
Using external fixators may be a viable alternative for intra-articular distal fractures.
Dr. Subramanya Gandhi, Department of Orthopaedics, A.C.S Medical College And Hospital, Chennai, Tamil Nadu, India. Mail Id: dr.subramanyagandhi@yahoo.com
Abstract
Introduction: Comminuted intra-articular distal radius fractures are complex injuries often resulting from high-energy trauma, requiring precise reduction and stable fixation. Spanning external fixation, with optional K-wire augmentation, has emerged as a minimally invasive technique offering reliable stabilization through ligamentotaxis while reducing operative time, blood loss, and infection risks.
Case Series: This case series evaluated patients with AO Type C3 distal radius fractures treated using spanning external fixators with optional K-wire supplementation. Functional outcomes were assessed using the disabilities of arm, shoulder, and hand score, and radiological outcomes were evaluated using the Sarmiento radiological score over a 1-year follow-up period. Almost all patients achieved excellent results on both scoring systems, with minimal complications and no significant functional limitations reported.
Conclusion: Spanning external fixation, with or without K-wire support, is an effective alternative to open reduction methods for complex intra-articular distal radius fractures. It offers the advantages of simplicity, reduced operative duration, less blood loss, and a lower risk of infection, making it a reliable option for managing these challenging injuries.
Keywords: Distal radius fracture, spanning external fixator, intra-articular fracture, K-wire augmentation, disabilities of arm, shoulder, and hand score, Sarmiento radiological score, AO type C3, ligamentotaxis.
Comminuted intra-articular distal radius fractures[Fig.1] present a significant challenge due to their complexity and the need for precise anatomical restoration [1-5]. These fractures often result from high-energy trauma and require stable fixation to achieve optimal functional outcomes [6,7]. While open reduction and internal fixation (ORIF) is widely considered the standard of care, spanning external fixation—with optional K-wire augmentation[Fig.2]—has emerged as a minimally invasive and reliable technique [8-17]. It facilitates ligamentotaxis, reduces operative time, minimizes blood loss, and lowers infection risks [18]. This study evaluates the functional and radiological outcomes of such treatment.

This prospective observational study included 30 adult patients with AO Type C3 distal radius fractures treated with spanning external fixation and optional K-wire augmentation[Fig.2]
Sample size calculation
The sample size was calculated based on an expected improvement of 15 points in the disabilities of arm, shoulder, and hand (DASH) score with a standard deviation of 20, a power of 80%, and alpha error of 5%, yielding a minimum sample size of 27. We enrolled 30 patients to account for potential dropouts or loss to follow-up.
Inclusion criteria
- Adults aged 18–65 years
- Closed, comminuted intra-articular distal radius fractures (AO type C)
- Fractures treated within 7 days of injury
- Willingness to participate and comply with 1-year follow-up.
Exclusion criteria
- Open fractures
- Associated neurovascular injury
- Previous wrist pathology or fracture on the same limb
- Bilateral wrist fractures
- Patients unfit for surgery or general anesthesia.
Operative technique
Under regional or general anesthesia, closed reduction was attempted under C-arm guidance. A spanning external fixator was applied between the radius and the second metacarpal, ensuring appropriate distraction and alignment. Optional K-wire fixation was added based on the level of comminution and fracture stability. Typically, 1–2 K-wires were used to transfix the fracture fragments. Postoperatively, patients were advised to perform finger range-of-motion exercises while maintaining the external fixator for 6–8 weeks.
Functional outcome assessment
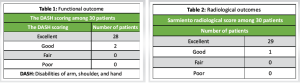
Functional outcomes were evaluated using the Disabilities of Arm, Shoulder, and Hand (DASH) score at regular intervals post-operatively. As shown in Table 1, 28 patients (93.3%) had excellent outcomes, and 2 patients (6.7%) had good outcomes, with no fair or poor results.
Radiological outcome assessment
Radiological results were assessed using the Sarmiento radiological score. As presented in Table 2, 29 patients had excellent results, and one had a good outcome.
Statistical analysis plan
Data were analyzed using the Statistical Package for the Social Sciences Version 25. Continuous variables like DASH scores were presented as mean ± standard deviation. Categorical outcomes (e.g., radiological grading) were expressed as percentages. Paired t-tests were used to compare DASH scores over time. A P < 0.05 was considered statistically significant.
Our findings align with previous studies by Ju et al. [17] and Chen et al. [18], showing good-to-excellent outcomes using external fixators with K-wire augmentation. This technique offers advantages over ORIF in cases of severe comminution or compromised soft tissue.
As in prior studies [19,20], we observed no major complications such as infection or CRPS. Compared to volar plating, external fixation is less technically demanding and more adaptable in high-volume trauma settings.
Interpretation of our results
In our study, the majority of patients achieved excellent functional and radiological outcomes using external fixation with optional K-wire augmentation. DASH scores improved significantly over the follow-up period, indicating substantial restoration of upper-limb function. Radiologically, most patients maintained near-anatomical alignment per the Sarmiento score. These results suggest that external fixation, with careful patient selection and proper technique, is a reliable alternative for managing complex distal radius fractures.
