
Partial resection of the calcaneal tuberosity with bursectomy significantly improves functional outcomes in patients with Haglund’s syndrome unresponsive to conservative management.
Dr. Ashin Khan, Department of Orthopaedics, Sree balaji medical college and hospital, Chrompet , Chennai, Tamil Nadu 600044, India. E-mail: aashinkhan.31@gmail.com
Abstract
Introduction: The aims and objectives of the study are to evaluate the functional improvement and radiological outcomes following partial resection of the calcaneal tuberosity in patients with Haglund’s syndrome unresponsive to conservative management using the American Orthopaedic Foot and Ankle Society (AOFAS) scoring system as illustrated in Figure.
Materials and Methods: From January 2023 to July 2025, 12 adult patients treated at Sree Balaji Medical College Hospital with symptomatic Haglund’s syndrome underwent partial calcaneal tuberosity resection and bursectomy. Patients had failed ≥3 months of conservative care. Functional assessments (AOFAS hindfoot score) and lateral radiographs (Fowler–Philip angle, calcaneal pitch, and total calcaneal angle) were recorded preoperatively, and at 6 weeks, 3 months, and final follow-up (minimum 6 months).
Results: Mean AOFAS scores improved from 55.6 preoperatively to 77.5 at 6 months, indicating statistically and clinically significant improvement. No major complications were observed during the follow-up period. Partial osteotomy of the calcaneal tuberosity offers a safe and effective option for patients with Haglund’s syndrome who fail to respond to conservative therapy. It significantly improves function and reduces pain, as evidenced by a consistent rise in AOFAS scores.
Conclusion: Partial osteotomy of the calcaneal tuberosity offers a safe and effective option for patients with Haglund’s syndrome who fail to respond to conservative therapy. It significantly improves function and reduces pain, as evidenced by consistent rise in AOFAS scores.
Keywords: Haglund’s syndrome, calcaneal tuberosity osteotomy, American Orthopaedic Foot and Ankle Society score, heel pain, foot surgery, retrocalcaneal bursitis, functional outcome.
Haglund’s syndrome is a painful condition involving a bony prominence on the posterosuperior aspect of the calcaneus, often leading to retrocalcaneal bursitis and Achilles tendinopathy [1]. This disorder, commonly seen in active individuals, particularly females, can cause significant morbidity. The pathophysiology involves irritation caused by mechanical impingement between the Achilles tendon and the prominent calcaneal tuberosity [2].
Conservative treatment options include non-steroidal anti-inflammatory drugs, heel lifts, footwear modifications, and physiotherapy [3]. Surgical intervention becomes necessary when conservative methods fail [4]. Partial osteotomy of the calcaneal tuberosity, by reducing the bony prominence, aims to relieve pressure on the Achilles insertion and retrocalcaneal bursa, thereby alleviating symptoms [5,6]. Several techniques have been described, but outcomes vary depending on the surgical approach and patient compliance.
This study was designed to evaluate the short-term functional outcome of partial calcaneal osteotomy using the American Orthopaedic Foot and Ankle Society (AOFAS) hindfoot score as a standardized metric in a cohort of patients treated at a tertiary care teaching hospital in South India.
Patient Selection and Grouping
- Study center: Sree Balaji Medical College and Hospital, Chennai
- Study design: Prospective case series
- Sample Size: 10 patients.
Inclusion criteria
- Adults (>18 years) with symptoms lasting for over 3 months
- Failure of conservative management for over 3 months
- No systemic inflammatory diseases.
Exclusion criteria
- Prior heel surgery
- Congenital foot deformities
- Recent steroid injection or trauma to the heel.
Surgical protocol
All surgeries were performed under spinal anesthesia with the patient in either supine or floppy lateral position, using either a medial or lateral approach. Bursal tissue and prominent bony exostosis were excised using osteotomes[7]. Postoperatively, a below-knee slab with 20° plantarflexion was applied. Protected weight-bearing was initiated at 3 weeks and full weight-bearing at 6 weeks. Follow-up was at 6 weeks, 3 months, and 6 months [8].
Functional assessment
- AOFAS hindfoot score evaluated at each visit.
- Clinical signs and radiographs were recorded to confirm healing and absence of recurrence.
A case series of 10 patients, with 7 female and 3 male patients, with a mean age of 42 years (range 36–50). All patients reported chronic posterior heel pain unresponsive to over 3 months of conservative therapy [3] (Table 1). Radiological confirmation was obtained in each case using Fowler’s angle and presence of parallel pitch lines as shown in Fig. 1 & 2 [1,9].
