
Open ankle injuries require extensive assessment as static radiographs may not show the full extent of injury and repairment using non-absorbable suture and suture anchor augmentation is a viable option.
Mr. Braden Womack, Department of Orthopaedics, University of Toledo Medical Center, Ohio, USA. E-mail: bwomack2@rockets.utoledo.edu
Abstract
Introduction: Bony and ligamentous ankle injuries are some of the most commonly treated injuries by orthopedic surgeons. Open ligamentous ankle injuries without an associated fracture or dislocation are rare and to our knowledge have only sparsely been described in the literature. We present a case and successful treatment of an open lateral ankle injury with capsular rupture and ligamentous damage without fracture or dislocation in a 22-year-old female. Due to the rarity of this injury, there is not a standard treatment protocol.
Case Report: A 22-year-old female presenting presented with an open ankle injury while playing volleyball after a sudden varus and inversion force. An xX-ray obtained at an outside hospital showed no acute fracture or dislocation of the ankle joint. In the operating room, stress examinations showed a positive anterior drawer and a positive varus stress test. Heavy non-absorbable suture was used to repair the ruptured ligaments with the ankle capsule. Augmentation of the repair was performed with a suture anchor placed in the lateral aspect of the distal fibula. Subsequently at 6-months post -operative the patient returned to full weight -bearing and radiographs showed maintenance of ankle alignment with no radiographic or clinical signs of instability.
Conclusion: Open ankle injuries without dislocation or fracture are very rare. Therefore, an ample assessment should always be conducted with an understanding that the extent of the injury may be underestimated via static radiographs. Surgical repair is necessary for treatment and we have described one technique through which treatment of open lateral ligamentous ankle injury is possible.
Keywords: Open ankle injury, ankle, ankle injury, dislocation, fracture, surgical management.
Ankle injuries are common with the lateral ligament complex of the ankle being the single most injured structure of the body [1]. Oftentimes, these injuries are limited to the anterior talofibular ligament (ATFL) and occur without disrupting the skin [1,2]. While these injuries make up the majority seen to the lateral ankle, there are also instances of open ankle injuries with and without dislocation described in the literature. Open ankle injuries without fracture often require a high-energy trauma involving excessive inversion due to the strength and stability of the joint [3]. Although rare, understanding the mechanism, risk factors, and treatment of these injuries is important to help prevent complications such as chronic pain, joint instability, and potential neurovascular injuries [4]. We aim to provide an in-depth description and fluoroscopic examination of an open lateral ankle injury with ligamentous and capsular rupture without an associated fracture or dislocation demonstrating the unique characteristics of the injury and providing approaches to guiding management.
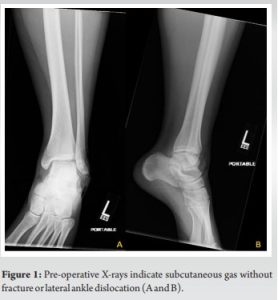
A 22-year-old female presented to the emergency department due to an ankle injury suffered while playing volleyball. The injury occurred on impact from a jump resulting in a sudden varus force and inversion injury to the ankle. This resulted in a 7 × 5 cm open wound overlying the lateral malleolus with exposed bone. On presentation, there was extrusion of the distal fibula through her skin with invagination of skin distal to the tip of the fibula. The patient was neurovascularly intact. An x-ray obtained at an outside hospital showed no acute fracture or dislocation of the ankle joint. The ankle mortise was well preserved on initial imaging (Fig. 1). The patient presented to our institution on the day of the injury and was subsequently taken urgently to the operating room. Antibiotics were initiated before transfer to our institution and preoperatively.
During the operation, an extension of the open traumatic arthrotomy was performed distally to gain exposure to the tibiotalar joint. It was noted that the ATFL, calcaneofibular ligament (CFL), posterior talofibular ligament (PTFL) and the lateral ankle capsule were torn with the talus readily visible. Once exposure was completed, stress examinations were performed showing a negative external rotation stress test but a positive anterior drawer and a positive varus stress test (Fig. 2).

