
Surgical fixation is the most important intervention in Pipkin Type III fractures which are complex and rare presentation and can be time-driven as the patient might need either open reduction internal fixation or arthroplasty depending on femoral head vascularity.
Dr. Saiel A Kumarjuvekar, Department of Orthopedics, B.J. Government Medical College, Pune, Maharashtra, India. E-mail: kumarjuvekar@gmail.com
Abstract
Introduction: Femoral head fractures are relatively rare compared to other hip pathologies. Despite being infrequent, these fractures can give rise to various complications, even after a successful surgical fixation. To categorize these fractures, Pipkin introduced a classification system, distinguishing them into four types. Among these, Type III (31C.3) fractures are associated with femoral neck fractures and are notably less common, often leading to unfavorable outcomes.
Case Report: We present a case of a Type III Pipkin fracture in a 35-year-old male resulting from a road traffic accident. The patient underwent management with open reduction and internal fixation, utilizing headless compression screws and cancellous cannulated screws. Post-operative, the patient was instructed to remain non-weight bearing, and subsequent follow-ups were conducted to monitor for any potential complications.
Conclusion: Femoral head fractures are recognized for their complexity, with outcomes becoming even more diverse when associated with neck fractures. Effective pre-operative planning, coupled with timely reduction and fixation, plays a pivotal role in the management of these fractures.
Keywords: Pipkin, femoral head fracture, classification, complications, outcomes, surgical treatment.
Femoral head fractures are complex injuries at the hip joint, named after Sir Frank Jefferson Pipkin, who extensively studied them in 1957. The initial documented report of such fractures dates back to 1869 by Birkett [1]. Pipkin subsequently classified femoral head fractures into four types: Type I below the fovea, Type II above the fovea, Type III associated with a femur neck fracture alongside Type I or Type II, and Type IV associated with acetabular fractures [2]. Notably, Type III fractures demonstrate the poorest outcomes, as reported by the Orthopedic Trauma Association [3]. High-velocity motor vehicle accidents or falls from significant heights are common causes of femoral head fractures [4]. In this case report, we present an intriguing case of a patient sustaining a Type III Pipkin’s injury.
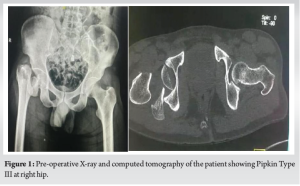
A 35-year-old male was involved in a road traffic accident, after which he experienced an inability to mobilize himself along with severe pain in his right hip. Upon arrival at the local hospital, a plain radiograph revealed a right hip intracapsular fracture with a femur head fracture suggestive of Pipkin Type III injury (Fig. 1). He was subsequently transferred to our center for further care, arriving 24 h after the injury. An urgent computed tomographic scan was performed, revealing a Pipkin Type III fracture of the right hip. On the same day, he underwent an open surgical dislocation of the hip and internal fixation of the femoral head and neck.
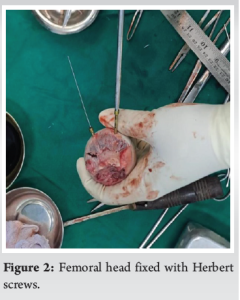
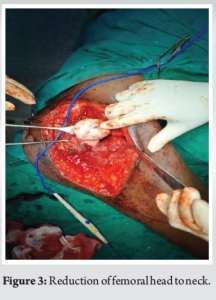
The surgical dislocation of the right hip was performed with the patient in a left lateral position using a standard posterior approach [5]. Upon reaching the fracture site, the fracture ran subfoveal, and the second fracture line corresponded to that seen in the computed tomography at the neck with the head being dislodged inferiorly and rotated. The head and fracture fragment were removed from the surgical field carefully. The femoral head was fixed with two 3.5 mm headless compression screws, while the neck was fixed with three 6.5 mm cancellous cannulated screws (Fig. 2 and 3).
Post-operative X-rays (Fig. 4) of the hip demonstrated a good reduction of the femoral head and neck. The patient was advised non-weight-bearing on the operated limb for 6 weeks, with a gradual increase in weight-bearing thereafter and eventual full weight-bearing status at 3-month post-surgery (Fig. 5, 6, 7), as tolerated by the patient.


Birkett initially reported femoral head fractures in case reports, after which Pipkin categorized them into four types. In Pipkin’s original series, only 3 out of 25 (12%) patients had a Type III fracture. The posterior approach to the hip is recommended by many experienced surgeons as it does not disrupt the blood supply to the femoral head [6,7]. Several studies have been conducted on Pipkin subtypes, indicating poor results and high complications, often requiring reoperations [8-10]. Scolaro et al. investigated a series of 147 Pipkin injuries, where all 13 Type III fractures underwent open reduction and internal fixation, later requiring revision to arthroplasty. In addition, 10% of Pipkin I, II, and IV cases ended up requiring arthroplasty [11]. Park et al. also noted the necessity for arthroplasty after closed reduction in Pipkin fractures [12]. Giannoudis et al. reported significant complications such as infection, avascular necrosis, and heterotrophic ossification. Scolaro et al. observed a 9% rate of avascular necrosis in their study [11]. Considering poorer functional outcomes compared to Type I and II fractures and a high risk of avascular necrosis, arthroplasty may be a preferable option over fixation in Type III fractures. However, the authors of this study acknowledge the importance of preserving the joint in younger patients, with arthroplasty being a more viable option for the elderly. There is limited evidence for the use of total hip replacement in treating Pipkin fractures in young individuals.
