
This case, in conjunction with a comprehensive examination of relevant literature, enhances our comprehension of the clinical features, diagnostic approaches, and treatment results concerning lipomas in the hand, specifically those situated in the index finger. This contributes to the progression of patient care in analogous scenarios.
Dr. Margarita-Michaela Ampadiotaki, Department of Orthopaedics, KAT General Hospital of Attica, 14561, Athens, Greece. E-mail: marab.ortho@gmail.com
Abstract
Introduction: Lipomas are the most common benign mesenchymal tumors found on the head, neck, shoulder, and back, but they are rarely encountered in the fingers, constituting <1% of such tumors.
Case Report: This case report presents an exceptional location of a giant lipoma on the proximal phalanx of a 60-year-old Caucasian male’s right index finger, alongside a literature review that identified 20 similar cases. The patient, with no significant health issues, reported that the growth had been asymptomatic for 2 years before seeking consultation due to aesthetic concerns and impaired finger extension. Diagnostic imaging, including magnetic resonance imaging preoperatively, and histopathological analysis after surgical excision confirmed the diagnosis of a mature lipoma.
Conclusion: This case contributes to the scarce documentation on finger lipomas, emphasizing the diagnostic challenges they present and the effectiveness of surgical removal in averting recurrence. It also highlights the unusual demographic occurrence, given the predominant presentation in middle-aged females, and underscores the necessity of considering lipomas in the differential diagnosis of finger masses. The literature review expands on the rarity of this condition, providing an analysis of 20 other cases, thereby enriching the understanding of lipoma manifestations in rare locations.
Keywords: Lipoma, finger, index, case report.
Lipomas, benign tumors predominantly composed of adipose tissue, are among the most common mesenchymal neoplasms, affecting approximately 1% of the population [1]. Despite their widespread distribution across areas rich in fat, including head, neck, shoulder, back, and extremities, their manifestation within the hand and particularly in the fingers is exceptionally rare, contributing to <1% of all cases [2]. Notably, there is a slightly higher incidence of lipomas in females compared to males. These tumors can arise at any age but are most frequently observed between the fourth to sixth decades of life, suggesting a predilection toward middle-aged individuals [3]. The literature records a limited number of finger lipomas, with an even smaller fraction classified as giant lipomas, defined by a size greater than 5 cm. Such occurrences in the fingers are particularly uncommon, ranging from asymptomatic growths to those capable of affecting functionality and causing neurological symptoms [4]. This article presents a distinctive case of a giant lipoma in the proximal phalanx of the right index finger in a 60-year-old patient, notable for its absence of a traumatic history and compressive symptoms. This addition to the clinical literature not only underscores the rarity of lipoma occurrence in such locations but also highlights the importance of meticulous examination and intervention, given their potential impact on mobility and neurological outcomes.
A 60-year-old Caucasian male patient sought consultation at our outpatient clinic, presenting with a mass on the dorsal aspect of the right index finger. He was in optimal health, presenting no underlying medical conditions and not undergoing any pharmacological treatment. Professionally, he was employed as a plumber. The patient reported initial observation of the mass approximately 2 years before his first medical consultation, noting that it had remained asymptomatic for most of that period. The decision to seek medical evaluation was driven by esthetic concerns and a recent onset of functional impairment; specifically, the patient experienced a limitation in the range of motion, particularly in extending the finger, which had developed over the past 2 months. On clinical evaluation, the patient exhibited a soft, mobile, and elastic mass located on the dorsal aspect of the right index finger. Neurological assessment revealed no symptoms, and there were no indications of inflammation present. Diagnostic imaging commenced with a plain anteroposterior radiograph of the affected digit, which confirmed the absence of bone invasion. Subsequently, a magnetic resonance imaging (MRI) scan was performed, accurately delineating the lesion’s precise location. The MRI findings facilitated a differential diagnosis, with the characteristics of the mass strongly suggesting a lipoma (Fig. 1). Based on these assessments, the medical team recommended surgical excision of the mass. Accordingly, the patient was scheduled for surgery to remove the lesion.

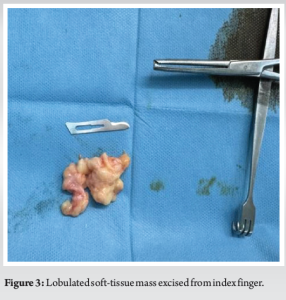
The operation was performed under local anesthesia (Lidocaine Hydrochloride 2%) and employing a tourniquet for hemostasis, a longitudinal incision was made on the dorsal aspect of the index finger. This approach revealed a fatty, lobulated mass situated within the subcutaneous layer, adjacent to the proximal phalanx of the digit, yet not encroaching on the tendon fascicles (Fig. 2). The lesion was meticulously excised in its entirety, with careful preservation of the surrounding neurovascular structures and extensor tendons (Fig. 3). The excised specimen was measured at 6.5 × 2.2 × 1.5.