The joint was then thoroughly examined, irrigated, and debrided. There were no osseous or chondral injuries. The ruptured ligaments with the ankle capsule were then approximated and repaired with a heavy non-absorbable suture. Augmentation of the repair was performed with a suture anchor placed in the lateral aspect of the distal fibula. One limb of the anchor was started posteriorly and run along the distal and anterior aspect of the traumatic arthrotomy to reinforce the repair. The other suture was used to further reinforce the repair (Fig. 3). Repeat stress examination of the ankle now demonstrated no residual instability with varus tilt or anterior drawer tests. The wound was closed in a standard layered fashion. A soft sterile dressing and a posterior splint were then applied. She was instructed to remain non-weight-bearing following surgery.

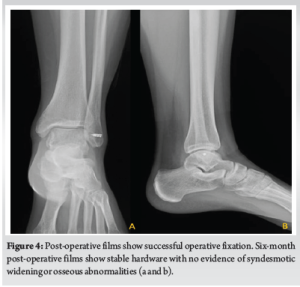
At her 2-week post-operative visit, she was transitioned into a short leg cast and remained non-weight-bearing. At her 6-week post-operative visit, the patient was transitioned to a CAM boot. to allow for ankle range of motion. She remained non-weight-bearing and began physical therapy. At 10 weeks postoperatively, the patient progressed to weight-bearing as tolerated and continued physical therapy. By her 6-month visit, the patient returned to full weight-bearing without post-operative complications. Radiographs showed maintenance of ankle alignment with no radiographic or clinical signs of instability (Fig. 4).
The ankle joint is formed by the distal tibia, fibula, and talus which are stabilized by ligamentous complexes: The tibiofibular syndesmosis (anteroinferior tibiofibular, posteroinferior tibiofibular, and the interosseous tibiofibular ligament), the medial collateral ligaments (superficial and deep deltoid) and the lateral collateral ligaments (anterior talofibular, calcaneofibular, and the PTFL). Given its anatomic location, the ATFL is the main lateral stabilizer of the ankle joint limiting both anterior translation and internal rotation of the talus [5]. Pure ATFL injuries are the most common lower ankle injuries, while ATFL and CFL dual injuries are the second most common [6]. The CFL is rarely injured in isolation because it works in concert with the ATFL to prevent inversion of the ankle; increasing the amount of force the lateral collateral ligaments can withstand [7]. However, a pure ligamentous dislocation has been found to occur with various mechanisms. The most common injury pattern occurs when the ankle is maximally plantar flexed with an axial load combined with forced inversion of the foot. This allows injuries of the ATFL and CFLs leading to a posteromedial dislocation [8]. When recreated by Fernandes in cadaveric studies, it was observed that this injury mechanism can also result in pure medial or lateral dislocation with compromise of the ATFL and CFLs [8]. Although it is more common to observe posteromedial dislocations with ligamentous damage, to the best of our knowledge only a limited number of cases have been published describing a lateral open ligamentous disruption without associated fracture or dislocation. Of these cases, Bryant et al. reported two cases of lateral collateral ligament injuries after extreme inversion during rock climbing, suggesting rock-climbing shoes can cause increased stress on the lateral ligament and capsule, resulting in open injury [9]. Carter et al. and Chun et al. reported instances where similar injuries occurred in basketball players causing complete ligamentous rupture of the ATFL, CFL, and PTFL [2,10]. Thompson et al. described a severe inversion injury needing surgical repair [11]. In these cases, the degree of instability caused by the injury is not well documented, making it difficult to understand the full extent of the injury. As one can see in our case, a complete rupture of the lateral ankle ligaments and ankle capsule can cause significant instability within the ankle that may not be evident on static ankle imaging (Fig. 2). Due to the rarity of this injury, there is no standard treatment protocol. For instance, there have been examples of using external fixation for immobilization due to extensive destruction and stretching of the capsule as described in Carter et al. [10]. Bryant et al. and Chun et al. had success utilizing surgical repair in which they used sutures to repair the damaged ligaments and capsule for restoration of function, which lead to a high rate of return to pre-injury level [2,10,12]. In our case, we demonstrate successful management of this rare open lateral ankle injury without dislocation using non-absorbable suture and suture anchor augmentation to repair the lateral ankle ligaments and capsule, restoring ankle joint stability.
Open ankle injuries with disruption of the lateral ligamentous complex and capsule without fracture or dislocation are very rare injuries. Therefore, an ample assessment should always be conducted with an understanding that the extent of the injury may be underestimated through static radiographs in patients presenting with an open ankle wound. After a diagnosis is made, prompt surgical exploration and examination are needed to understand the full extent of the injury before repair of the injured ligaments is performed. We have described one technique through which treatment of open lateral ligamentous ankle injury is possible.
