
Ramp lesions are complex and challenging to diagnose due to their hidden nature in standard imaging procedures, necessitating advanced magnetic resonance imaging techniques or arthroscopic intervention for accurate detection.
Dr. Iffath Misbah, Department of Radiodiagnosis, Saveetha Institute of Medical and Technical Sciences, Chennai, Tami Nadu, India. E-mail: iffathmisbahcp@gmail.com
Abstract
Introduction: Ramp lesions, often associated with anterior cruciate ligament (ACL) injuries, exhibit a varied incidence rate of 9–42%, increasing with delayed ACL reconstruction. These lesions, resulting from abnormal tibial movements and semimembranosus muscle contraction, are challenging to diagnose due to their hidden nature in standard magnetic resonance imaging and arthroscopy procedures.
Case Report: This report examines the case of a ramp lesion in the context of a multi-ligament injured knee of a 34-year-old male. The patient had a complete ACL, medial collateral ligament, and avulsion of the posterior cruciate ligament with a type 1 ramp lesion. These findings were confirmed by arthroscopy and were treated with arthroscopic reconstruction of the ligament and all inside repair of the ramp lesion. We report the pertinent imaging findings relevant to the ramp lesions.
Conclusion: Ramp lesions present a significant diagnostic and treatment challenge in orthopedic practice. Enhanced imaging techniques and a deeper understanding of their pathophysiology are crucial for an accurate diagnosis.
Keywords: Ramp, hidden lesion, magnetic resonance imaging, arthroscopy.
The posteromedial knee ramp lesions, likened to ramps for their shape, have been known since 1983 but have gained recent attention due to their association with ACL injuries. These lesions, first termed “Ramp lesions” by Michael J. Strobel, involve the peripheral attachment of the posterior horn of the medial meniscus. For years, these injuries were often overlooked in magnetic resonance imaging (MRIs) and arthroscopies, primarily because standard MRI procedures, conducted with the knee fully extended, obscured the posteromedial space. In addition, specific examination techniques, like the trans-notch view and assessment of the medial meniscus posterior horn mobility, are necessary for their diagnosis, leading to them being termed “hidden lesions.” Their significance has risen in line with the quest to perfect ACL reconstructions, as ramp lesions affect both anterior and rotational knee stability. In the literature, ramp lesions are typically defined as longitudinal or oblique superior meniscocapsular junction tears or meniscotibial ligament tears, often <2 cm, and usually accompanying ACL tears. In this report, we present the imaging findings associated with a ramp tear in a young male with multiple ligamentous injuries to the knee.
Here, we report a 34-year-old male presented with knee injury following a collision injury with a moped. He was unable to weight bear and walk following the injury and was subjected to an imaging assessment after preliminary management of the acute knee injury. Plain radiographs of the knee were obtained and demonstrated an increased valgus opening, indicating a medial collateral ligament (MCL) injury (Fig. 1).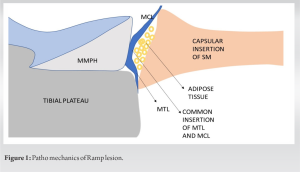 On the MRI, complete disruption of the mid substance of the ACL and a minimally displaced posterior cruciate ligament injury were observed. The lateral collateral ligament was intact; however, the MCL was torn on the tibial side and found to be retracted. Regarding the menisci, the Lateral menisci had a complex posterior horn tear, and the medial meniscus had a horizontal cleavage tear of the posterior horn. Strikingly, there was an irregularity in the posterior margin of the menisco-capsular junction with fluid filling, and this could be attributed to the ramp lesion (Fig. 2). Subsequently, he was taken up for arthroscopic surgery, which confirmed the presence of a ramp tear (Fig. 3).
