
Despite advancement in our understanding of CTEV, relapsed, residual, and resistant cases do occur; early identification, proper treatment, and compliance with post-corrective splinting are essential to the successful management of these cases.
Dr. Faisal Harun, Department of Orthopaedic Surgery, Jawaharlal Nehru Medical College, Aligarh Muslim University, Aligarh, Uttar Pradesh, India. E-mail: dr.faisalharun@gmail.com
Abstract
Introduction: Congenital talipes equinovarus (CTEV) is a common pediatric deformity, with conservative management being the primary method of management. Even with appropriate management of CTEV, relapses can still occur, and some cases may present with residual deformities or prove resistant to treatment. The cause of these conditions is multifactorial, and there exists a difference of opinion regarding the management of such cases. The study aimed to provide clinically relevant outcome data in this specific and less frequently encountered population. The relatively small sample reflects the rarity of idiopathic relapsed, residual, and resistant CTEV and provides valuable preliminary data to guide future larger studies.
Materials and Methods: This prospective, descriptive, observational study included 33 clubfeet in 25 patients presenting with relapsed, residual, or resistant CTEV between July 2022 and June 2024. Patients were treated with either Ponseti’s method, including serial manipulation, casting, and tendo-achilles tenotomy, or Joshi’s external stabilization system (JESS), a minimally invasive external fixation technique. Pre- and post-correction outcomes were assessed using the Pirani and Dimeglio scoring systems. Data on treatment compliance, complications, and outcomes were analyzed.
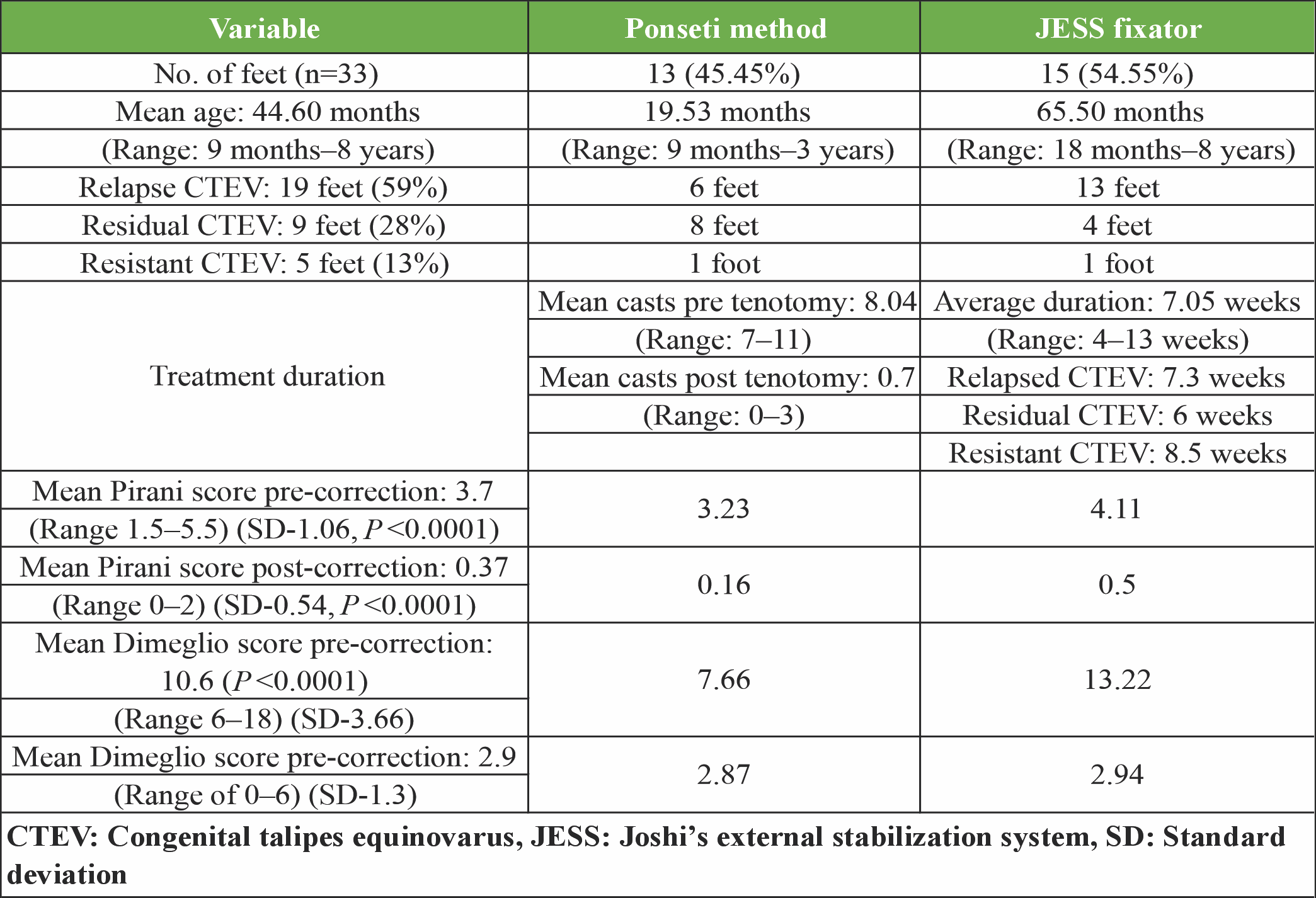
Results: The mean age of patients was 44.6 months, ranging from 9 months to 8 years. Among 33 feet, 19 were classified as relapsed (59%), 9 as residual (28%), and 5 as resistant CTEV (13%). Ponseti’s method was used for 45.45% of feet, and JESS for 54.55%. Post-correction Pirani scores improved significantly (mean pre-correction 4.11, post-correction 0.55; P < 0.001). Similarly, Dimeglio’s scores improved (mean pre-correction 13.22, post-correction 2.88; P < 0.001). Complications were minimal and manageable, including cast slippage and pin-tract infections. JESS demonstrated superior outcomes for older children with more severe deformities.