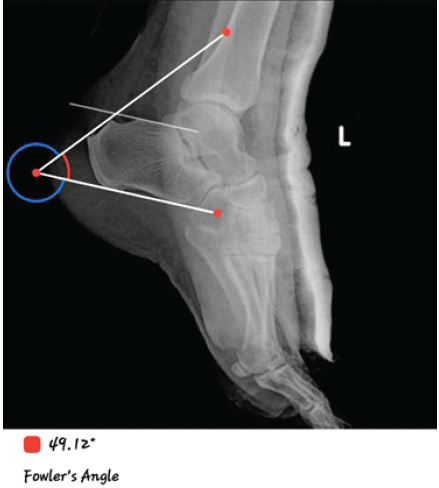
Figure 1: Post-operative lateral X-ray at 6 months showing restored heel contour and improved angles. Post-op X-ray. Fowler’s angle: 49. American Orthopaedic Foot and Ankle Society at 6 months: 73.
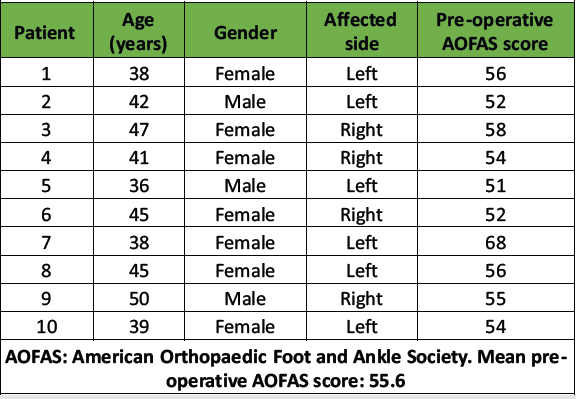
Table 1: Patient demographics and pre-operative scores
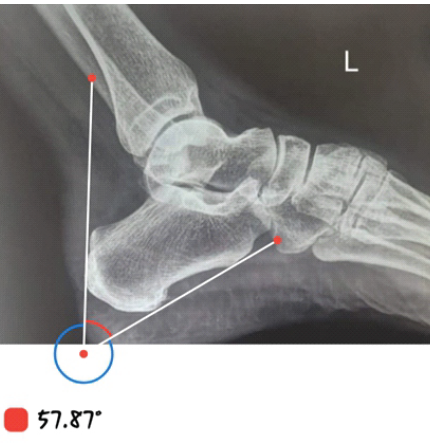
Figure 2: Pre-operative lateral X-ray showing bony prominence (Fowler’s angle: 58°). Pre-Op X-ray. Fowler’s angle: 58.
At 6 weeks postoperatively, all patients showed notable improvement. Mild-to-moderate residual discomfort was noted in two patients, especially with prolonged walking. At 3 months, functional gains were consistent, and at 6 months, all patients had significant pain relief and were able to resume normal daily activities (Table 2) as seen in Fig. 1 and 3 [10].
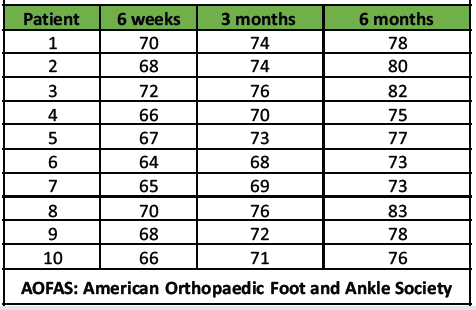
Table 2: Post-operative AOFAS scores over time
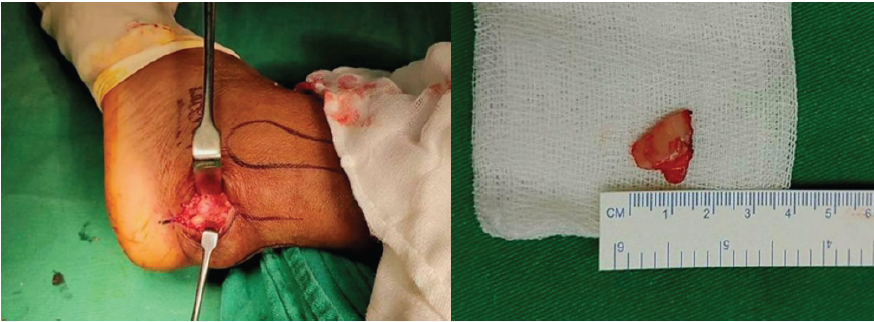
Figure 3: Intra-operative image showing partial resection of calcaneal tuberosity.
