
Cost-effective semitendinosus graft augmentation for quadriceps tendon tear.
Dr. H Varrdhaman Dhariwal, Department of Orthopaedics, Stanley Medical College, Chennai, Tamil Nadu, India. E-mail: varrdh@gmail.com
Abstract
Introduction: Quadriceps tendon injury is a very uncommon injury among athletes. The incidence is 13% of all tendon injuries. Quadriceps tendon injury is usually male predominant.
Case Series: The study was conducted in our medical college in the period of 2022–2025. Ten patients with quadriceps tendon ruptures were included in the study. Through anterior midline approach, the tear was identified. Transverse patellar tunnel created after harvesting semitendinosus graft. Graft passed through the tunnel and both limbs sutured to the tendon after repairing the rent. All the patients were reviewed postoperatively at 1, 3, 6, and 12 weeks. Out of the ten patients, all the patients had successful outcome at the end of 6 weeks. Every patient was followed upto 2 years to look for any complication. Two patients had superficial infection which was treated with antibiotics.
Discussion: Quadriceps tendon injury is a very uncommon injury among athletes. The most commonly used method of repair is ipsilateral hamstring grafting. Other methods like stabilization with suture anchor, the Codivilla technique, and platelet-rich plasma administration are also being used. Chronic quadriceps tendon injuries are found to be more challenging to repair than acute tears. Surgical treatment has been the gold standard and has remained unchanged for several years. Our technique helps the patient in restoring the extensor mechanism of the knee and early return to his functional activities and thus protecting his knee from developing arthritis and instability.
Conclusion: This is a case series which includes ten cases with adequate follow-up. The main objective of this procedure was to restore the patient’s ability to extend and flex his knees without lag and return to day-to-day life by a single sitting definitive procedure without any implant in situ.
Keywords: Quadriceps tendon tear, semitendinosus graft, patellar tunnel, cost effective.
Acute quadriceps tendon injuries are predominantly due to eccentric loading of heavy body weight with the knee in flexion and volar flexed foot. The tear or ruptures of the muscle usually occurs in a transverse pattern at the tendinous insertion site in geriatric population and at the middle of the tendon substance or the muscle bulk in young individuals. At around 1–2 cm, above the upper pole of patella is considered to be the most common place for tears, as it is considered to be the reduced blood supply zone. Partial or incomplete tears are usually treated nonoperatively or conservatively, depending on the magnitude of the tear and the patient’s requirement or activity level, patient can be immobilized using either a above knee cast or a long knee brace for 6 weeks, followed by slow and gradual strengthening and rehabilitation exercises. Immobilizer is gradually weaned off when good quadriceps strength is achieved with a good straight leg raise (SLR) without extensor lag. For larger ruptures, surgical intervention has to be done without delay. If the distal attachment is, the muscle starts retracting within a week time. As time advances, the repair of the torn ends becomes difficult due to increased tension along the repaired ends. A defect of 2.5–5.0 cm or more can happen between the tendon ends, if neglected for more than 3 months. For both acute and chronic tears of the quadriceps muscle, the above-mentioned technique can be used effectively and successful outcome can be obtained.
The study was conducted in Government Stanley Medical college in the period of 2022–2025. Ten patients with quadriceps tendon ruptures were included in the study. All the patients underwent pre-operative evaluation. Proper pre-operative evaluation done using X-ray knee anteroposterior and lateral (standing) and magnetic resonance imaging (MRI). Computed tomography is not required for all cases. Post-operative evaluation scoring is done using International Knee Documentation Committee (IKDC) and Tegner Lysholm score.