Relation to research objective
The primary objective of this study was to assess the effectiveness of external fixation (with optional K-wire pinning) in managing comminuted intra-articular distal radius fractures. Our findings support the hypothesis that external fixation provides good to excellent outcomes[Fig. 3-7] in cases where ORIF may pose technical difficulties, longer operative time, and higher soft tissue morbidity.

Comparison with other studies
Our findings are consistent with several national and international studies that support the use of external fixation for unstable distal radius fractures. Kapoor et al. and Rozental et al. reported comparable DASH score improvements and radiological maintenance using external fixators [15,16]. In contrast, some studies favor ORIF for early mobilization and slightly better range of motion outcomes. However, these differences may stem from variability in fracture patterns, surgical expertise, or post-operative rehabilitation protocols. In severely comminuted cases, the challenges of anatomic reduction and risks of surgical morbidity make external fixation a more pragmatic option.
Order of importance in findings
- Excellent functional outcomes (DASH score): Restoration of upper-limb function was consistently observed[Fig.3-6]
- Radiological maintenance (Sarmiento score): Near-anatomical alignment was preserved in most cases[Fig. 7]
- Minimal soft tissue complications: Compared to open methods, no significant soft tissue compromise or infections were noted
- Reduced operative time and blood loss: Especially important in elderly or high-risk patients
- Ease of technique: Suitable for surgeons in resource-limited or high-volume trauma settings.
Limitations of our study
- Small sample size: With only 30 patients, results may not be generalizable to all populations
- Lack of a control group: We did not directly compare external fixation with ORIF in the same setting
- Short-term follow-up: A 1-year follow-up may not capture long-term complications like late arthritis or loss of reduction
- Single-center study: Surgical outcomes may vary with different teams and settings.
Suggestions for future research
Larger, multicentric randomized controlled trials comparing external fixation and ORIF in various fracture subtypes could provide more definitive guidance. Long-term studies with follow-ups beyond 2–3 years would help assess post-traumatic arthritic changes, range of motion deficits, and patient satisfaction. Comparative cost-effectiveness analyses would also benefit healthcare systems in determining the best surgical option.
A total of 30 patients with comminuted intra-articular distal radius fractures were included in the study. The mean age of the patients was 42.6 years (range: 25–65 years). All patients were treated with external fixation, with optional K-wire augmentation depending on the fracture pattern.
The mean follow-up duration was 12 months, during which both functional and radiological outcomes were assessed.
Functional outcome (DASH score)
- Excellent results were observed in 28 patients (93.3%), with a significant reduction in DASH scores over the follow-up period
- Good results were recorded in 2 patients (6.7%), primarily due to stiffness and delayed rehabilitation
- No patients were graded as fair or poor
- The mean DASH score at the final follow-up was 14.2 (lower scores indicate better function).
Radiological outcome (Sarmiento score)
- According to the Sarmiento radiological scoring system:
- Excellent outcomes were observed in 29 patients (96.7%)
- Good outcome in 1 patient (3.3%).
- The one patient with a good score had a minor loss of radial length and palmar tilt but retained functional use.
No cases of pin tract infection, complex regional pain syndrome, or loss of reduction were noted during the follow-up period.
We concluded that spinning external fixation is a good option for the treatment of AO-type C3 distal radius fractures. The good outcomes of this study suggest that use of the spanning external fixators could be an alternative treatment method for intra articular distal fractures, as it is easier, needs less operation time, decreases amount of blood loss, and decreases risk of infection in comparison with spanning bridging plate or locked distal radius plates.
Spanning external fixation is a valuable treatment option for AO-type C3 distal radius fractures. This technique offers advantages such as simplicity, reduced operative time, minimized blood loss, and a lower risk of infection compared to spanning bridging plates or locked distal radius plates. It serves as an effective alternative for managing intra-articular distal fractures.
