhood, characterized by asymmetric growth of the epiphyseal cartilage in childhood [1]. It is rare, the reported incidence is 1 in 1 million. The most commonly affects children in the 2–14 years age group; it has 3 times higher male preponderance. The lower limb is most frequently affected, especially the ankle joint, followed by the knee joint [2-4]. The disease can be locally aggressive at the ankle, and can result in deformity or instability. Most cases are asymptomatic; however, the common clinical presentation is a slow-growing, painless mass, localized to the medial side of the ankle. This may eventually increase in size, leading to pain, deformity, instability, blisters, and edema and necessitate resection and close follow-up till skeletal maturity [2]. Due to the rare nature of the condition or asymptomatic nature, there is a paucity of literature on this subject. We present a case of Trevor disease involving the lateral aspect of distal tibia and talus in a 9-year-old patient with the aims of highlighting its clinical and radiological presentation, treatment, and outcomes.
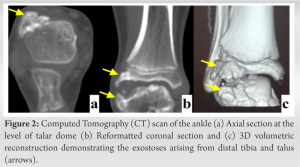
A 9-year-old male presented with a painful swelling over the lateral aspect of the dorsum of right ankle and foot swelling for the past 1.5 years. The swelling had been noticed by his parents, was insidious in onset, and slowly progressive. The patient denied any history of trauma, fever or swelling in other joints of the body. Physical examination revealed a bony swelling over the dorsolateral aspect of the right ankle measuring 4 × 3 cm, which was tender on deep palpation. Temperature over the swelling was normal. There was no deformity at the ankle or hind foot, and the range of motion over the ankle and subtalar joints was bilaterally comparable. The child walked without a limp. Plain radiographs of the ankle showed two exostoses, primarily cartilaginous, over the distal lateral aspect of the tibia and the talus (Fig. 1). Computed tomography (CT) scan confirmed the presence of exostoses originating from the tibia and talus (Fig. 2). 3D CT showed the antero-lateral growth involving the antero-lateral aspect of distal tibia and dorsal lateral aspect of talus over epiphyseal region. 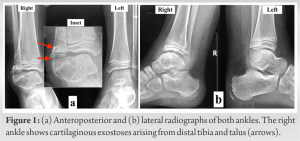
Considering the progressive symptoms, a decision for surgical excision was taken, after informed discussion with the family. An anterolateral approach to the ankle was chosen, centered over the swellings (Fig. 3). A plane was developed between the peroneal tendons and extensor digitorum tendons. The swellings over the tibia and talus were exposed, and excised in an extra-periosteal fashion, taking care not to damage the physeal cartilage (Fig. 4). Histopathology of the sample revealed primarily matures cartilaginous, with no cellular atypia; this was reported as showing features consistent with cartilaginous osteochondroma.
The patient was discharged in stable condition with a below knee cast for 2 weeks, when sutures were removed and patient was allowed weight bearing, as tolerated, in an ankle boot walker for another 4 weeks. Serial review at 3, 6, and 8 months (Fig. 5) showed no evidence of recurrence. The patient was asymptomatic at the final follow-up of 8 months.
The first account of Trevor disease can be attributed to Mouchet and Belot, who in 1926, described this condition as “tarsomegaly” [3]. However, the condition was accurately identified by Trevor in 1950, in a series of ten cases [4]. One further case report in 1953 gave this condition the title of Chondrodystrophie epiphysaire, describing it as a congenital dystrophy of the epiphysis depicting advanced ossification centers [5]. Fairbank then described the disease as “dysplasia epiphysealis hemimelica,” as it is confined to one side of the limb [2]. The entity is characterized by irregular ossification centers, which may develop together or individually, leading to irregular cartilage overgrowth, involving either the lateral or the medial part of the bone [2]. However, there have been cases involving the medial and lateral aspects of the ankle simultaneously, raising concerns on whether the term “hemimelica” should be used to describe this condition [6]. Taking cognizance of this problem, Azouz et al. have further classified Trevor Disease as “localized” (only one epiphysis is affected), “classic” (more than one epiphysis in the same limb is affected) or “generalized,” where the entire limb is affected [7]. The most commonly affected bones are tibia and fibula (22%), talus and calcaneus (22%), distal femur (21%), proximal tibia (11%), navicular, cuboid, cuneiforms, (10%) and the incidence in the upper limb is rare between 1 and 2%. Hensinger has demonstrated a single case report of familial preponderance in 2 generations of the same family, however Trevor’s disease is known to be independent of genetic or environmental determinant [8]. Trevor disease presents with painless localized asymmetric growth which may lead to deformity and pain in some patients. Other symptoms, such as joint deformity, limb length discrepancy, locking of the joint, and muscle wasting leading to limp, may occur variably [9]. Plain radiographs are the first steps in management and identifying the condition, where the epiphysis shows an osteochondral protuberance demonstrating a partially ossified, lobulated, cartilaginous mass arising unilaterally from the affected epiphysis with or without an osseous connection, depicting an asymmetrical growth. CT scan can help to differentiate the pathology from the normal physis and is useful for planning resection. On T2-weighted Magnetic resonance imaging (MRI) sections, Trevor disease lesions show the same high-signal intensity as normal cartilage, with interspersed foci of low signal corresponding to calcifications [10]. Thus, MRI helps in not only delineating the soft-tissue margins and the extent of epiphyseal involvement but differentiating the epiphyseal tissue from accessory ossification center. The histopathological features of Trevor disease resemble osteochondroma, with varying degrees of endochondral ossification as well as hyaline cartilage cap, without malignant transformation [11]. There is a lack of consensus on the treatment of Trevor disease due to its rarity, asymptomatic presentation and variability of its nature. Asymptomatic patients are treated non-operatively, under close follow-up, till skeletal maturity [12]. Operative management is reserved for symptomatic lesions. The goal of surgical intervention is complete removal of the osseous growth, without injuring the epiphysis. Keret et al. have divided the lesions into intra- and extra-articular. Whereas excision is the treatment of choice for extra-articular growths and has excellent outcomes, intra-articular involvement results in unfavorable results [13].
