
In the case of comminuted fracture of olecranon, Fragment-specific plate fixation is a good alternative to tension band wiring as fixation using plates helps to maintain ulnar length and provides good stability.
Dr. Rishabh Aggarwal, Department of Orthopaedics, Dr. D.Y. Patil Medical College and Hospital, Pimpri-Chinchwad, Pune, Maharashtra, India. E-mail: rishabhaggarwal98@gmail.com
Abstract
Introduction: Olecranon fractures account for 5–7% of elbow fractures, making them a common injury. The majority of these fractures are treated surgically because they are intra-articular and can disrupt the elbow extensor mechanism. Mayo Type II fractures are displaced with a stable ulnohumeral joint, indicating intact ligamentous structures, particularly the anterior portion of the medial collateral ligament.
Case Report: In our case report, a male in his 20’s came to the outpatient department with complaints of pain in the right elbow since 1 day following a fall from a bike. He also reported that he was unable to fully extend his right elbow. After a plain radiograph, a right displaced comminuted olecranon fracture was suggested. He underwent a pre-anesthesia checkup and standard laboratory testing before being taken for surgery. Open reduction internal fixation with fragment-specific plates was done. An above-elbow slab in the extended position was applied post-surgery and continued for 14 days. Elbow range of motion physiotherapy was started in accordance with tolerance, and the patient responded favorably to surgery.
Conclusion: To effectively categorize olecranon fractures according to displacement, comminution, and stability, the Mayo classification was developed. With appropriate computed tomography scan imaging and pre-operative planning, individual fragments of these comminuted fractures can be delineated, and fragment-specific implants can be used, resulting in good radiological and clinical outcome with minimal complications as compared to tension band wiring.
Keywords: Olecranon fracture, fragment-specific plate fixation, elbow trauma, absolute fixation, mayo classification.
Injury to the olecranon is relatively frequent. Although much less common in minors, it accounts for 5–7% of elbow fractures in adults [1]. Its subcutaneous location makes it susceptible to direct trauma, which typically results from a direct impact to the elbow’s point or a fall onto an extended arm [2]. Strong biceps contractions against a fixed ulna can also result in olecranon fractures. Simple non-displaced fractures or complicated fractures involving elbow joint dislocation are both possible. Intact ligamentous structures, especially the anterior part of the medial collateral ligament, are indicated by the displacement of Mayo Type II fractures with a stable ulnohumeral joint [3,4]. Plain radiographs are typically adequate to confirm the diagnosis and formulate a management strategy. In some circumstances, a computed tomography (CT) scan may be necessary to evaluate the injury’s seriousness and determine a fixation strategy. The gold standard of care for comminuted fractures, Monteggia fractures, fractures accompanied by dislocations, and oblique fractures with distal extension impacting the coronoid is fixation with plates and screws [5]. With surgical fixation, a good recovery is expected, though the final result may be influenced by the extent of the soft-tissue damage, the presence of multiple fracture fragments, and the intra-articular nature of the injury. In our case report, we have treated a Mayo type IIB olecranon fracture with open reduction internal fixation with fragment-specific plates.
Case presentation
A male in his 20’s complained of right elbow pain and movement restrictions for 1 day when he visited the outpatient department. Before going to the hospital, he appeared to be in good health. However, the day before, he fell off his bike, and as a result, he experienced an acute onset, continuous, aching, moderately severe elbow pain that was exacerbated by movement and alleviated by immobilization, rest, and analgesics. On examination of the right elbow, there was tenderness, swelling, and restriction of movements. Active flexion was possible up to 30°.
Investigations
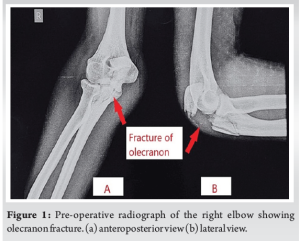
The right elbow’s displaced comminuted olecranon fracture was identified by a normal radiograph as shown in (Fig. 1).
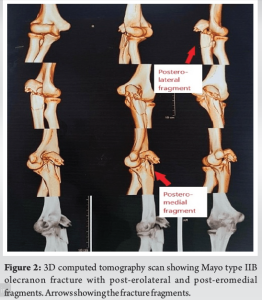
A 3D CT scan was done for better delineation of the fracture fragments as shown in (Fig. 2).
Treatment
The surgical procedure was done after routine laboratory investigations and pre-anesthesia checkup under general anesthesia with the patient in the left lateral position. After exsanguination, the upper limb tourniquet was inflated to 220 mm of Hg. A 15 cm incision was made over the posterior aspect of the right elbow via the lateral paraolecranon approach as shown in (Fig. 3). The ulnar nerve was identified and protected throughout the surgery. After elevating the triceps, the fracture site and post-erolateral and post-eromedial fragments were identified. The fracture was reduced using pointed reduction forceps and two 2.7 mm L plates were used to fix the post-eromedial and post-erolateral fragments using locking and cortical screws as shown in (Fig. 4). Final reduction was checked using fluoroscopic guidance and closure was done in layers.

