
Fracture window technique can be an apt approach to deal with coronal shear fractures around the elbow joint.
Dr. Kaustav Mukherjee, Department of Orthopedics, Kalyani Institute of Medical Science, Burdwan, West Bengal, 713104, India. E-mail: kaustavm.1992@gmail.com
Abstract
Introduction: Coronal shear injuries are a rare subgroup of elbow fractures. Fractures involving the capitellum, lateral condyle, and olecranon are a rare triad, presenting as a result of very specific trauma mechanism and often challenging to treat. Addressing all these fragments often entails surgeons resorting to more than one approach to adequately fix the fractures.
Case Report: An elderly lady presented with a history of a slip and fall at home on flexed elbow. Radiographs revealed a unique fracture pattern with involvement of capitellum, olecranon, and lateral condyle. A single standard posterior approach to elbow and dual fracture window technique was utilized to fix the fragments sequentially, with capitellum fixed in posteroanterior fashion with headless compression screw. Lateral condyle and olecranon were fixed appropriately in sequence. Initial postoperative immobilization for 2 weeks was followed by gradual elbow movements as tolerated. A good functional and radiological outcome was recorded at the end of the final follow-up.
Conclusion: A single incision posterior approach, utilizing the dual fracture window, can be an effective way to fix all fracture fragments in a single approach for coronal shear elbow fractures.
Keyword: Coronal shear injury, elbow, rare fracture triad.
Elbow coronal shear injuries are a rare subgroup of fractures affecting the distal humerus and account for <1% of all fractures around the elbow [1-3]. Capitellum remains the most commonly fractured anatomical structure, ranging from a simple large fragment to gross comminution, with fractures often extending into the trochlea [2]. Involvement of ligamentous structures (lateral collateral ligament in 30% of cases) and radial head fractures (in almost 40% of cases) are also well documented in literature [4-6]. Patho-mechanism of such injuries involves axial loading on a flexed elbow, which transmits force onto the capitello-trochlear area by force transmission through the radial head [2,3]. This mechanism holds true for majority of the fractures in young individuals with good bone stock, but in elderly osteoporotic individuals, force transmission from the point of impact often propagates long enough to present with varied fracture components, which become challenging to treat. We report a unique case of an elbow fracture with involvement of the capitellum, lateral condyle, and olecranon. To the best of our knowledge, no such fracture triad has been reported in literature till date. We aim to discuss the challenges in operative planning, the importance of a single approach to deal with all the fracture components, and the pathomechanism behind this relatively rare fracture pattern.
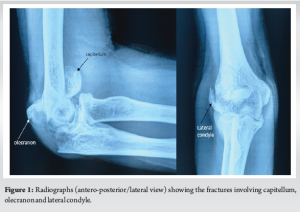
A 65-year-old woman, from a poor socioeconomic background, presented to the outpatient department with pain and swelling over the right elbow for the past 2 days. The patient gave a history of fall at home on a flexed elbow and sustained a closed injury to the right elbow. Following fall, she was unable to move her arm and complained of severe pain. She was taken to an indigenous bone setter where primary treatment in the form of local splints was applied. Having no relief in pain over the next few days, the patient presented to us seeking relief. She was a known diabetic on medications. Initial clinical examinations revealed diffuse swelling over the right elbow with bruising over the posterior and lateral aspects. Tenderness was elicited around all the elbow bony prominences with a restricted range of motion at the affected elbow joint. There was no neurovascular deficit in the affected extremity. Radiographic assessment of the elbow (anteroposterior [AP]/lateral) revealed fractures involving the olecranon, a “double–arc” shadow depicting capitellum fracture on the lateral view, and lateral condyle fracture on AP view. The patient was advised to undergo higher imaging (computed tomography), but it was not affordable for any further investigations (Fig. 1).
