
Rare patterns of implant failure with proximal femoral nail require special surgical techniques and corticotomy for implant removal which highlight the importance of good pre-operative planning.
Dr. Ankit Dadra, Department of Orthopaedics, Postgraduate Institute of Medical Education and Research, Chandigarh, India. E-mail: ankitdadra@gmail.com
Abstract
Introduction: Delayed union, non-union, and unstable fixation can lead to fatigue fractures of orthopedic implants. Breakages typically occur at the fracture site or locking screw insertion, acting as stress concentration foci. This case report highlights a rare instance of a 3-part broken proximal femoral nail (PFN), extracted using a corticotomy-assisted method without knee joint violation.
Case Report: A 45-year-old male patient with a subtrochanteric femur fracture, initially fixed with a short PFN, presented with non-union and a broken implant a year post-surgery. Radiographs revealed breakage at two sites, creating three nail pieces. During revision surgery, the proximal nail part was removed through standard extraction. The middle fragment was accessed and removed at the fracture site, and the distal part was extracted through a lateral cortical window using a beaded guidewire in a retrograde fashion, avoiding the knee joint. A long PFNA was subsequently inserted, and bone grafting was performed.
Conclusion: This case underscores a rare PFN failure pattern, with fractures at three sites. The corticotomy-assisted extraction technique preserved medullary canal integrity, minimized tissue damage, and maintained biomechanical stability. This approach offers a viable alternative to traditional methods, reducing complications and improving surgical outcomes.
Keywords: Proximal femoral nail, Implant breakage, Corticotomy-assisted extraction, Intramedullary nail, Guidewire.
Delayed union, non-union and unstable fixation can lead to fatigue fracture of an orthopedic implant [1]; an intramedullary nail usually breaks at the fracture site [2] or at the locking screw insertion site, which acts as foci of stress concentration [3]. Late failure may be due to the mechanical properties of the nail or bad surgical technique; the nail can break at more than one site. Several techniques for the removal of a broken nail have been described; devices such as extraction hooks and olive wire (beaded guidewire) have been developed for extraction of the distal fragment of the broken nail, which cannot be accessed from the fracture site and requires access to the knee joint [4]. The present case highlights a rare scenario where the authors extracted a broken 3-part proximal femoral nail (PFN), along with one broken proximal locking screw, by a corticotomy-assisted method of extraction of the distal part, without violating the knee joint.
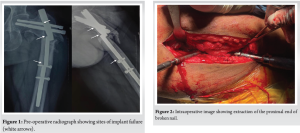
A 45-year-old male patient with a history of a fall from stairs in March 2022 was diagnosed with a subtrochanteric femur fracture which was subsequently fixed using a short PFN in a peripheral hospital. One year later, the patient developed pain in the ipsilateral thigh after which he could not ambulate. He presented to our advanced trauma center with pain and difficulty in ambulation. Fresh radiology revealed a non-union of the fracture and a broken implant (Fig. 1). The peculiarity of this broken implant was that it had failed at two sites, proximally at the fracture site and distally at the proximal locking bolt, with three nail pieces. The patient was planned for implant removal with exchange nailing and bone grafting.
