
Simultaneous bilateral ACL reconstruction is a viable treatment option in the adolescent patient.
Dr. Joshua D Rutnagur, Department of Trauma and Orthopaedics, Royal Aberdeen Childrens’ Hospital, Westburn Road, Aberdeen, AB25 2ZG, Scotland, United Kingdom. E-mail: rutnagurj@hotmail.co.uk
Abstract
Introduction: Simultaneous bilateral anterior cruciate ligament (ACL) ruptures are rare, especially in the pediatric population, with very limited evidence. We aimed to review the current literature and present a case study of an adolescent patient who underwent bilateral reconstruction with hamstrings autograft in a single-stage with a partial transphyseal “all-inside” technique. Literature Review: The limited evidence reports that the incidence of growth disturbance following ACL reconstruction in the skeletally immature is 2.6% with no significant difference between a partial transphyseal and an all-epiphyseal technique. Regarding graft choice in the skeletally immature, no significant difference has been found in function using hamstrings versus bone-to-bone patella autograft. The all-inside technique has shown good outcomes in the skeletally immature with no cases of growth disturbance observed in the literature reviewed. Patients spend less days in hospital and return to sport sooner following simultaneous reconstruction versus staged.
Case Report: A 15-year-old male footballer underwent simultaneous reconstruction of bilateral ACL ruptures through a partial transphyseal “all-inside” technique with hamstrings autografts. He began physiotherapy according to local protocol and was discharged from hospital on Day 4 post-operative. He returned to competitive sports 11 months postoperatively with no intraoperative or post-operative complications.
Conclusion: This case suggests that bilateral simultaneous ACL reconstruction is a safe management strategy in the rare case of bilateral ruptures in the skeletally immature, which adds to the evidence base. The number of required hospital stays was reduced and there was return to sport in a comparative time frame to unilateral ACL reconstruction rehabilitation.
Keywords: Anterior cruciate ligament, bilateral, all-inside, adolescent, pediatric, knee.
Rupture of the anterior cruciate ligament (ACL) was once considered rare in the pediatric population; however, they are now being seen with increasing frequency. Recent epidemiological data from the US have suggested a 3-fold increase in the incidence of ACL injury in the skeletally immature between 1990 and 2009. This has been reported due to dramatic increase in youth competitive activity, early sport specialization, and year-round training [1]. Simultaneous bilateral ACL injuries are a rare injury pattern within the literature. There is not a consensus on management of these injuries; however, it has been shown in the adult population that simultaneous repair is a safe and cost-effective approach to management [2]. Treatment strategies for ACL injuries in the skeletally immature have developed, with reluctance to employ conventional techniques used successfully in adults due to risk of physeal damage. Fabricant et al. [3] have shown several physeal-sparing and transphyseal techniques producing good functional outcomes and low complication rates. There is currently no evidence reporting bilateral simultaneous ACL reconstruction using hamstrings autograft and an “all-inside” technique; however, the “all-inside” partial transphyseal technique has reported good subjective and objective clinical outcomes [4]. We report a case of a 15-year-old male who underwent delayed reconstruction of bilateral ACL ruptures with such a strategy.