The patient was counseled about the need for surgical intervention for the optimal outcome of the affected joint. Considering the gross swelling, the patient was put on an above-elbow slab, anti-inflammatory drugs for 5 days, and was asked to come back for surgical intervention. The patient was positioned in a left lateral decubitus position. A single standard posterior incision was advocated. The olecranon fracture window was utilized to approach the distal humerus. Appropriate soft tissue dissection and releases were done to approach the second fracture window of the lateral condyle-extensor mass. Indirect reduction of the capitellum was done using bone hooks and fixed with temporary K-wires. Fluoroscopy confirmed anatomical reduction of capitellum fragment, which was later fixed with headless compression screws in posterior to anterior direction. Lateral condyle fixation followed next, which was achieved by means of a K-wire and 4 mm canulated cancellous screw. Finally, the olecranon fracture was fixed by a standard tension band wiring (Fig. 2). The wound was closed in layers, and the elbow was immobilized for the next 10 days in a slab. The patient was followed up at regular intervals of 3 weeks for the initial 3 months and later at interval of 3 months over a 1-year period. Gradual elbow movements were started at 3 weeks, and at the final follow-up (1 year), the patient had a range of 10°–130° elbow flexion. Radiographs showed good bony union with no evidence of arthritic changes (Fig. 3).


Coronal shear injuries are a rare subgroup of fractures affecting the elbow. Axial load on a flexed elbow is considered the predisposing cause of such injuries [1,2]. However, a peculiar fracture pattern where olecranon, capitellum, and lateral condyle are involved raises inquisitiveness on the injury mechanism. Understanding the forces leading to a fracture is an important aspect of orthopedic trauma fixation, as it aids in easier reduction and better fixation outcomes. The mechanism of coronal shear fractures was elaborated by Watts et al. where a low-energy fall and direct compression of the distal humerus by a radial head in a flexed elbow was considered to be the cause of such fractures [7]. A case series of fractures involving the capitellum and olecranon was discussed by Sun et al. where he further illustrated how an axial load on a flexed elbow gets transmitted from the point of impact and transmits fracturing the olecranon and extends into the capitellum [3]. The mechanism of the injury in our case was quite similar, where a fall on a flexed elbow transmits the force from the primary point of contact (olecranon) and then transmits through the osteoporotic bones to fracture the capitellum. However, the final component of the injury (varus/valgus strain) is the force component, which leads to the third and final fracture component. We suggest that following the primary axial loading impact, the secondary varus/valgus thrust on a flexed elbow ultimately leads to the distal humerus loading against the proximal ulna/radial head, respectively. The suggested mechanism of injury is well illustrated as shown in Fig. 4.

Optimal management of these fractures is tricky. These fracture patterns are usually encountered in osteoporotic bones [2]. Open reduction and internal fixation remain the mainstay of treatment, which has shown good results over the years [5,6]. However, deciding on the ideal approaches remains debatable. Lateral extensile, combined posterior and lateral, and additional medial window all have been described in literature, where surgeons have usually resorted to a dual approach to deal with such complicated fractures [8-10]. In our case, we have described a “dual-fracture” window technique to deal with all the fracture components. A single standard posterior skin incision exposes the olecranon fracture site, which was utilized as the first window to access the posterior distal humerus. The lateral condyle fracture was utilized as the second window to access the capitellum fragment. Utilizing the fracture windows helped to adequately access and fix the fracture fragments (Fig. 5). A similar fracture window was utilized by Sun et al. [3] in their report of two cases, where the olecranon fracture window was utilized to fix the capitellum fracture in posterior-anterior fashion.
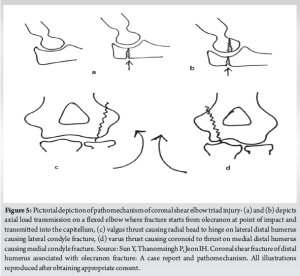
We propose a mechanism of such an unusual coronal shear fracture triad where the force transmission across the olecranon into the capitellum shear fracture is due to the axial load on a flexed elbow. The final varus/valgus thrust on the flexed elbow causes the final energy dissipation, leading to the medial/lateral condyle fracture, respectively. A single incision posterior approach can be enough to reduce and fix them, if fracture windows are utilized appropriately. This will significantly reduce the operating time and reduce the need for a second approach to fix such fractures.
