
Limb salvage surgery is a viable option for recurrent malignant peripheral nerve sheath tumors of the upper limb.
Dr. Marlon M Mencia, Department of Clinical Surgical Sciences, The University of the West Indies, Port of Spain General Hospital, Charlotte Street, Port of Spain, Trinidad, West Indies. E-mail: mmmencia@me.com
Abstract
Introduction: A malignant peripheral nerve sheath tumor (MPNST) is a rare soft-tissue sarcoma with a high recurrence rate and poor prognosis. Early diagnosis and complete surgical excision are the fundamental principles of treatment. A benign presentation and low clinical suspicion often delay definitive diagnosis, and en bloc excision may not be feasible depending on the size and location of the tumor. We describe a rare case of a recurrent MPNST successfully treated by surgical excision.
Case Report: A 35-year-old woman presented with a rapidly growing painful mass 3 months following incomplete removal of a MPNST from her forearm. Staging investigations showed no evidence of metastasis. The patient underwent en-bloc surgical excision, split skin grafting, and adjuvant radiation therapy. Histology and immunohistochemical analysis confirmed a MPNST. Five years after having surgery, the patient shows no evidence of recurrence and has excellent function.
Conclusion: MPNST are rare soft tissue sarcomas that can masquerade as benign lumps. There is a paucity of literature on the outcome of surgically-treated recurrent disease. Notwithstanding local recurrence of the tumor, complete surgical excision can yield excellent clinical results.
Keywords: Malignant peripheral nerve sheath tumor, soft-tissue sarcoma, en bloc excision, recurrence, radiation therapy.
Malignant peripheral nerve sheath tumors (MPNST) are a rare and aggressive sub-type of soft-tissue sarcoma. Histologically of ecto-mesenchymal origins with a tendency to metastasize, they represent 5–10% of soft-tissue sarcomas [1]. These tumors primarily affect young- and middle-aged adults without gender preference and display a resistance to chemotherapy treatment [2]. Most MPNSTs arise from a peripheral nerve, a pre-existing neurofibroma, or in association with neurofibromatosis type 1 (NF1). More than 50% develop alongside establised NF1, while the remainder are sporadic mutations or radiation therapy induced [3,4]. The management of MPNSTs is often a complex process. Most tumors present as a painful lump associated with paraesthesia and aggressive growth. Prompt biopsy and immunohistochemical analysis are recommended, however, without a pathognomonic molecular marker, an accurate diagnosis is difficult [5]. Another challenge is the size and location of some tumors which prevent complete surgical resection [4,6]. Furthermore, although adjuvant radiotherapy and chemotherapy are beneficial, their efficacy remains controversial [7]. These challenges make management difficult and despite aggressive treatment, MPNSTs are associated with high recurrence, frequent metastasis, and an overall poor prognosis. This case report discusses the successful surgical treatment of a 35-year-old woman with a recurrent MPNST of the forearm.
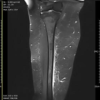
A 35-year-old right-handed woman presented to her local health office with a 6-month history of a painful lump on her left forearm. The pain was not affected by elbow movement, but the patient complained of tingling radiating from the lump to the dorsum of her hand. Her past medical history was unremarkable, and she reported no constitutional symptoms. Clinically the lump, which measured 2.0 cm × 1.0 cm, did not display any suspicious features. The primary care physician assumed that it was a lipoma and removed it under local anesthetic. The pathology report showed a heterogeneous proliferation of spindle cells with abundant mitotic figures suggestive of an MPNST. Regretfully, despite numerous attempts the health office was unable to contact the patient. Three months later, the patient presented to our clinic with a painful, rapidly growing mass arising from her previous surgical site. At this point, the mass measured 7.0 × 5.5 cm was firmly attached to the deeper tissues. The overlying skin was stretched, appearing thin and shiny, but there were no enlarged lymph nodes and normal distal neurovascular function (Fig. 1 and 2). A magnetic resonance imaging (MRI) scan demonstrated a hyperintense fusiform mass on the T2-weighted image signal with peripheral enhancement post-gadolinium administration. The mass that did not seem to involve