Trevor disease is a rare condition of asymmetrical growth of the epiphysis, with the most common presentation over the ankle region. Although it is rare, its course around the ankle joint is particularly aggressive. Whereas asymptomatic patient can be kept under close follow up till skeletal maturity, symptomatic patients need surgical excision to prevent further pain, deformity and growth disturbance.
The present report highlights the diagnostic features of Trevor Disease of the ankle. Prompt recognition and timely surgical intervention in selected cases can help prevent morbidity, deformity and instability.
References
- 1.Wynne-Davis R, Hall CM, Apley AG. Atlas of Skeletal Dysplasias. London: Churchill Livingstone; 1985. p. 539-43. [Google Scholar | PubMed]
- 2.Fairbank TJ. Dysplasia epiphysialis hemimelica (tarso-epiphyseal aclasis). J Bone Joint Surg Br 1956;38-B:237-57. [Google Scholar | PubMed]
- 3.Mouchet A, Belot J. Tarso megalia. J Radiol Electrol 1926;10:289-93. [Google Scholar | PubMed]
- 4.Trevor D. Tarso-epiphysial aclasis; a congenital error of epiphysial development. J Bone Joint Surg Br 1950;32-B:204-13. [Google Scholar | PubMed]
- 5.Ingelrans P, Lacheretz M. A case of ephysial chondrodystrophy. Rev Chir Orthop Reparatrice Appar Mot 1953;39:242-8. [Google Scholar | PubMed]
- 6.Uygur E, Demiroğlu M, Aydin D, Kiliç B, Özkan K. An unusual presentation of Trevor’s disease at the ankle joint: Involvement of both medial and lateral epiphyses. Foot (Edinb) 2018;36:55-8. [Google Scholar | PubMed]
- 7.Azouz, EM, Slomic AM, Marton D, Rigault P, Finidori G. The manifestations of dysplasia epiphysealis hemimelica. Pediatr Radiol 1985;15:44-9. [Google Scholar | PubMed]
- 8.Hensinger RN, Cowell HR, Ramsey PL, Leopold RG. Familial dysplasia epiphysealis hemimelica, associated with chondromas and osteochondromas. Report of a kindred with variable presentations. J Bone Joint Surg Am 1974;56:1513-6. [Google Scholar | PubMed]
- 9.Graves SC, Kuester DJ, Richardson EG. Dysplasia epiphysealis hemimelica (Trevor disease) presenting as peroneal spastic flatfoot deformity: A case report. Foot Ankle 1991;12:55-8. [Google Scholar | PubMed]
- 10.Freihaut RB, O’Keane JC, Stephens MM. Dysplasia epiphysealis hemimelica with associated osteochondral lesion of the talus: A case report and review of the literature. Foot Ankle Int 2007;28:727-30. [Google Scholar | PubMed]
- 11.Nowicki PD, Borders H. Dysplasia epiphysealis hemimelica (Trevor disease) of the ankle. Orthopedics 2015;38:216, 269-71. [Google Scholar | PubMed]
- 12.Kuo RS, Bellemore MC, Monsell FP, Frawley K, Kozlowski K. Dysplasia epiphysealis hemimelica: Clinical features and management. J Pediatr Orthop 1998;18:543-8. [Google Scholar | PubMed]
- 13.Keret D, Spatz DK, Caro PA, Mason DE. Dysplasia epiphysealis hemimelica: Diagnosis and treatment. J Pediatr Orthop 1992;12:365-72. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Osteochondroma of Dorsal Spine: A Rare Clinical Entity
April 1, 2026 Osteochondroma of Dorsal Spine: A Rare Clinical Entity November 1, 2025 Distal Fibula Osteochondroma with Peroneal Tendon Subluxation – A Case Report
November 1, 2025 Distal Fibula Osteochondroma with Peroneal Tendon Subluxation – A Case Report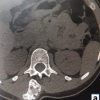 October 1, 2025 Pedunculated Exostosis of the Pedicle of Lumbar Vertebra: A Rare Cause of Lumbar Pain and Swelling
October 1, 2025 Pedunculated Exostosis of the Pedicle of Lumbar Vertebra: A Rare Cause of Lumbar Pain and Swelling January 1, 2025 Open Ankle Injury without Associated Fracture or Dislocation Requiring Surgical Intervention: A Case Report
January 1, 2025 Open Ankle Injury without Associated Fracture or Dislocation Requiring Surgical Intervention: A Case Report