Management of the unstable knee following ACL injury is important, particularly in the skeletally immature patient, as recurrent instability can lead to chondral and meniscal injury, predisposing to osteoarthritis [5]. While ACL reconstruction treats rotational instability and decreases incidence of future intra-articular wear, surgery in the skeletally immature carries risk of complications relating to disturbance of the physis including leg length discrepancy, angular deformity, or tibial recurvatum. Different surgical techniques have been described and an overall reported rate of growth disturbance after ACL reconstruction of 2.6% with no significant difference between transphyseal and all-epiphyseal techniques [6]. While some studies have demonstrated magnetic resonance imaging (MRI) evidence of physeal disruption, there is no proven evidence of disturbance of growth with a transphyseal technique when compared to all-epiphyseal [7]. Kocher et al. [8] suggested that distance of the graft fixation from the physis was significant in the low occurrence of growth disturbance. Reported outcome scores for both all-epiphyseal and transphyseal techniques have been shown to be equivocal [8]. In Longo et al. [6] systematic review, the mean Lysholm score in the transepiphyseal group was 96.8 and all-epiphyseal group was 95.7. Various graft types have been reported with hamstring autograft most reported. Alternatives are hamstrings allograft and bone-to-bone patella autograft. The type of graft used has not been shown to influence outcome of ACL reconstruction in the skeletally immature and there has been analysis of RCTs showing that hamstrings autograft results in similar restoration of knee function when compared with bone-to-bone patella autograft [9,10]. The all-inside partial transphyseal technique has shown positive subjective and objective clinical outcomes in the skeletally immature [4]. There were no cases of growth disturbance reported. Some studies have suggested that screw fixation has superior biomechanical outcomes when compared with suspensory fixation in ACL reconstruction; however, other studies have shown this not to be the case [11,12]. Suspensory fixation carries a lower risk of physeal damage and growth disturbance when compared with screw fixation [13]. Studies have compared the used of fixed versus adjustable loop devices for suspensory fixation and showed that there was no significant difference in functional outcome or graft failure rates at 2 years follow-up [13]. When managing bilateral ACL ruptures, it has been shown that there is no clinical difference in outcome when patients’ underwent simultaneous reconstruction versus a staged reconstruction [10]. This case series suggests that simultaneous repair is a safe, reproducible, and cost-effective way to manage these rare injuries. In total, patients’ spent less days in hospital and returned to work and sport sooner than having a staged reconstruction. This study was limited by the low numbers involved and the patient group was skeletally mature, making it difficult to draw comparisons. There is, however, a lack of evidence supporting simultaneous reconstruction in the skeletally immature, hence the premise for this report.
A 15-year-old male footballer was referred to the tertiary pediatric orthopedic service 18 months after sustaining bilateral ACL injuries (separate events, 3 months apart). He underwent MRI imaging, demonstrating disruption of the ACL bilaterally. The case was reviewed at the local multidisciplinary team meeting for soft-tissue knee and the patient was offered simultaneous repair. At 36 months post-injury, he underwent bilateral simultaneous repair using an “all-inside” partial transphyseal technique and hamstrings autograft. He began physiotherapy according to the local standardized ACL rehabilitation protocol and was discharged from inpatient care after 4 days. He received weekly face to face physiotherapy and was reviewed by the operating clinician at 3 months, 6 months, and 12 months postoperatively. He attained his rehabilitation milestones and returned to competitive sports 11 months post-operative, which was comparable to the evidence for skeletally immature patients who have undergone unilateral ACL reconstruction [14]. He has had no recurrence of knee pain, stiffness, or symptoms of instability.
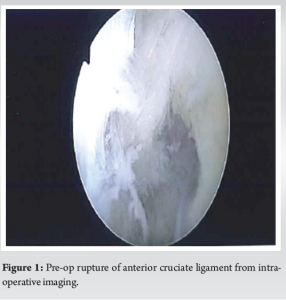
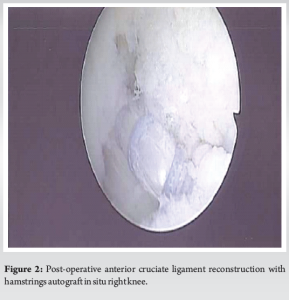
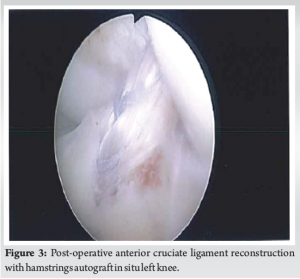
The technique described is a partial transphyseal all-inside ACL reconstruction technique using Arthrex® Endobutton® fixation. Ipsilateral semitendinosus autograft was harvested, prepared with whip-stitch, quadrupled over two tightropes and pre-tensioned. Knee arthroscopy was performed with standard medial and lateral portals. Arthroscopy demonstrated bilateral ACL complete tears with fatty infiltration but no other injury to the posterior cruciate ligament, the menisci, or osteochondral surface. The femoral tunnel was drilled entirely epiphyseal into the lateral femoral condyle and the tibial tunnel was drilled from outside to in. No transphyseal screw was used. The graft was fixed using Endobuttons® at the desired tension. The knees were cycled multiple times and final satisfactory position of the ACL graft was noted. The graft diameters were 8 mm on the left and 8.5 mm on the right. The tibial tunnels were 9 mm diameter bilaterally and the femoral tunnels were 9 mm on the right and 8.5 mm on the left. Fig. 1, 2, and 3 demonstrate the pre-op imaging of one of the ruptured ACLs and both post-operative reconstructed ACLs with hamstrings autograft.