Operative Technique
The described operative technique is done in supine position with knee in extension. Make an (Fig. 1 & 2) adequate midline incision expose the torn ends of the tendon[Fig. 5]. The hematoma is well irrigated with adequate wash and both the ends of the torn tendon identified (Fig. 3) and freshened. A transverse patellar tunnel is created using 4.5 mm cannulated drill bit after verifying the correct position in C-arm in upper one third and lower two third. Semitendinosus graft harvested using the same incision (Fig. 4). Graft passed through the tunnel using suture shuttling/loops or wire passer. Both limbs of the graft are taken on either side of the patella and then sutured to the muscle bulk of the quadriceps, as shown in Fig. 1 after primary repair of the tear. If adequate tendon is left proximally, make a side to side repair using 5-ethibond sutures through the tendon and 0-vicryl retinacular repair. After good repair of the tendon, evaluate patellar tracking. Move the knee and check the movements to evaluate position of the patella. Retinacular repair should be done with interrupted sutures using vicryl and preceded with layered closure. Apply an above knee slab or a cast (after suture removal) or locked knee brace in extension. Strict non-weight-bearing walking till 6 weeks. Closed chain knee bending exercises are encouraged till 30° after good workup of quads and hamstring exercises for 2 weeks extensively. All the patients were reviewed postoperatively at 1, 3, 6, and 12 weeks and also at the end of one and 2 years, respectively. Out of the ten patients, all the patients had successful outcome at the end of 12 weeks. Two patients had superficial infection which was treated with oral antibiotics. Serial follow-up was done until 2 years to assess the durability of the repair, potential graft loosening, or to the assess whether the patient has developed any extensor lag.


Quadriceps tendon ruptures are uncommon injuries among athletes and accounts for 3% of all tendon injuries in road traffic accident. Chronic tendon ruptures are difficult to repair. Surgical management has remained gold standard for these ruptures. We present an implant free reconstruction of the quadriceps tendon using autologous semitendinosus graft. Using the above described operative technique, the extensor mechanism of the patient is well reconstructed, letting the patient to return to his normal day-to-day activities. The use of autologous hamstring graft has its own biological advantages which have already been described in the past and is a common graft in used in ligamentous reconstruction in knee surgeries. Its long-term viability, stable biomechanical properties provides evidence for its use in using it for this procedure. According to literature, autologous hamstring graft and gracilis has also been used for its reconstruction with pulvertaft weave or with or without suture anchor [1-3], but our technique allows transosseous repair using autologous graft. Another technique, Codivilla technique lengthens the tendon in chronic retracted tendon rupture by V-Y plasty (tendon lengthening) and suture anchors [4-6]. V-Y plasty in chronic retracted tendon in total knee arthroplasty patients is also being done but tendon viability and strength need to take care of [7,8]. The use of polyethylene terephthalate tape has been used recently for reconstruction of quadriceps tendon [9,10] with good biological outcome, but autologous grafting stays superior to any implant used otherwise. Prolene mesh has also been used to repair chronic retracted tears with layered closure [5]; however, its bio integrity is questionable. Autologous conditioned plasma augmentation [5] has also been used for quadriceps tendon tear with gradual pain relief and improvement of movements, but it is not considered to be a definitive treatment. In spite of the advantages of autologous hamstring graft, hamstring grafts has its own challenges especially in elderly individuals. This can be assessed using pre-operative clinical assessment and MRI. Hence, pre-operative evaluation of patients is of utmost importance. A drill bit of not more than 4.5 mm should be used as there can be graft loosening with age or intraoperative patellar fractures. Although the outcome depends on the proper post-operative follow-up and rehabilitation and patient doctor relationship and cooperation, the major advantage of this technique is that, it is a no implant whereas other techniques mentioned above uses either a suture anchor or a mesh for the repair and achieves full extensor function of the knee and patient returning to his day-to-day activities and future preferences to go for a MRI or any other radiological screening, an implant in situ might be of hindrance and this technique avoids this complication. Table 1 shows good results at 12 weeks follow-up. After 12 weeks of good physio and rehabilitation, patient is able to do good flexion (Fig. 6) and SLR and that too without extensor lag (Fig. 7). The outcome of the procedure was assessed until 2 years using Tegner Lysholm score and IKDC (S) [TABLE 1] scoring system and we obtained excellent results. Potential complications following the procedure include graft loosening, patellar fractures, maltracking, extensor lag, and infection. We did not have any of these complications except superficial infections in two patients.