the fascia appeared to originate from the lateral antebrachial cutaneous nerve, consistent with MPNST (Fig. 3). A chest computerized tomography scan showed no evidence of pulmonary metastases. At a multidisciplinary team meeting with the patient, we used a shared-decision model, agreeing that surgical excision was the most appropriate course of action. The patient gave informed consent for the use of her anonymized images in this case report. Operating under a tourniquet (without exsanguination) to produce a bloodless field, we made an elliptical incision approximately 2 cm from the lesion’s margins and sharply dissected it off the underlying muscle. Proximally, the tumor had penetrated the fascia and was adherent to the muscle bellies of the brachioradialis and extensor carpi radialis longus. To effect complete excision of the tumour, we dissected deep into the muscle bellies sacrificing approximately 50% of the muscles while leaving their tendinous origins intact. Extensor carpi radialis brevis was not involved and therefore left undisturbed. Both median and radial nerves were exposed and protected throughout the procedure. At the end of the operation, the base of the wound appeared healthy and was temporarily covered with a vacuum-assisted device (Fig. 4). Histology confirmed a high grade, poorly differentiated spindle cell tumor with invasion into the dermis and the underlying skeletal muscle. The mass was partially encapsulated with a peripheral attachment to surrounding nerve bundles. The circumferential and deep margins had a minimum clearance of 2 mm. Immunohistochemistry was positive for the S100 protein with focal staining, and the appearance was consistent with MPNST. Fourteen days later, we returned to the operating theatre, debrided the wound bed to encourage bleeding, and placed a split skin graft over the defect. We applied a wrist drop splint for 1 month to encourage maximum “take” of the skin graft. Gentle physiotherapy and occupational therapy were then commenced to regain movement and strength in the upper limb. Three months later, following advice from the radiation oncologist, we referred the patient for external beam radiation therapy (Total 64 Gy–50Gy/25 fractions and 14Gy/7 fractions). The patient who shows no evidence of local recurrence (LR) is reviewed annually using surveillance MRI imaging. Five years after surgery, the patient reports minimal discomfort while using her arm and has returned to work as an administrative assistant. Physical examination demonstrated an excellent range of wrist and elbow movement (Fig. 5). Her Disabilities of the Arm, Shoulder, and Hand score and EuroQoL 5 Dimensions scores were 12.5 and 0.799 respectively, implying excellent function.
While MPNSTs may resemble benign tumors, their clinical course is often aggressive and recurrence rates are high. Complete surgical excision and adjuvant therapy are recommended for primary tumors, but there is a paucity of literature on outcomes following LR. Our discussion focuses on the difficulties encountered in establishing the diagnosis, surgical management of LR, and the functional outcome. MPNST are rare and perplexing malignancies. The best clinical outcomes are linked to early diagnosis and treatment [8]. However, several factors combine to make the diagnosis challenging. First, MPNSTs often present as benign-looking soft-tissue lumps. It is therefore not surprising that many tumors are in the first instance inadequately excised. Surgery that does not completely remove the tumor can initiate an aggressive secondary response which is often the first clinical clue to its menacing nature [9]. Second, clinicians are unlikely to be familiar with these rare tumors. MPNSTs have an incidence of 0.001% in the general population therefore it is improbable that a primary care physician would even encounter a single case during their career. Lack of awareness and low clinical suspicion are likely contributors to late detection. Third, MPNSTs are spindle cell tumors which share similar histological features with other benign tumors. This cellular resemblance presents a diagnostic challenge. While immunohistochemistry is helpful in some cases, it is constrained by the absence of a pathognomonic tumor marker for MPNST [5]. Several tumor markers show promise. In this regard, the S 100 protein is considered the best marker for MPNST but has limited diagnostic accuracy and is positive in only 50–90% of tumors [10]. The innocuous presentation of MPNST in our patient combined with