Rehabilitation protocol
Postoperatively, the patient was commenced on a local ACL protocol used in both adolescents and adults. This began day 1 post-operative as follows:
Phase 1 (from day 1)
- Weight bear as able (WBAA)
- Goals: Reduce inflammation, gain full extension, promote distal circulation, gradually regain range of motion (ROM), increase confidence, and promote early mobility.
Phase 2 (from week 1)
- Ideal criteria before progressing to this phase: Full active and passive extension and mobilize independently with/without aids.
- Goals: promote early function, increase ROM, encourage full-weight-bearing (FWB), and improve muscular control.
Phase 3 (from week 2)
- Ideal criteria before progressing to this phase: Minimal discomfort, FWB, straight leg raise with no lag, range 0–100
- Goals: progress functional activities, prevent anterior knee pain, prevent scar adherence and joint stiffness, restore normal gait pattern, promote appropriate muscle strength, power and endurance, improve proprioception, maintain cardiovascular fitness, and encourage compliance with rehab.
Phase 3 (from week 6)
- Ideal criteria before progressing to this phase: Normal, symmetrical gait, full active ROM, no/minimal effusion, single leg squat (SLS) >80% parity, clam 10 reps with 10 s hold, and plank 30 s hold.
- Goals: Promote appropriate strength, power and endurance based on individual need, improve neuromuscular performance, and increase confidence.
Phase 4 (from week 12)
- Ideal criteria before progressing to this phase: SLS 60, 5 s hold with good alignment
- Goals: Sport specific function.
Phase 5 (from week 16)
- Ideal criteria before progressing to this phase: as phase 4
- Goals: Ongoing sport-specific function.
Phase 6 (from week 20)
- Ideal criteria before progressing to this phase: Tuck jump 60% quality or more, 5 RM >80% parity, and hop for distance >80% parity
- Goals: Prepare neuromuscular and psychological ability to return to unrestricted function.
Phase 7 (from week 24)
- Ideal criteria before progressing to this phase: all tests >90% parity
- Goals: Unrestricted confident function, injury prevention.
This case demonstrates that bilateral simultaneous ACL reconstruction is an effective management strategy in the skeletally immature. It reduced the number of inpatient hospital stays from 2 to 1 and facilitated a return to competitive sport at 11 months postoperatively, no different to the rehabilitation period for unilateral reconstruction. This relied on a physiotherapy service able to provide regular face-to-face contact, which may not be the case in other centers within the NHS. Further, research is required with greater numbers to draw any conclusions on complication rates.
This case demonstrates that bilateral simultaneous ACL reconstruction with the described technique is a viable treatment option in the adolescent patient. The patient returned to sport 11 months postoperatively, equivalent to quoted timeframe for a unilateral ACL rehabilitation.