Post-operative imaging demonstrated a mean decrease of 8° in the Fowler–Philip angle, reflecting effective resection of the posterosuperior calcaneal prominence and mechanical decompression of the Achilles insertion.
Graphical analysis
The mean AOFAS scores showed consistent improvement:
- Pre-op: 55.6
- 6 weeks: 67.6
- 3 months: 72.3
- 6 months: 77.5
Graph 1 statistical analysis using paired t-tests indicated significant differences between pre-operative and all post-operative time points (P < 0.05). No wound infections, re-operations, or complications such as Achilles tendon avulsion or recurrence were reported during follow-up [11].
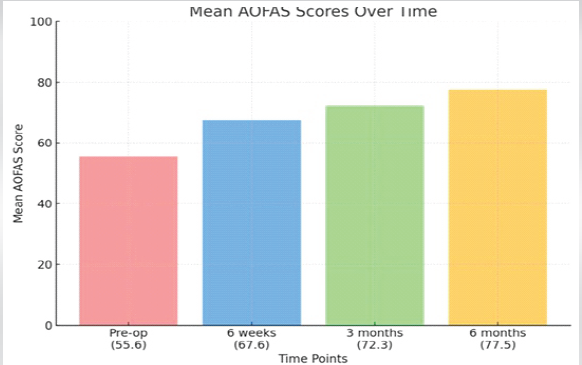
Graph 1: Mean American Orthopaedic Foot and Ankle Society over time.
Clinical illustration
A 38-year-old woman came in with primary complaints of pain in the posterior heel of her left foot, which has persisted for the past 2 years without any recent injury. The patient has tried physiotherapy and heel lifts to address the issue but has not experienced any relief, and she has been using painkillers for the discomfort. Her pre-operative AOFAS score was 68.
Haglund’s syndrome presents a treatment challenge due to its complex pathophysiology and tendency for recurrence [1,2]. When conservative modalities fail, surgery becomes essential to reduce the posterior calcaneal prominence and decompress adjacent soft tissues [3,4].
Conservative management – including heel lifts, physiotherapy, and anti-inflammatory therapy – remains first-line, but prolonged symptoms or recurrence are common. Surgical partial resection directly removes the mechanical impingement, providing faster and more durable pain relief when conservative measures fail [5,6].
Our results demonstrate that partial osteotomy is a highly effective intervention for this patient group as it effectively removes the impinging bone, providing lasting relief. All patients in our series showed functional improvement, as quantified by the AOFAS hindfoot score, which rose from a mean of 55.6 preoperatively to 77.5 at 6 months. This gain is consistent with previous studies: Mir et al. reported similar improvements in AOFAS scores post-lateral approach osteotomy [13]. Brunner J et al. [8], Nunley Ja et al. [12] and Anderson JA et al. [9] also found significant post-operative gains using various surgical methods.
The lack of serious complications in our study may be attributed to meticulous patient selection, strict post-operative protocols, and preservation of the Achilles tendon during surgery [7,9]. In addition, minimal soft tissue dissection through selective medial or lateral approaches may have aided in faster recovery and fewer wound complications .
While imaging angles like Fowler’s and pitch lines assist in diagnosis [1,9], clinical assessment remains crucial. AOFAS scoring served as a reliable, standardized metric for quantifying recovery in function and pain [3,6].
Limitations include a small sample size and a lack of a control or comparative group. However, the consistent improvement in all cases supports the reproducibility of this technique in skilled hands. Future studies may consider incorporating patient-reported outcome measures or comparing outcomes of different osteotomy techniques [14,15,16].
This case series contributes to growing evidence that partial osteotomy is a safe and effective intervention for refractory Haglund’s syndrome and offers reliable functional relief when non-operative treatment fails.
Partial osteotomy of the calcaneal tuberosity offers a safe and effective option for patients with Haglund’s syndrome who fail to respond to conservative therapy. It significantly improves function and reduces pain, as evidenced by a consistent rise in AOFAS scores.
Partial resection of the calcaneal tuberosity with bursectomy offers significant relief for patients with Haglund’s syndrome resistant to non-surgical measures. It improves functional outcomes with low complication rates when performed with meticulous technique.