clinical naivety resulted in incomplete excision. The tumor revealed its true ominous character by quickly reappearing in a larger form. This clinically aggressive behavior, together with characteristic histological features and immunohistochemistry (S100 protein-focal positive staining), were clues to the diagnosis. The rapid and invasive growth of MPNST is related to the poor prognosis for most patients with the disease. Not surprisingly, therefore, an aggressive surgical approach of wide local excision with negative surgical margins combined with adjuvant radiation therapy is the mainstay of contemporary treatment [3,5]. In a retrospective study of 71 patients treated with surgery and radiation therapy for localized MPNST, Bishop et al. reported a 5-year LR and disease-specific survival (DSS) rate of 84% and 66%, respectively. Positive or uncertain surgical margins were the only factors adversely associated with LR [11]. In a similar study, Stucky et al. evaluated 175 patients diagnosed with MPNST from the Mayo Clinic, reporting on patient outcomes and prognostic variables. The authors found an LR rate of 22% and a 5-year DSS rate of 60%. Tumor size >5 cm, LR, high grade, and truncal location were poor prognostic indicators for DSS [3]. In an attempt to add clarity, Cai et al. performed a systematic review and meta-analysis to investigate the 5-year overall survival (OS), 5-year event-free survival (EFS), and LR rate for MPNST and to assess prognostic risk factors. They found a pooled 5-year OS rate, 5-year EFS rate, and LR rate of 49%, 37%, and 38%, respectively. The worst prognosis was associated with large tumor size, depth, and positive margin status. They concluded that the survival and LR of MPNST were poor and complete resection with adequate surgical margins remains the mainstay of treatment for most patients [12]. A resection margin is considered microscopically negative (R0) if the closest margin is>1 mm from the inked surface. The peripheral margins of our specimen were clear by >1 cm; the closest margin along the deep surface was reported as 2 mm. The skin-grafted tumor-base tolerated radiation therapy very well, although this is not proven to confer an OS advantage [7]. At 5 years’ post-surgery, the patient remains healthy with no evidence of LR or metastasis. Radical surgical excision of MPNST improves OS but may result in significant morbidity and loss of function. In a retrospective review of 658 patients with MPNST treated with surgery, Martin et al. reported that 61 patients underwent amputations, and 27.2% had <M3 muscle power and 24.3% critical sensory loss (defined as partial or complete loss of hand, foot, or buttock sensation) [13]. Vetrano et al. reviewed the clinical, histologic, and imaging data of 42 patients treated at their institution to identify factors that may improve the surgical outcome of peripheral nerve sheath tumors. The timing of surgery was found to be the most important predictive factor of outcome with MPNSTs having the worst outcomes [8]. Notwithstanding a larger recurrent lesion, we excised the tumor en bloc without sacrificing critical structures that could affect the functional outcome. Our patient reports high region-specific and general health-related quality of life scores. She returned to work 1 year after surgery and currently participates in low-intensity recreational exercise.
MPNST are rare and aggressive soft-tissue sarcomas with a dismal prognosis. Complete resection is not always feasible, and high LR rates present another challenge to successful treatment. Furthermore, the tumor demonstrates a strong metastatic tendency. Compounded by a poor response to radiation therapy, the mortality rate remains unacceptably high [14]. There is an urgent need for a better understanding of tumor biology, including developing more effective diagnostic tests and treatment algorithms. Disease-specific biomarkers of MPNST will make diagnosis easier while understanding the pathogenesis will improve the treatment and outcome of patients. Suboptimal outcomes highlight the need for further research into the pathophysiology of this disease and clinical trials to evaluate emerging treatment options.
There is a relatively small body of literature that is concerned with the treatment of recurrence following surgical excision of MPNSTs. Despite the general trend of poor results, this case report illustrates that a good functional outcome can be expected when these rare tumors are treated with meticulous surgery and adjuvant radiotherapy.