Outcome and follow-up
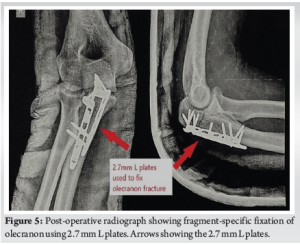
An acceptable fracture reduction was visible on a post-operative radiograph as shown in (Fig. 5). Elbow range of motion was started on post-operative day 2 as per patient tolerance.
On follow-up at 2 months, the patient had full range of motion of the elbow with no complaints.
Olecranon fractures frequently affect the elbow’s articular surface. In 20% of instances, post-traumatic arthritis develops, and this result is linked to chronic malreduction of >2 mm of the articular surface [6]. Accidental malreduction by reducing the larger sigmoid notch in fractures with considerable comminution may increase the patient’s risk for developing arthritis [7]. For unstable fracture patterns with significant comminution, a fracture line exiting distal to the semilunar notch (Mayo type IIB), and fracture-dislocations (Mayo type III), plate and screw fixation is advised [8]. Fragment plate fixation is designed to minimize subcutaneous plate prominence without sacrificing stability, thus decreasing the rate of symptomatic implants and potentially the need for implant removal. Mini-fragment fixation has also been found to be a viable alternative in clavicle, talar neck, and tibial plafond fractures [9,10]. Fracture stabilization with mini-fragment plates in comminuted fractures involving multiple fragments is linked to a decreased incidence of symptomatic implants, whereas there is no discernible difference in terms of post-operative complications or reoperations [8].
In order to effectively categorize olecranon fractures according to displacement, comminution, and stability, the Mayo classification was developed. With appropriate CT scan imaging and pre-operative planning, individual fragments of these comminuted fractures can be delineated, and fragment specific implants can be used, producing a favourable radiological and clinical result with minimal complications.
Fragment specific implants can be used in comminuted olecranon fracrures for favourable radiological and clinical result with minimal complications. In case of comminuted fracture, fixation using plates helps to maintain ulnar length and provides good stability as compared to tension band wiring.
References
- 1.Sullivan CW, Herron T, Hayat Z. Olecranon fracture. In: StatPearls. Treasure Island: StatPearls Publishing; 2023. [Google Scholar | PubMed]
- 2.Wiegand L, Bernstein J, Ahn J. Fractures in brief: Olecranon fractures. Clin Orthop Relat Res 2012;470:3637-41. [Google Scholar | PubMed]
- 3.Sullivan CW, Desai K. Classifications in brief: Mayo classification of olecranon fractures. Clin Orthop Relat Res 2019;477:908-10. [Google Scholar | PubMed]
- 4.Torres SJ, Limpisvasti O. Ulnar collateral ligament repair of the elbow-biomechanics, indications, and outcomes. Curr Rev Musculoskelet Med 2021;14:168-73. [Google Scholar | PubMed]
- 5.Johnson NP, Silberman M. Monteggia fractures. In: StatPearls. Treasure Island: StatPearls Publishing; 2023. [Google Scholar | PubMed]
- 6.Meulenkamp B, Martin R, Desy NM, Duffy P, Korley R, Puloski S, et al. Incidence, risk factors, and location of articular malreductions of the tibial plateau. J Orthop Trauma 2017;31:146-50. [Google Scholar | PubMed]
- 7.Lee SH, Kim MB, Lee YH, Kang HJ. Reduction of olecranon fractures with no or minimal dorsal cortex comminution based on the contour of the posterior ulnar cortex: Does it restore the greater sigmoid notch? Arch Orthop Trauma Surg 2022;142:2215-24. [Google Scholar | PubMed]
- 8.Wadhwa H, Oquendo YA, Goodnough LH, DeBaun MR, Bishop JA, Gardner MJ. Mini-fragment plating of olecranon fractures is comparable to precontoured small-fragment plating. J Orthop 2022;11:41-5. [Google Scholar | PubMed]
- 9.Maceroli MA, Wong C, Sanders RW, Ketz JP. Treatment of comminuted talar neck fractures with use of minifragment plating. J Orthop Trauma 2016;30:572-8. [Google Scholar | PubMed]
- 10.Dang KH, Ornell SS, Huynh RA, DeLeon JC, Pesek R, Karia RA. Early clinical and radiographic outcomes of a mini-fragment, low profile plating system in tibial plafond fractures. Injury 2019;50:1773-80. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Isolated Humeral Trochlear Fracture without Associated Elbow Injury: A Rare Case Report
July 1, 2026 Isolated Humeral Trochlear Fracture without Associated Elbow Injury: A Rare Case Report September 29, 2019 An Unusual Cause of Buttock Pain after Posterior Thoracolumbar Fixation: Rod Migration into the Pelvis
September 29, 2019 An Unusual Cause of Buttock Pain after Posterior Thoracolumbar Fixation: Rod Migration into the Pelvis October 1, 2025 A Rare Clinical Dilemma: Humeral Shaft Fracture in a Full-Term Pregnant Patient – A Case Report with Review of Literature
October 1, 2025 A Rare Clinical Dilemma: Humeral Shaft Fracture in a Full-Term Pregnant Patient – A Case Report with Review of Literature September 1, 2025 Triple-Segmental Shaft Femur Fracture: A Case Report
September 1, 2025 Triple-Segmental Shaft Femur Fracture: A Case Report