References
- 1.Peltier LF. Eponymic fractures: John Rhea Barton and Barton’s fractures. Surgery 1953;34:960-70. [Google Scholar | PubMed]
- 2.Slutsky DJ, Osterman AL. Fractures and Injuries of the Distal Radius and Carpus: The Cutting Edge. Philadelphia, PA: Saunders/Elsevier; 2009. p. 563. [Google Scholar | PubMed]
- 3.Tang Z, Yang H, Chen K, Wang G, Zhu X, Qian Z. Therapeutic effects of volar anatomical plates versus locking plates for volar Barton’s fractures. Orthopedics 2012;35:1198-203. [Google Scholar | PubMed]
- 4.Aggarwal AK, Nagi ON. Open reduction and internal fixation of volar Barton’s fractures: A prospective study. J Orthop Surg (Hong Kong) 2004;12:230-4. [Google Scholar | PubMed]
- 5.Dai MH, Wu CC, Liu HT, Wang IC, Yu CM, Wang KC, et al. Treatment of volar Barton’s fractures: Comparison between two common surgical techniques. Chang Gung Med J 2006;29:388-94. [Google Scholar | PubMed]
- 6.Vasenius J. Operative treatment of distal radius fractures. Scand J Surg 2008;97:290-6. [Google Scholar | PubMed]
- 7.Bartl C, Stengel D, Bruckner T, Rossion I, Luntz S, Seiler C, et al. Open reduction and internal fixation versus casting for highly comminuted and intra-articular fractures of the distal radius (ORCHID): Protocol for a randomized clinical multi-center trial. Trials 2011;12:84. [Google Scholar | PubMed]
- 8.Rikli DA, Kupfer K, Bodoky A. Long-term results of the external fixation of distal radius fractures. J Trauma 1998;44:970-6. [Google Scholar | PubMed]
- 9.Wolfe SW, Austin G, Lorenze M, Stigart CR, Panjabi MM. A biomechanical comparison of different wrist external fixators with and without K-wire augmentation. J Hand Surg Am 1999;24:516-24. [Google Scholar | PubMed]
- 10.Fernandez DL, Wolfe SW. Distal radius fractures. In: Green DP, Hotchkiss RN, Pederson WC, Wolfe SW, editors. Green’s Operative Hand Surgery. 5th ed. Philadelphia, PA: Churchill Livingstone; 2005. p. 645-710. [Google Scholar | PubMed]
- 11.Beasley RW. Beasley’s Surgery of the Hand. New York: Thieme Medical Publishers; 2003. [Google Scholar | PubMed]
- 12.Jupiter JB. Intra-articular distal radius fractures. In: Berger RA, Weiss AP, editors. Hand Surgery. Vol. 2. Philadelphia, PA: Lippincott; 2004. p. 277-95. [Google Scholar | PubMed]
- 13.Mackenney PJ, McQueen MM, Elton R. Prediction of instability in distal radial fractures. J Bone Joint Surg Am 2006;88:1944-51. [Google Scholar | PubMed]
- 14.Missakian ML, Cooney WP, Amadio PC, Glidewell HL. Open reduction and internal fixation for distal radius fractures. J Hand Surg Am 1992;17:745-55. [Google Scholar | PubMed]
- 15.Wolfe SW. Patterns and treatment of distal radius fractures. In: Proceedings of the AAOS/ASSH Update on the Painful and Injured Wrist. Helsinki: Rosemont, IL; 2009. p. 66. [Google Scholar | PubMed]
- 16.Alam W, Shah FA, Qureshi KM, Rehman SU, Hussain S, Imran M. Intra-articular fractures of distal radius; outcome of treated with bridging (static) external fixator. Prof Med J 2014;21:649-53. [Google Scholar | PubMed]
- 17.Mancuso CA, Jin Z, Swigler CW, Merrell G, Wolfe SW. Distal radius fracture outcomes in older adults: A prospective multicenter cohort study. J Hand Surg Am 2020;45:856.e1-14. [Google Scholar | PubMed]
- 18.Ju DG, Lee JY, Shin SJ. Clinical and radiological outcomes following external fixation with additional K-wires for unstable distal radius fractures in elderly patients. Clin Orthop Surg 2020;12:366-72. [Google Scholar | PubMed]
- 19.Chen Y, Liu Z, Pan Y, Zhu Y, Zhang X. External fixation versus volar locking plate fixation for distal radius fractures: A systematic review and meta-analysis of randomized controlled trials. Orthop Surg 2021;13:942-50. [Google Scholar | PubMed]
- 20.Walenkamp MM, Mulders MA, Goslings JC, Schep NW. External fixation versus volar locking plate for distal radius fractures: A meta-analysis. Injury 2016;47:278-85 [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2025 Functional Outcome of Distal Radius Fractures Managed by Minimally Invasive Plate Osteosynthesis: A Prospective Study of 20 Patients
May 1, 2025 Functional Outcome of Distal Radius Fractures Managed by Minimally Invasive Plate Osteosynthesis: A Prospective Study of 20 Patients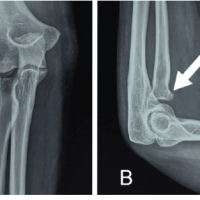 March 1, 2025 Functional Outcome of Radial Head Fracture Treated with Open Reduction Internal Fixation using Plating Versus Herbert Screw Fixation: A Case Series
March 1, 2025 Functional Outcome of Radial Head Fracture Treated with Open Reduction Internal Fixation using Plating Versus Herbert Screw Fixation: A Case Series October 1, 2024 A Study of Functional Outcome and Assessment of Role of Proximal Humerus Internal Locking System (Philos) Plating in Elderly Population with Proximal Humerus Fracture: A Case Series
October 1, 2024 A Study of Functional Outcome and Assessment of Role of Proximal Humerus Internal Locking System (Philos) Plating in Elderly Population with Proximal Humerus Fracture: A Case Series August 1, 2026 Isolated Calcific Deposition in the Subacromial Bursa: A Rare Case Report and Arthroscopic Management
August 1, 2026 Isolated Calcific Deposition in the Subacromial Bursa: A Rare Case Report and Arthroscopic Management