Open ankle injuries without fracture or dislocation are rare. There is no standardized approach to assessment and treatment. Given this, we hope to outline that prompt surgical exploration and examination are needed to truly understand the extent of the injury. In our case, primary suture repair with suture augmentation was preformed.
References
- 1.Funk JR. Ankle injury mechanisms: Lessons learned from cadaveric studies. Clin Anat 2011;24:350-61. [Google Scholar | PubMed]
- 2.Chun D, Kim J, Won SH, Yi Y, Kim Y, Cho J. Open ligamentous complex disruption of the lateral ankle without dislocation or fracture. Medicine (Baltimore) 2019;98:e17447. [Google Scholar | PubMed]
- 3.Wight LJ, Owen D, Goldbloom D, Knupp M. Pure ankle dislocation: A systematic review of the literature and estimation of incidence. Injury 2017;48:2027-34. [Google Scholar | PubMed]
- 4.Mustafa MM, Altayeb AA, Mohamed AA, Mohamed AA, Abdalla EM. Open ankle dislocation without associated malleolar fracture: Case report. J Orthop Clin Res 2023;1:103-11. [Google Scholar | PubMed]
- 5.Golanó P, Dalmau-Pastor M, Vega J, Batista J. Anatomy of the ankle. In: Sports et Traumatologie. Paris: Springer; 2014. p. 1-24. [Google Scholar | PubMed]
- 6.Rigby R, Cottom JM, Rozin R. Isolated calcaneofibular ligament injury: A report of two cases. J Foot Ankle Surg 2015;54:487-9. [Google Scholar | PubMed]
- 7.Hunt KJ, Pereira H, Kelley J, Anderson N, Fuld R, Baldini T, et al. The role of calcaneofibular ligament injury in ankle instability: Implications for surgical management. Am J Sports Med 2019;47:431-7. [Google Scholar | PubMed]
- 8.Frank AL, Charette RS, Groen K. Ankle dislocation. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/nbk554610/# [Google Scholar | PubMed]
- 9.Bryant R, Clubb S, Jones S, Bostock SH. Open lateral ligament injuries of the ankle and rock climbing. Foot 2001;11:89-90. [Google Scholar | PubMed]
- 10.Carter CT, Schroerlucke SR, Rosenblum WJ, Martell JR. Open ligamentous disruption of the lateral aspect of the ankle without associated fracture or dislocation: A case report. JBJS Case Connect 2013;3:e19. [Google Scholar | PubMed]
- 11.Thompson TL, Muhammad K. Open rupture of the lateral ligaments of the ankle without dislocation: A case report. Am J Orthop (Belle Mead NJ) 2006;35:240-1. [Google Scholar | PubMed]
- 12.Hembree WC, Tsai MA, Parks BG, Miller SD. Comparison of Suture-based anchors and traditional bioabsorbable anchors in foot and ankle surgery. J Foot Ankle Surg 2017;56:3-7. [Google Scholar | PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 10, 2024 Management of Bilateral Posterior Sternoclavicular Joint Dislocation: A Case Report
July 10, 2024 Management of Bilateral Posterior Sternoclavicular Joint Dislocation: A Case Report April 10, 2024 Terrible Triad of the Elbow with Ipsilateral Complete Triceps Tearing, Distal Radius and Scaphoid Waist Fracture: A Case Report
April 10, 2024 Terrible Triad of the Elbow with Ipsilateral Complete Triceps Tearing, Distal Radius and Scaphoid Waist Fracture: A Case Report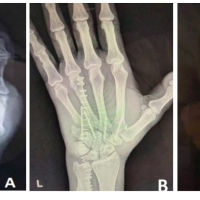 December 10, 2022 Analysis of Functional Outcomes Following Surgical Management of Neglected Multiple Carpometacarpal Dislocations: A Series of 4 four Cases and Review of Literature
December 10, 2022 Analysis of Functional Outcomes Following Surgical Management of Neglected Multiple Carpometacarpal Dislocations: A Series of 4 four Cases and Review of Literature May 1, 2026 “No Traction” Technique: A Novel, Simple, Easy, and Ergonomic Manoeuvre to Reduce Posterior Dislocation of the Hip Joint – A Case Report
May 1, 2026 “No Traction” Technique: A Novel, Simple, Easy, and Ergonomic Manoeuvre to Reduce Posterior Dislocation of the Hip Joint – A Case Report