On the MRI, complete disruption of the mid substance of the ACL and a minimally displaced posterior cruciate ligament injury were observed. The lateral collateral ligament was intact; however, the MCL was torn on the tibial side and found to be retracted. Regarding the menisci, the Lateral menisci had a complex posterior horn tear, and the medial meniscus had a horizontal cleavage tear of the posterior horn. Strikingly, there was an irregularity in the posterior margin of the menisco-capsular junction with fluid filling, and this could be attributed to the ramp lesion (Fig. 2). Subsequently, he was taken up for arthroscopic surgery, which confirmed the presence of a ramp tear (Fig. 3). 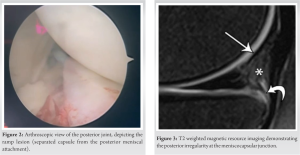 The order of reconstruction was ACL reconstruction, medial and lateral meniscal repair, ramp repair, and finally, medial collateral ligament repair was performed. The PCL was left to conservative management.
The order of reconstruction was ACL reconstruction, medial and lateral meniscal repair, ramp repair, and finally, medial collateral ligament repair was performed. The PCL was left to conservative management.
Ramp lesions, often associated with ACL tears, vary in incidence from 9% to 42%, increasing when ACL reconstruction is delayed beyond 3 months. Jiang et al. [1] found 20 cases of ramp lesions without complete ACL tears, linked instead to ACL longitudinal splits, suggesting minimal anterior instability and semimembranosus contraction as potential causes (Fig. 1). The true prevalence of ramp lesions, either alone or with ACL tears, is unclear due to difficulties in detection through MRI and arthroscopy. Notably, their incidence is consistent across adult and pediatric populations, contrasting with the higher prevalence of other meniscal injuries in younger age groups [2,3].
Ramp lesions after an ACL tear are mainly due to excessive anterior tibia movement, causing semimembranosus muscle contraction and stressing the surrounding ligaments. This stress, coupled with the medial meniscus being compressed between the articular surfaces, leads to these lesions. They can also result from valgus injuries involving internal tibia rotation and axial loading or as a contrecoup injury from pivoting movements causing varus strain and femur rotation on the tibia, leading to meniscus trapping and tearing. The sensitivity of 3.0-T MRI (83.3%) was superior to 1.5-T MRI (67.6%), according to Hatayama et al. [4]. Irregularity at the posterior margin and complete fluid filling were the most sensitive findings for detecting ramp lesions on MRI, according to Yeo et al. [5] and Laurens et al. [6]. Consecutive sagittal images serve to determine which regions of the meniscocapsular junction and posterior horn are torn. Axial images help to assess the mediolateral dimensions of the same lesions. Salient features on MRI [7] are detailed in Table 1.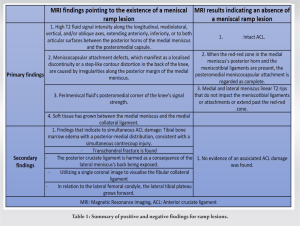
Meniscal ramp lesions have no consented treatment at the present time. Research has shown that ramp lesions in the context of acute ACLR may recover without surgical intervention if the surrounding biological conditions are appropriate. Some have suggested that ramp lesions should be surgically addressed rather than being let to heal on its own due to the hypermobility of the separated meniscocapsular component. There are data to suggest that individuals with similar longitudinal meniscal tear patterns who have ACLR without first having surgery may benefit from nonsurgical treatment. This is against the general view that ramp lesions should be addressed when there is chronic ACL insufficiency [8,9,10].
These lesions result from abnormal tibia movement and semimembranosus contraction, often undetected due to diagnostic challenges. They occur consistently across all age groups, unlike other meniscal injuries. Advanced MRI techniques offer improved detection, with specific imaging features aiding in their identification. Treatment approaches for ramp lesions remain debated, with some cases responding to nonsurgical methods, particularly in acute ACLR contexts, while others advocate for surgical intervention, especially in chronic ACL insufficiency.
A suspicious irregularity in the posterior meniscopcapsular junction should raise suspicion of ramp lesions, and it is imperative to confirm this during knee arthroscopy by probing the meniscocapsular junction posteriorly.