References
- 1.Ng VY, Scharschmidt TJ, Mayerson JL, Fisher JL. Incidence and survival in sarcoma in the United States: A focus on musculoskeletal lesions. Anticancer Res 2013;33:2597-604. [Google Scholar | PubMed]
- 2.Baehring JM, Betensky RA, Batchelor TT. Malignant peripheral nerve sheath tumor: The clinical spectrum and outcome of treatment. Neurology 2003;61:696-8. [Google Scholar | PubMed]
- 3.Stucky CC, Johnson KN, Gray RJ, Pockaj BA, Ocal IT, Rose PS, et al. Malignant peripheral nerve sheath tumors (MPNST): The Mayo Clinic experience. Ann Surg Oncol 2012;19:878-85. [Google Scholar | PubMed]
- 4.Wanebo JE, Malik JM, VandenBerg SR, Wanebo HJ, Driesen N, Persing JA. Malignant peripheral nerve sheath tumors. A clinicopathologic study of 28 cases. Cancer 1993;71:1247-53. [Google Scholar | PubMed]
- 5.Boto J, Boudabbous S, Lobrinus JA, Gourmaud J, Terraz S. Solitary neurofibroma of the spermatic cord: A case report. J Radiol Case Rep 2015;9:19-28. [Google Scholar | PubMed]
- 6.Kar M, Deo SV, Shukla NK, Malik A, DattaGupta S, Mohanti BK, et al. Malignant peripheral nerve sheath tumors (MPNST)--clinicopathological study and treatment outcome of twenty-four cases. World J Surg Oncol 2006;4:55. [Google Scholar | PubMed]
- 7.Kahn J, Gillespie A, Tsokos M, Ondos J, Dombi E, Camphausen K, et al. Radiation therapy in management of sporadic and neurofibromatosis type 1-associated malignant peripheral nerve sheath tumors. Front Oncol 2014;4:324. [Google Scholar | PubMed]
- 8.Vetrano IG, Lucarella F, Dalolio M, Di Cristofori A, Nataloni IF, Tiberio F, et al. The importance of predicting factors in the surgical outcome of peripheral nerve sheath tumors. J Neurol Surg A Cent Eur Neurosurg 2014;75:104-9. [Google Scholar | PubMed]
- 9.Abdel Al S, Abou Chaar MK, Asha W, Al-Najjar H, Al-Hussaini M. Fungating malignant peripheral nerve sheath tumor arising from a slow-growing mass in the forearm: A case report and review of the literature. J Med Case Rep 2020;14:91. [Google Scholar | PubMed]
- 10.Stasik CJ, Tawfik O. Malignant peripheral nerve sheath tumor with rhabdomyosarcomatous differentiation (malignant triton tumor). Arch Pathol Lab Med 2006;130:1878-81. [Google Scholar | PubMed]
- 11.Bishop AJ, Zagars GK, Torres KE, Bird JE, Feig BW, Guadagnolo BA. Malignant peripheral nerve sheath tumors: A single institution’s experience using combined surgery and radiation therapy. Am J Clin Oncol 2018;41:465-70. [Google Scholar | PubMed]
- 12.Cai Z, Tang X, Liang H, Yang R, Yan T, Guo W. Prognosis and risk factors for malignant peripheral nerve sheath tumor: A systematic review and meta-analysis. World J Surg Oncol 2020;18:257. [Google Scholar | PubMed]
- 13.Martin E, Pendleton C, Verhoef C, Spinner RJ, Coert JH, MONACO Collaborators. Morbidity and function loss after resection of malignant peripheral nerve sheath tumors. Neurosurgery 2021;90:354-64. [Google Scholar | PubMed]
- 14.LaFemina J, Qin LX, Moraco NH, Antonescu CR, Fields RC, Crago AM, et al. Oncologic outcomes of sporadic, neurofibromatosis-associated, and radiation-induced malignant peripheral nerve sheath tumors. Ann Surg Oncol 2013;20:66-72. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Not All Red Flags Indicate Malignancy: A Case Report of a Benign Lipoma Mimicking Soft-tissue Sarcoma
August 1, 2026 Not All Red Flags Indicate Malignancy: A Case Report of a Benign Lipoma Mimicking Soft-tissue Sarcoma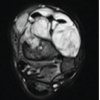 August 1, 2026 Low-Grade Myxofibrosarcoma of the Leg Presenting as a Pathological Pilon Fracture: A Case Report
August 1, 2026 Low-Grade Myxofibrosarcoma of the Leg Presenting as a Pathological Pilon Fracture: A Case Report July 1, 2026 Radiation-Associated Femoral Nonunion and Fixation Failure Following Limb-Salvage Surgery for Thigh Soft-tissue Sarcoma: Two Case Reports and a Review of the Literature
July 1, 2026 Radiation-Associated Femoral Nonunion and Fixation Failure Following Limb-Salvage Surgery for Thigh Soft-tissue Sarcoma: Two Case Reports and a Review of the Literature June 1, 2026 Giant Cell Tumor of the Metacarpal Treated with Non-Vascularized Bone Graft: A Case
June 1, 2026 Giant Cell Tumor of the Metacarpal Treated with Non-Vascularized Bone Graft: A Case