Histopathological analysis confirmed the presence of mature adipose tissue, corroborating the diagnosis of mature lipoma as suggested by the initial clinical and MRI assessments. The post-operative course was uneventful, with suture removal conducted 15 days post-surgery. During the 1-year follow-up period, there has been no recurrence of the lesion, and the patient had a fully functional hand with no complaints.
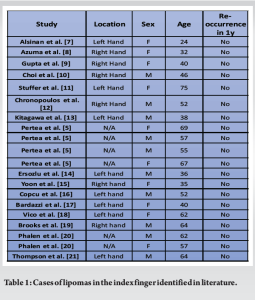
Lipomas are the most prevalent benign tumors of the soft tissues and rank as the third most common type in the upper limbs. Despite this, lipomas located in the hands and fingers are extremely rare, with only a small number of individual cases or case series reported in the literature [5]. The exact origin of lipomas remains unclear. It is noted that about 5% of individuals diagnosed with a lipoma present with multiple lesions and have a family history of the condition, suggesting an autosomal dominant inheritance pattern [5]. Hand lipomas typically exhibit slow growth and, in most instances, are asymptomatic, manifesting as a palpable and movable mass. Bocchiotti et al. suggested that giant lipomas exceeding 50 mm in size were more prone to being symptomatic [6]. When diagnosing a mass on the finger that resembles a lipoma, it is crucial to consider both benign and malignant lesions, such as liposarcoma, lipoblastoma, giant cell tumor, spindle cell lipoma, angiolipoma, neural fibrolipoma, cyst, pyogenic granuloma, and nodular fasciitis, due to their clinical similarities to finger lipoma. Biopsy is often deemed unnecessary because imaging, such as MRI, can provide sufficient diagnostic information. On conducting a thorough review of the literature, we identified a limited number of cases involving lipomas located on the index finger, thereby highlighting the uncommon nature of the case documented in our case. Clinically, these tumors are characterized by their asymptomatic nature and slow growth rate, often prompting medical consultation due to reduced range of motion or cosmetic concerns. Our investigation revealed only 20 reported cases of lipomas in the index finger, affecting females and males in equal percentages, with a median age of 51.3 years (range, 24–75 years). This finding aligns with medical literature that suggests lipomas are more commonly observed in individuals of middle age. Following surgical removal, there were no reports of recurrence, suggesting effective management through surgical intervention (Table 1).
Our case report of a 60-year-old Caucasian male presenting with a giant lipoma on the dorsal aspect of the right index finger contributes to the limited body of literature on this rare occurrence. The successful diagnosis and surgical intervention underscore the significance of considering lipomas within the differential diagnosis for masses in the fingers, despite their rarity in this location. This case emphasizes the importance of a comprehensive diagnostic approach, incorporating clinical evaluation, advanced imaging techniques including MRI, and histopathological analysis to accurately identify and manage these benign tumors. The absence of recurrence and the full restoration of finger mobility post-surgery in our patient highlight the effectiveness of surgical excision as a definitive treatment for lipomas of the finger. Several studies recommend the surgical excision of a finger lipoma in case of pain or restricted range of motion. Considering the favorable rates of post-operative follow-up, such as minimal complications and no recurrence rates, surgical resection might be preferable even in asymptomatic cases.
One notable aspect of this case report is its rarity, given that encountering lipomas in the index finger is uncommon. Our findings, aligned with the review of existing literature, reiterate the uncommon presentation of lipomas in the index finger, and the necessity for differential diagnosis considering both benign and malignant tumors. The prevalence of such cases in middle-aged individuals, particularly females, adds a demographic perspective to the clinical profile of finger lipomas. This case, alongside a review of pertinent literature, enriches our understanding of the clinical characteristics, diagnostic strategies, and management outcomes for lipomas in the hand, particularly those located in the index finger, thereby aiding in the advancement of patient care in similar cases.
This case, in conjunction with a comprehensive examination of relevant literature, enhances our comprehension of the clinical features, diagnostic approaches, and treatment results concerning lipomas in the hand, specifically those situated in the index finger. This contributes to the progression of patient care in analogous scenarios.