References
- 1.Jiang J, Ni L, Chen J. Isolated meniscal ramp lesion without obvious anterior cruciate ligament rupture. Orthop Surg 2021;13:402-7. [Google Scholar | PubMed]
- 2.Malatray M, Raux S, Peltier A, Pfirrmann C, Seil R, Chotel F. Ramp lesions in ACL deficient knees in children and adolescent population: A high prevalence confirmed in intercondylar and posteromedial exploration. Knee Surg Sports Traumatol Arthrosc 2018;26:1074-9. [Google Scholar | PubMed]
- 3.Qalib YO, Tang Y, Wang D, Xing B, Xu X, Lu H. Ramp lesion of the medial meniscus. EFORT Open Rev 2021;6:372-9. [Google Scholar | PubMed]
- 4.Hatayama K, Terauchi M, Saito K, Aoki J, Nonaka S, Higuchi H. Magnetic resonance imaging diagnosis of medial meniscal ramp lesions in patients with anterior cruciate ligament injuries. Arthroscopy 2018;34:1631-7. [Google Scholar | PubMed]
- 5.Yeo Y, Ahn JM, Kim H, Kang Y, Lee E, Lee JW, et al. MR evaluation of the meniscal ramp lesion in patients with anterior cruciate ligament tear. Skeletal Radiol 2018;47:1683-9. [Google Scholar | PubMed]
- 6.Laurens M, Cavaignac E, Fayolle H, Sylvie R, Lapègue F, Sans N, et al. The accuracy of MRI for the diagnosis of ramp lesions. Skeletal Radiol 2022;51:525-33. [Google Scholar | PubMed]
- 7.Greif DN, Baraga MG, Rizzo MG, Mohile NV, Silva FD, Fox T, et al. MRI appearance of the different meniscal ramp lesion types, with clinical and arthroscopic correlation. Skeletal Radiol 2020;49:677-89. [Google Scholar | PubMed]
- 8.Chahla J, Dean CS, Moatshe G, Mitchell JJ, Cram TR, Yacuzzi C, et al. Meniscal ramp lesions: anatomy, incidence, diagnosis, and treatment. Orthop J Sports Med 2016;4:2325967116657815. [Google Scholar | PubMed]
- 9.Seil R, Hoffmann A, Scheffler S, Theisen D, Mouton C, Pape D. Ramp lesions : Tips and tricks in diagnostics and therapy. Orthopade 2017;46:846-54. [Google Scholar | PubMed]
- 10.DePhillipo NN, Cinque ME, Chahla J, Geeslin AG, Engebretsen L, LaPrade RF. Incidence and detection of meniscal ramp lesions on magnetic resonance imaging in patients with anterior cruciate ligament reconstruction. Am J Sports Med 2017;45:2233-7. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Intra-articular Ganglionic Cysts of Knee: A Cause for Anterior Knee Pain
August 1, 2026 Intra-articular Ganglionic Cysts of Knee: A Cause for Anterior Knee Pain April 1, 2026 Bucket Handle Tear of the Medial Meniscus with a New Magnetic Resonance Imaging Sign: The “Head in the Sand Sign” – A Case Report
April 1, 2026 Bucket Handle Tear of the Medial Meniscus with a New Magnetic Resonance Imaging Sign: The “Head in the Sand Sign” – A Case Report August 6, 2024 A Comparative Study on Correlation between Magnetic Resonance Imaging and Arthroscopic Findings in the Knee Joint Injuries
August 6, 2024 A Comparative Study on Correlation between Magnetic Resonance Imaging and Arthroscopic Findings in the Knee Joint Injuries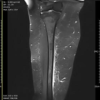 August 1, 2026 Not All Red Flags Indicate Malignancy: A Case Report of a Benign Lipoma Mimicking Soft-tissue Sarcoma
August 1, 2026 Not All Red Flags Indicate Malignancy: A Case Report of a Benign Lipoma Mimicking Soft-tissue Sarcoma