References
- 1.Fabricant PD, Kocher MS. Anterior cruciate ligament injuries in children and adolescents. Orthop Clin North Am 2016;47:777-88. [Google Scholar | PubMed]
- 2.Yang XA, Vermeijden HD, O’Brien R, Van der List JP, Di Felice GS. Bilateral simultaneous anterior cruciate ligament tears treated with single staged simultaneous primary repair: A case report. Int J Surg Case Rep 2022;99:107670. [Google Scholar | PubMed]
- 3.Fabricant PD, Jones KJ, Delos D, Cordasco FA, Marx RG, Pearle AD, et al. Reconstruction of the anterior cruciate ligament in the skeletally immature athlete: A review of current concepts: AAOS exhibit selection. J Bone Joint Surg Am 2013;95:e28. Erratum in: J Bone Joint Surg Am 2013;95:e117. [Google Scholar | PubMed]
- 4.Nawabi DH, Mccarthy M, Graziano J, DeMille P, Chiaia TA, Green DW, et al. Return to play and clinical outcomes after all-inside, anterior cruciate ligament reconstruction in skeletally immature athletes. Orthop J Sports Med 2014;2: Vol: 7, Supp: 2. DOI: 10.1177/2325967114S00038 [Google Scholar | PubMed | CrossRef]
- 5.Maffulli N, Longo UG, Gougoulias N, Loppini M, Denaro V. Long-term health outcomes of youth sports injuries. Br J Sports Med 2010;44:21-5. [Google Scholar | PubMed]
- 6.Longo UG, Ciuffreda M, Casciaro C, Mannering N, Candela V, Salvatore G, et al. Anterior cruciate ligament reconstruction in skeletally immature patients: A systematic review. Bone Joint J 2017;99-B:1053-60. [Google Scholar | PubMed]
- 7.Yoo WJ, Kocher MS, Micheli LJ. Growth plate disturbance after transphyseal reconstruction of the anterior cruciate ligament in skeletally immature adolescent patients: An MR imaging study. J Pediatr Orthop 2011;31:691-6. [Google Scholar | PubMed]
- 8.Kocher MS, Smith JT, Zoric BJ, Lee B, Micheli LJ. Transphyseal anterior cruciate ligament reconstruction in skeletally immature pubescent adolescents. J Bone Joint Surg 2007;89-A:2632-9. [Google Scholar | PubMed]
- 9.Li S, Chen Y, Lin Z, Cui W, Zhao J, Su W. A systematic review of randomized controlled clinical trials comparing hamstring autografts versus bone-patellar tendon-bone autografts for the reconstruction of the anterior cruciate ligament. Arch Orthop Trauma Surg 2012;132:1287-97. [Google Scholar | PubMed]
- 10.Vaishya R, Esin AR, Agarwal AK, Vijay V. Bilateral simultaneous anterior cruciate ligament reconstruction: A case series and review of the literature. J Clin Orthop Trauma 2019;10:576-80. [Google Scholar | PubMed]
- 11.Lubowitz JH, Schwartzberg R, Smith P. Cortical suspensory button versus aperture interference screw fixation for knee anterior cruciate ligament soft-tissue allograft: A prospective, randomized controlled trial. J Arthrosc Relat Surg 2015;31:1733-9. [Google Scholar | PubMed]
- 12.Connaughton AJ, Geeslin AG, Uggen CW. All-inside ACL reconstruction: How does it compare to standard ACL reconstruction techniques? J Orthop 2017;14:241-6. [Google Scholar | PubMed]
- 13.Boyle MJ, Vovos TJ, Walker CG, Stabile KJ, Roth JM, Garrett WE Jr. Does adjustable-loop femoral cortical suspension loosen after anterior cruciate ligament reconstruction? A retrospective comparative study. Knee 2015;22:304-8. [Google Scholar | PubMed]
- 14.Graziano J, Chiaia T, De Mille P, Nawabi DH, Green DW, Cordasco FA. Return to sport for skeletally immature athletes after ACL reconstruction: Preventing a second injury using a quality of movement assessment and quantitative measures to address modifiable risk factors. Orthop J Sports Med 2017;5: PMID: 28451617. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 October 1, 2025 One-stage Anterior Cruciate Ligament Reconstruction with Medial Open Wedge High Tibial Osteotomy – A Surgical Technique
October 1, 2025 One-stage Anterior Cruciate Ligament Reconstruction with Medial Open Wedge High Tibial Osteotomy – A Surgical Technique October 10, 2023 Bilateral Non-traumatic Neglected Femoral Neck Fracture in a Healthy Adolescent: A Case Report and Review of Literature
October 10, 2023 Bilateral Non-traumatic Neglected Femoral Neck Fracture in a Healthy Adolescent: A Case Report and Review of Literature June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study
June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study June 1, 2026 Artelon Graft Augmentation in Revision Anterior Cruciate Ligament Reconstruction: Surgical Technique Guide
June 1, 2026 Artelon Graft Augmentation in Revision Anterior Cruciate Ligament Reconstruction: Surgical Technique Guide