References
- 1.Todd A, Nickloes D. Lipomas, Practice Essentials, Pathophysiology, Etiology; 2024. Available from: https://emedicine.medscape.com/article/191233-overview?form=fpf#a6 [Last accessed on 2024 Mar 21]. [Google Scholar | PubMed]
- 2.Wafa A, Wani S, Alsinan TA, Alkhonizy S. Multilocular lipoma of the left thumb of the hand: A case report. Case Reports Plast Surg Hand Surg 2021;8:130-3. [Google Scholar | PubMed]
- 3.Johnson CN, Ha AS, Chen E, Davidson D. Lipomatous soft-tissue tumors. J Am Acad Orthop Surg 2018;26:779-88. [Google Scholar | PubMed]
- 4.Elghoul N, Benchakroun M, Bennis A, Zaddoug O, Zine A, Tanane M, et al. A painless restricted motion of the thumb: What etiology? About an uncommon tumor in uncommon localization. Case Rep Orthop 2020;2020:5649204. [Google Scholar | PubMed]
- 5.Pertea M, Lunca S, Filip A, Moraru DC, Carp C, Pinzaru R, et al. Atypical sites of the lipoma on the hand and fingers: Clinical and imaging features and surgical outcomes. Diagnostics (Basel) 2022;12:2286. [Google Scholar | PubMed]
- 6.Bocchiotti MA, Lovati AB, Pegoli L, Pivato G, Pozzi A. A case report of multi-compartmental lipoma of the hand. Case Reports Plast Surg Hand Surg 2018;5:35-8. [Google Scholar | PubMed]
- 7.Alsinan TA, Alhablany TM, Alokaili HR, Altamimi AS, Rashidi ME. Multilocular lipoma in the middle and index fingers: A case report. Cureus 2022;14:e22172. [Google Scholar | PubMed]
- 8.Azuma R, Demitsu T, Hiratsuka Y, Kakurai M, Imagawa I, Yoneda K, et al. Subcutaneous lipoma of the index digit presenting as fingertip bulging. J Dermatol 2006;33:386-7. [Google Scholar | PubMed]
- 9.Gupta A, Singal R, Mittal A, Goyal M. Report of two cases of subcutaneous lipoma over the finger and review of literature: Case series: Benign tumour. Musculoskelet Surg 2011;95:247-9. [Google Scholar | PubMed]
- 10.Choi J, Choi Y, Jung S, Seo B. Giant lipoma in the index finger of the dominant hand of a swimmer: A case report. Jt Dis Relat Surg 2023;34:469-73. [Google Scholar | PubMed]
- 11.Stuffer M, Thurner JE. Lipoma of the index digit--a very rare location. Arch Orthop Trauma Surg 1995;114:239-40. [Google Scholar | PubMed]
- 12.Chronopoulos E, Nikolaos P, Karanikas C, Kalliakmanis A, Plessas S, Neofytou I, et al. Patient presenting with lipoma of the index finger: A case report. Cases J 2010;3:20. [Google Scholar | PubMed]
- 13.Kitagawa Y, Tamai K, Kim Y, Hayashi M, Makino A, Takai S. Lipoma of the finger with bone erosion. J Nippon Med Schl 2012;79:307-11. [Google Scholar | PubMed]
- 14.Ersozlu S, Ozgur AF, Tandogan RN. Lipoma of the index finger. Dermatol Surg 2007;33:382-4. [Google Scholar | PubMed]
- 15.Yoon S, Jung SN. Lipoma of the finger presenting as restricted motion. Indian J Plastic Surg 2008;41:237-8. [Google Scholar | PubMed]
- 16.Copcu E, Sivrioglu NS. Posttraumatic lipoma: Analysis of 10 cases and explanation of possible mechanisms. Dermatol Surg 2003;29:215-20. [Google Scholar | PubMed]
- 17.Bardazzi F, Savoia F, Fanti PA. Subungual lipoma. Br J Dermatol 2003;149:418. [Google Scholar | PubMed]
- 18.Vico P, Heymans O, Goldschmidt D. Les lipomes des doigts. Ann Chir Memb Super 1993;12:352-5. [Google Scholar | PubMed]
- 19.Brooks ML, Mayer DP, Grannick MS, Rhoda CH. Parosteal lipoma of the finger: Preoperative evaluation with computed tomography. Comput Med Imaging Graph 1989;13:481-5. [Google Scholar | PubMed]
- 20.Phalen GS, Kendrick JI, Rodriquez JM. Lipomas of the upper extremity. Plast Reconstr Surg 1971;48:512. [Google Scholar | PubMed]
- 21.Thompson NB, Moneim SM. Lipoma of the index finger in a 64-year-old man: A case report. UNM Orthop Res J 2015;4:64-65. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 National Demographic and Treatment Patterns of Finger Cellulitis, Paronychias, and Felons
February 1, 2026 National Demographic and Treatment Patterns of Finger Cellulitis, Paronychias, and Felons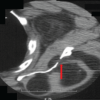 January 1, 2026 Lipomas Eroding Adjacent Bone: Report of Three Cases
January 1, 2026 Lipomas Eroding Adjacent Bone: Report of Three Cases May 1, 2025 Cross-finger Flap on Electrical Ring Burn Injury: A Case Report
May 1, 2025 Cross-finger Flap on Electrical Ring Burn Injury: A Case Report April 1, 2025 Recurrent Intra-articular Lipoma of Ankle Joint; A Rare Case Report
April 1, 2025 Recurrent Intra-articular Lipoma of Ankle Joint; A Rare Case Report