Surgical technique
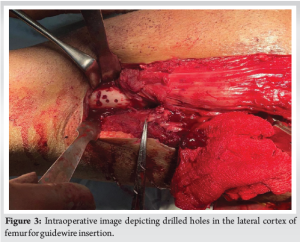
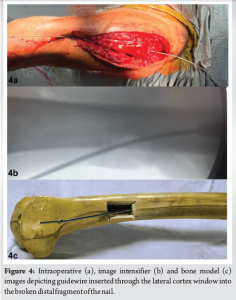
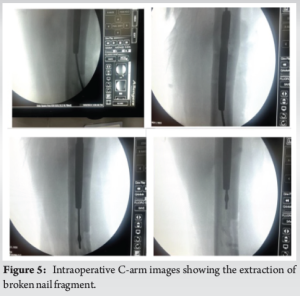
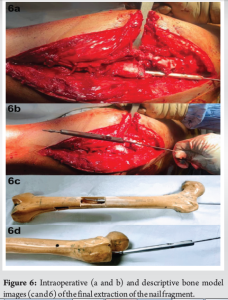
The patient was positioned supine on the fracture table. Incisions were given over the previous scar mark and the fracture site. The proximal part of the nail was removed from the insertion site after removal of neck screws; the broken distal end of the proximal screw was left in situ (Fig. 2). The fracture site was freshened and the proximal end of the middle fragment of the broken nail was seen in the distal bone fragment. It was removed from the fracture site using a plier. The distal locking screws were then removed. A 10 mm × 20 mm lateral cortical was created distal to the nail using multiple drill holes and a burr to pass a beaded guidewire in a retrograde fashion. Since the window was unicortical and the nail would cross the corticotomy site, it would be structurally stable (Fig. 3). The guidewire was chosen such that the bead had a diameter larger than the canal of the nail to engage in it; it could not be too big or else a larger cortical window would have been needed. The guidewire was passed through the distal fragment in a retrograde fashion (Fig. 4). It was then held with a plier and back hammered to extract the distal part of the nail (Fig. 5 and 6). The complete removal of the implant was confirmed using image intensifier guidance, except for the distal part of the broken screw in the femoral head (Fig. 7).
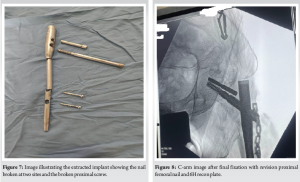
Sequential reaming was performed and a long PFNA was then inserted after the fracture was reduced and held with a bone holder. A 6-hole reconstruction plate with unicortical locking screws was used to hold the reduction before reaming and nail insertion (Fig. 8). Bone grafting was done using autograft from the ipsilateral iliac crest. The wound was washed and closed in layers. The surgical duration was approximately 2 h.
Intramedullary nail breakage, although rare, is a known complication, especially in cases of delayed or non-union, when the patient starts weight-bearing. In such a scenario nail instead of being a load-sharing device acts as a load-bearing device and ultimately breaks [5]. Removal of the proximal broken fragment is relatively straightforward with universal extractors consisting of threaded conical bolts, which can engage with the proximal end of the nail and then back hammered out of the bone. In a 2-part broken nail, the distal part can be accessed from the fracture site and extracted; however, if the nail breaks at two or more sites, the distal part of the nail is inaccessible from the fracture site. For extracting this distal part, several techniques have been described in the literature [1-4,6-8]. The hook method employs a long hook inserted through or along the nail to engage with the nail at the distal end to pull it out. However, the hook can slip from the nail and may require multiple attempts for re-insertions [9]. In addition, it cannot be used in thin nails or passed through if there is bony ingrowth into the canal [10]. In long nails also its value is limited and it is more suited for extraction of short nails. Georgilas et al. [3] reported a method of nail removal using antegrade sequential reaming over a guidewire until the reamer engages into the implant. While it has the advantage of causing no damage to the medullary canal, it damages the reamer and mostly renders it unusable. Karladani [11] used a screw through the locking hole, to lock a plain guidewire after inserting it through the nail and then back hammering it to remove the broken nail. Using a concept similar to this, Lee and Yang [12] used a 10 mm K-wire to lock the guidewire in place. However, antegrade guidewire insertion is not easy if the nail is broken at two sites. Locking the guidewire is technically challenging and may require multiple attempts, increased operative time and radiation exposure. Magu et al. [4] described the technique of retrograde insertion of a ball-tipped guidewire through the knee joint loaded with a 7 mm washer. The washer engages on the distal tip of the nail, which can be used to hammer out the nail. The disadvantage of this method is that it violates the knee joint and creates an osteochondral defect distal to the nail. In comparison to this, our technique is relatively less invasive as it does not require an arthrotomy. It is also biomechanically stable since the longer nail bypasses the lateral cortical window. The medullary canal and the blood supply are not damaged and there is no risk of any implant falling distally into the medullary canal.
This case report highlights a rare failure pattern of a PFN, where the implant fractured at three sites, presenting a challenging extraction scenario during revision surgery. The method involves corticotomy-assisted extraction of the distal nail fragment through a lateral cortical window, preserving medullary canal integrity and minimizing tissue damage. It also ensures biomechanical stability and reduces the risk of complications associated with other methods.