We were successful in achieving a stable knee with regaining of the extensor mechanism by augmenting the repair of the quadriceps tendon using autologous hamstring graft by biological augmentation. Our technique is effective for both acute and chronic quadriceps tendon tear as a definitive treatment. In both acute and chronic ruptures, we had excellent functional outcomes and patient satisfaction and were assessed using IKDC and Tegner and Lysholm scores both pre-operative and post-operative.
Locally available graft can be used to give a robust repair of torn quadriceps tendon. It is an implant free technique with excellent regainment of knee function and there is no fracture of the patella or graft loosening in long-term follow-up. All the patients had excellent results in a single sitting definitive procedure.
References
- 1. Ilan DI, Tejwani N, Keschner M, Leibman M. Quadriceps tendon rupture. J Am Acad Orthop Surg 2003;11:192-200. [Google Scholar] [PubMed]
- 2. Elattar O, McBeth Z, Curry EJ, Parisien RL, Galvin JW, Li X. Management of chronic quadriceps tendon rupture: A critical analysis review. JBJS Rev 2021;9:???.page no 9. [Google Scholar] [PubMed]
- 3. Rehman H, Kovacs P. Quadriceps tendon repair using hamstring, prolene mesh and autologous conditioned plasma augmentation. A novel technique for repair of chronic quadriceps tendon rupture. Knee 2015;22:664-8. [Google Scholar] [PubMed]
- 4. Shah MK. Simultaneous bilateral rupture of quadriceps tendons: Analysis of risk factors and associations. South Med J 2002;95:860-6. [Google Scholar] [PubMed]
- 5. Pengas IP, Assiotis A, Khan W, Spalding T. Adult native knee extensor mechanism ruptures. Injury 2016;47:2065-70. [Google Scholar] [PubMed]
- 6. Reito A, Paloneva J, Mattila VM, Launonen AP. The increasing incidence of surgically treated quadriceps tendon ruptures. Knee Surg Sports Traumatol Arthrosc 2019;27:3644-9. [Google Scholar] [PubMed]
- 7. Clayton RA, Court-Brown CM. The epidemiology of musculoskeletal tendinous and ligamentous injuries. Injury 2008;39:1338-44. [Google Scholar] [PubMed]
- 8. Rougraff BT, Reeck CC, Essenmacher J. Complete quadriceps tendon ruptures. Orthopedics 1996;19:509-14. [Google Scholar] [PubMed]
- 9. Scuderi C. Ruptures of the quadriceps tendon; study of twenty tendon ruptures. Am J Surg 1958;95:626-35. [Google Scholar] [PubMed]
- 10. Chhapan J, Sankineani SR, Chiranjeevi T, Reddy MV, Reddy D, Reddy AV. Early quadriceps tendon rupture after primary total knee arthroplasty. Knee 2018;25:192-4. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 October 29, 2014 Editorial – Social Media and Orthopaedic Surgeon: Concept of Orthopaedic Educational and Academic Network (OCEAN)
October 29, 2014 Editorial – Social Media and Orthopaedic Surgeon: Concept of Orthopaedic Educational and Academic Network (OCEAN) April 10, 2022 A 22-Month old with a Neglected Monteggia Injury: A Case Report and Review of the Literature
April 10, 2022 A 22-Month old with a Neglected Monteggia Injury: A Case Report and Review of the Literature May 10, 2024 Spontaneous First Metatarsal Rotational Correction by the Syndesmosis Procedure for Hallux Valgus Deformity: A Case Report
May 10, 2024 Spontaneous First Metatarsal Rotational Correction by the Syndesmosis Procedure for Hallux Valgus Deformity: A Case Report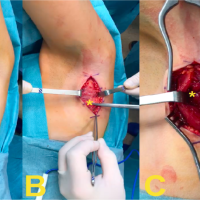 September 10, 2021 Surgical Management of a Latissimus Dorsi Costal Tear in an Elite Female Handball Player: A Case Report
September 10, 2021 Surgical Management of a Latissimus Dorsi Costal Tear in an Elite Female Handball Player: A Case Report