Femoral head fractures involving the neck present varied outcomes. Thorough pre-operative planning for surgical fixation is crucial. The timing of reduction and the selection of a surgical approach are both substantial factors influencing the ultimate outcomes and aiding in reducing the risk of complications. However, a deeper understanding of such situations requires extended and multicentric studies.
Despite the challenges of surgery, early intervention and meticulous surgical techniques are crucial to optimize outcomes and minimize the risk of complications, including avascular necrosis of the femoral head.
References
- 1.Birkett J. Description of a dislocation of the head of the femur, complicated with its fracture; with remarks. Med Chir Trans 1869;52:133-8. [Google Scholar | PubMed]
- 2.Pipkin G. Treatment of grade 4 fracture-dislocation of the hip. J Bone Joint Surg Am 1957;39:1027-42. [Google Scholar | PubMed]
- 3.Marsh JL, Slongo TF, Agel J, Broderick JS, Creevey W, DeCoster TA, et al. Fracture and dislocation classification compendium 2007: Orthopaedic trauma association classification, database and outcomes committee. J Orthop Trauma 2007;21 Suppl 10:S1-133. [Google Scholar | PubMed]
- 4.Giannoudis PV, Kontakis G, Christoforakis Z, Akula M, Tosounidis T, Koutras C. Management, complications and clinical results of femoral head fractures. Injury 2009;40:1245-51. [Google Scholar | PubMed]
- 5.Epstein HC, Wiss DA, Cozen L. Posterior fracture dislocation of the hip with fractures of the femoral head. Clin Orthop Relat Res 1985;201:9-17. [Google Scholar | PubMed]
- 6.Masse A, Aprato A, Alluto C, Favuto M, Ganz R. Surgical hip dislocation is a reliable approach for treatment of femoral head fractures. Clin Orthop Relat Res 2015;473:3744-51. [Google Scholar | PubMed]
- 7.Epstein HC. Posterior fracture-dislocations of the hip;long-term follow-up. J Bone Joint Surg Am 1974;56:1103-27. [Google Scholar | PubMed]
- 8.Bettinelli G, Placella G, Moharamzadeh D, Belluati A, Salini V. Articular femoral head fracture management: A meta-analysis of literature. Indian J Orthop 2021;55 Suppl 2:304-13. [Google Scholar | PubMed]
- 9.Engel JL, Johnsen P, Patel NK, Satpathy J, Mounasamy V. Pipkin type IV femoral head fractures: A case series and review of literature. Eur J Orthop Surg Traumatol 2021;31:791-5. [Google Scholar | PubMed]
- 10.Wang J, Cai L, Xie L, Chen H, Guo X, Yu K. 3D printing-based Ganz approach for treatment of femoral head fractures: A prospective analysis. J Orthop Surg Res 2019;14:338. [Google Scholar | PubMed]
- 11.Scolaro JA, Marecek G, Firoozabadi R, Krieg JC, Routt ML. Management and radiographic outcomes of femoral head fractures. J Orthop Traumatol 2017;18:235-41. [Google Scholar | PubMed]
- 12.Park KH, Kim JW, Oh CW, Kim JW, Oh JK, Kyung HS. A treatment strategy to avoid iatrogenic Pipkin Type 3 femoral head fracture-dislocations. Arch Orthop Trauma Surg 2016;136:1107-13. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Beyond Pipkin IV: Management of Femoral Head-neck Fracture-dislocation with Posterior Acetabular Wall and Peritrochanteric Fracture in an Adolescent Using a Modified Kocher-Langenbeck Approach
August 1, 2026 Beyond Pipkin IV: Management of Femoral Head-neck Fracture-dislocation with Posterior Acetabular Wall and Peritrochanteric Fracture in an Adolescent Using a Modified Kocher-Langenbeck Approach June 1, 2026 Bone Graft Harvesting Site Morbidity in Donor Area (Anterior Iliac Crest): A Retrospective Study
June 1, 2026 Bone Graft Harvesting Site Morbidity in Donor Area (Anterior Iliac Crest): A Retrospective Study December 1, 2025 Novel Technique for Extracting Metallic Debris from a Broken Reamer-Irrigator-Aspirator-2 Head within the Intramedullary Canal
December 1, 2025 Novel Technique for Extracting Metallic Debris from a Broken Reamer-Irrigator-Aspirator-2 Head within the Intramedullary Canal December 1, 2025 Revision of Cemented Reverse Total Shoulder Arthroplasty with Bone Graft in Osteogenesis Imperfecta: A Case Report
December 1, 2025 Revision of Cemented Reverse Total Shoulder Arthroplasty with Bone Graft in Osteogenesis Imperfecta: A Case Report