References
- 1. Fowler AW. A review of the etiology and treatment of Haglund’s deformity. Br J Surg. 1945;32(128):334–344. [Google Scholar] [PubMed]
- 2. Pavlov H, Heneghan MA, Hersh A, Goldman AB. The Haglund syndrome: initial and differential diagnosis. Radiology. 1982;144(1):83–88. [Google Scholar] [PubMed]
- 3. Padanilam TG. The painful heel: a review of conservative and surgical management. Foot Ankle Int. 1985;6(4):180–186. [Google Scholar] [PubMed]
- 4. Sella EJ, Caminear DS, McLarney EA. Haglund’s syndrome. J Foot Ankle Surg. 1998;37(2):110–114. [Google Scholar] [PubMed]
- 5. Watson AD, Anderson RB, Davis WH. Comparison of surgical techniques for treatment of insertional Achilles tendinopathy. Foot Ankle Int. 2000;21(9):736–739. [Google Scholar] [PubMed]
- 6. McGarvey WC, Palumbo RC, Baxter DE. Insertional Achilles tendinosis: surgical management and outcomes. Am J Sports Med. 2002;30(3):360–365. [Google Scholar] [PubMed]
- 7. Saxena A, Fullem B. Surgery for insertional Achilles tendinopathy. J Foot Ankle Surg. 2004;43(5):347–352. [Google Scholar] [PubMed]
- 8. Brunner J, Anderson JA, O’Malley MJ. Surgical treatment of Haglund’s deformity: a retrospective review. Foot Ankle Int. 2005;26(10):792–797. [Google Scholar] [PubMed]
- 9. Anderson JA, Suero EM, O’Malley MJ. Operative management of Haglund’s deformity: indications and results. Foot Ankle Int. 2008;29(8):780–784. [Google Scholar] [PubMed]
- 10. Pinney SJ, McGarvey WC. Management of chronic insertional Achilles tendinopathy. J Am Acad Orthop Surg. 2010;18(6):349–356. [Google Scholar] [PubMed]
- 11. Wiegerinck JI, Kok AC, van Dijk CN. Surgical treatment for chronic retrocalcaneal bursitis. Knee Surg Sports Traumatol Arthrosc. 2011;19(8):1360–1366. [Google Scholar] [PubMed]
- 12. Nunley JA, Ruskin G, Bedi A. Partial calcaneal resection for Haglund’s deformity: long-term follow-up. Foot Ankle Int. 2015;36(7):808–814. [Google Scholar] [PubMed]
- 13. Mir BA, Mir GR, Ahmad S. Functional outcome of partial resection of calcaneal tuberosity for Haglund’s deformity. Int J Orthop Sci. 2016;2(4):139–143. [Google Scholar] [PubMed]
- 14. Ortmann FW, McBryde AM Jr. Surgical management of Haglund’s deformity. Foot Ankle Int. 2018;39(8):935–942. [Google Scholar] [PubMed]
- 15. Singh AV, Faraz S, Vijayaragavan R, Thirugnanasambanthan S. Surgical resection of Haglund’s deformity by Achilles tendon splitting approach. Int J Orthop Sci. 2021;7(4):255-258. [Google Scholar] [PubMed]
- 16. Banerjee R, Chao JC, Taylor R. Operative outcomes of calcaneal exostectomy for Haglund’s deformity. Foot Ankle Orthop. 2023;8(1):24730114231155784. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Aneurysmal Bone Cyst of Calcaneum in a Young Adult: A Rare Case Report
July 1, 2026 Aneurysmal Bone Cyst of Calcaneum in a Young Adult: A Rare Case Report July 1, 2026 All-Inside Versus Inside-Out Meniscal Repair: A Comparative Study of Healing Rates And Functional Outcomes
July 1, 2026 All-Inside Versus Inside-Out Meniscal Repair: A Comparative Study of Healing Rates And Functional Outcomes July 1, 2026 Role of Meniscal Ramp Lesion Repair in Preventing Residual Instability after Anterior Cruciate Ligament Reconstruction
July 1, 2026 Role of Meniscal Ramp Lesion Repair in Preventing Residual Instability after Anterior Cruciate Ligament Reconstruction June 1, 2026 Comparison of Radial Head Prosthesis versus Excision in Comminuted Radial Head Fractures: A Retrospective Comparative Study
June 1, 2026 Comparison of Radial Head Prosthesis versus Excision in Comminuted Radial Head Fractures: A Retrospective Comparative Study