Elbow coronal shear injuries are usually seen during fall on a flexed elbow. This entails a variety of fracture patterns. A fracture triad involving – capitellum, olecranon, and lateral condyle is very rare. Fracture windows can be utilized judiciously to approach all the fragments and anatomically fix them in a single approach. This fracture window technique can be utilized by surgeons in fixing a variety of elbow coronal shear fractures.
References
- 1.McKee MD, Jupiter JB, Bamberger HB. Coronal shear fractures of the distal end of the humerus. J Bone Joint Surg Am 1996;78:49-54. [Google Scholar | PubMed]
- 2.Yari SS, Bowers NL, Craig MA, Reichel LM. Management of distal humeral coronal shear fractures. World J Clin Cases 2015;3:405-17. [Google Scholar | PubMed]
- 3.Sun Y, Thanomsingh P, Jeon IH. Coronal shear fracture of distal humerus associated with olecranon fracture: A case report and pathomechanism. J Orthop Surg (Hong Kong) 2019;27:2309499019849707. [Google Scholar | PubMed]
- 4.Singh AP, Singh AP. Coronal shear fractures of distal humerus: Diagnostic and treatment protocols. World J Orthop 2015;6:867-76. [Google Scholar | PubMed]
- 5.Dressler HB, De Paula RN. Bryan and morrey type IV intra-articular fracture of the distal extremity of the humerus treated surgically with anterior access: Case report. Rev Bras Ortop 2015;50:352-5. [Google Scholar | PubMed]
- 6.Stamatis E, Paxinos O. The treatment and functional outcome of type IV coronal shear fractures of the distal humerus: A retrospective review of five cases. J Orthop Trauma 2003;17:279-84. [Google Scholar | PubMed]
- 7.Watts AC, Morris A, Robinson CM. Fractures of the distal humeral articular surface. J Bone Joint Surg Br 2007;89:510-5. [Google Scholar | PubMed]
- 8.Imatani J, Morito Y, Hashizume H, Inoue H. Internal fixation for coronal shear fracture of the distal end of the humerus by the anterolateral approach. J Shoulder Elbow Surg 2001;10:554-6. [Google Scholar | PubMed]
- 9.Abbassi N, Abdeljaouad N, Daoudi A, Yacoubi H. Isolated fracture of the humeral trochlea: A case report and review of the literature. J Med Case Rep 2015;9:121. [Google Scholar | PubMed]
- 10.Tarallo L, Novi M, Porcellini G, Giorgini A, Micheloni G, Catani F. Surgical tips and tricks for coronal shear fractures of the elbow. Arch Orthop Trauma Surg 2021;141:261-70. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 December 1, 2025 Engagement of the Radial Head in Posterior Capitellum Fracture: Defining the Critical Point
December 1, 2025 Engagement of the Radial Head in Posterior Capitellum Fracture: Defining the Critical Point November 1, 2025 Surgical Treatment of Neglected Elbow Dislocation with the Box-loop Technique: A Case Report
November 1, 2025 Surgical Treatment of Neglected Elbow Dislocation with the Box-loop Technique: A Case Report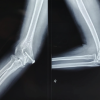 October 1, 2025 A Rare Repair: Trochlear Fracture Fixed With Headless Screws and Medial Epicondyle Osteotomy – A Case Report
October 1, 2025 A Rare Repair: Trochlear Fracture Fixed With Headless Screws and Medial Epicondyle Osteotomy – A Case Report August 1, 2025 Elbow Interpositional Arthroplasty using an Achilles Tendon Allograft: A Case Report
August 1, 2025 Elbow Interpositional Arthroplasty using an Achilles Tendon Allograft: A Case Report