Corticotomy-assisted extraction of a broken 3-part PFN can effectively preserve medullary canal integrity and minimize tissue damage, providing a viable alternative to more invasive traditional methods.
References
- 1.Brewster NT, Ashcroft GP, Scotland TR. Extraction of broken intramedullary nails--an improvement in technique. Injury 1995;26:286. [Google Scholar | PubMed]
- 2.Poehling GG, Webb LX. Retrieval and replacement of a broken Küntscher rod by a closed technique. Technical note. J Bone Joint Surg Am 1982;64:1389-90. [Google Scholar | PubMed]
- 3.Georgilas I, Mouzopoulos G, Neila C, Morakis E, Tzurbakis M. Removal of broken distal intramedullary nail with a simple method: A case report. Arch Orthop Trauma Surg 2009;129:203-5. [Google Scholar | PubMed]
- 4.Magu NK, Sharma AK, Singh R. Extraction of the broken intramedullary femoral nail--an innovative technique. Injury 2004;35:1322-3. [Google Scholar | PubMed]
- 5.Johnson NA, Uzoigwe C, Venkatesan M, Burgula V, Kulkarni A, Davison JN, et al. Risk factors for intramedullary nail breakage in proximal femoral fractures: A 10-year retrospective review. Ann R Coll Surg Engl 2017;99:145-50. [Google Scholar | PubMed]
- 6.Kim DS, Kwon CS, Ahn JK, Jeong BH, Sung YB, Yum JK. Simple method for the extraction of the broken intramedullary nail of femur: Case report. J Korean Orthop Assoc 2018;34:1171-4. [Google Scholar | PubMed]
- 7.Man CH, Bae MW. Method for removing broken proximal femoral nails using existing screw hole. Acta Ortop Bras 2018;26:72-4. [Google Scholar | PubMed]
- 8.Franklin JL, Winquist RA, Benirschke SK, Hansen ST Jr. Broken intramedullary nails. J Bone Joint Surg Am 1988;70:1463-71. [Google Scholar | PubMed]
- 9.Acharya M, Alani A, Almedghio S. The fish hook technique of extracting broken intramedullary nails. Acta Orthop Belg 2008;74:686-8. [Google Scholar | PubMed]
- 10.Roman MD, Fleaca SR, Mohor CI, Bacila C, Bratu D, Teodoru A, et al. Extraction of broken interlocking tibial nails: A review of surgical techniques and practical management. Appl Sci 2023;13:1645. [Google Scholar | PubMed]
- 11.Karladani AH. Removal of a broken nail using a guide wire and a screw. Acta Orthop 2006;77:986-8. [Google Scholar | PubMed]
- 12.Lee M, Yang KH. Removal of a broken intramedullary nail with a narrow hollow using a bulb-tipped guide wire and Kirschner wire - A case report. J Korean Fract Soc 2010;23:377-81. [Google Scholar | PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Management of Infected Non-union of Long Bones Using Antibiotic Cement-Coated Intramedullary Nails: A Prospective Case Series
August 1, 2026 Management of Infected Non-union of Long Bones Using Antibiotic Cement-Coated Intramedullary Nails: A Prospective Case Series August 1, 2026 Augmentation Plating with Intramedullary Nailing for Aseptic Long Bone Non-union: A Prospective Observational Study of Clinical, Radiological, and Functional Outcomes
August 1, 2026 Augmentation Plating with Intramedullary Nailing for Aseptic Long Bone Non-union: A Prospective Observational Study of Clinical, Radiological, and Functional Outcomes August 1, 2026 Radiological Outcomes of Reamed Short Proximal Femoral Nailing in Intertrochanteric Fractures in Patients Aged 50 Years and Above
August 1, 2026 Radiological Outcomes of Reamed Short Proximal Femoral Nailing in Intertrochanteric Fractures in Patients Aged 50 Years and Above August 1, 2026 Evaluation of Orthopedic Outcomes of Proximal Femoral Nailing for Intertrochanteric Fractures and Predictive Value of Pre-operative Glycemic Status, Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio: A Prospective Study
August 1, 2026 Evaluation of Orthopedic Outcomes of Proximal Femoral Nailing for Intertrochanteric Fractures and Predictive Value of Pre-operative Glycemic Status, Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio: A Prospective Study