Conclusion: Both Ponseti’s method and JESS are effective for managing relapsed, residual, and resistant CTEV, with JESS particularly beneficial for older children. Recurrence is commonly associated with inadequate bracing and follow-up. Comprehensive management, including early treatment, patient education, and consistent follow-up, is crucial for achieving and maintaining correction.
Keywords: Congenital talipes equinovarus, Ponseti technique, Joshi’s external stabilization system, relapse congenital talipes equinovarus, recurrent congenital talipes equinovarus, residual congenital talipes equinovarus.
Congenital idiopathic clubfoot is the most common congenital foot deformity, affecting 1–2/1,000 live births [1]. The Ponseti method has become the gold standard conservative treatment, achieving high correction rates through serial manipulation, casting, and tendo-achilles tenotomy. However, despite these high corrective rates, relapsed, residual, and resistant cases do occur. Relapses, characterized by recurrence of equinus and varus deformity in previously corrected feet, occur rapidly in infants without adequate splinting and more slowly in older children, though they become rare after age 5 and almost nonexistent after age 7 [2,3]. The underlying pathophysiology of clubfoot predisposes feet to recurrence, and the causes of relapse, residual, and resistant conditions are multifactorial. Mild recurrences respond well to manipulation and casting, but management of more severe cases depends on patient age and severity. In children aged 2.5 years or older, anterior tibial tendon transfer may be considered, while posteromedial release addresses severe cases with tight tendons and joint capsules. Persistent forefoot adduction may require cuboid-cuneiform osteotomy in children aged 4–9 years [4,5]. Idiopathic relapsed, residual, and resistant clubfoot represents a relatively uncommon subset of congenital talipes equinovarus (CTEV). This presents a significant challenge for orthopedic practitioners, as there exists considerable variation in opinion regarding optimal management protocols for relapsed, residual, and resistant clubfoot. Minimally invasive techniques like Joshi’s external stabilization system (JESS) offer promising alternatives. JESS operates on the principle of controlled differential distraction, gradually lengthening the medial and lateral columns of the foot while promoting histogenesis. The system is semi-invasive, bloodless, and reduces the risk of complications, scarring, and fibrous tissue formation compared to conventional surgery. JESS applies tension within physiological limits to stimulate tissue regeneration according to the law of tension stress, ensuring a plantigrade foot while minimizing stress on growing epiphyses. Unlike the Ilizarov method, JESS is more suitable for young children with small feet due to its lighter design and greater flexibility [6,7]. This prospective, descriptive, observational study was conducted at a tertiary care center to evaluate to evaluate the management and outcomes of idiopathic relapsed, residual, and resistant clubfoot. The study was not powered for hypothesis testing but aimed to provide clinically relevant outcome data in this specific and less frequently encountered population, analyzing the demographic characteristics, treatment efficacy using validated scoring systems, and identifying associated factors.
Aims and objectives
- To study the demography of patients presenting with relapse, residual, and resistant idiopathic CTEV at Jawaharlal Nehru Medical College and Hospital
- To evaluate the effectiveness of various techniques (conservative and/or operative) in the management of such feet
- To study the possible causes of recurrence of deformities in relapse, residual, and resistant CTEV.
This prospective, descriptive, observational study was conducted in our tertiary care center from July 2022 to June 2024. Patients with relapsed, resistant, and residual types of CTEV who presented to the outpatient department were included in the study after obtaining approval from the institutional ethical committee (IEC Approval No: IECJNMC/835, Dated October 19, 2022) and parents’ consent. 33 clubfeet in 25 patients were included in the study. This sample size was considered adequate for descriptive analysis of treatment outcomes and complications and is consistent with previously published observational and pilot studies in pediatric orthopedic literature. They were managed conservatively by Ponseti’s method, followed by tendo achilles tenotomy or by controlled differential distraction method using JESS from the period from June 2022 to July 2024. As the primary aim was descriptive rather than hypothesis-driven, treatment was defined through pre-existing knowledge. Hence, the conservative or JESS application was done according to the surgeon’s decision.
Inclusion and exclusion criteria
All patients satisfying the criteria of relapse, resistant, and residual CTEV were included in the study. These conditions can be defined as follows:
- Relapse CTEV – A “relapse” can be defined as the recurrence of deformity in a previously well-corrected foot [3].
- Residual CTEV – Residual clubfoot, in which the foot was never fully corrected, but rather partially corrected, hence the term residual [3].
- Resistant CTEV- Resistant clubfeet are those that do not fully respond to standard methods of conservative treatment [3].
Patients with classic idiopathic CTEV and those with non-idiopathic clubfoot were excluded from the study. Grading of the various components of CTEV was done using the Pirani score and Dimeglio score preoperatively. Post correction, Pirani and Dimeglio scores were calculated as the outcome criterion. The Pirani scoring system assesses clubfoot severity by evaluating six clinical signs, divided equally between the hindfoot (posterior crease, empty heel, rigid equinus) and midfoot (medial crease, lateral curvature, reducibility of talar head). Each sign is scored as 0 (normal), 0.5 (moderately abnormal), or 1 (severely abnormal), based on visual inspection and palpation. The total score, ranging from 0 to 6, reflects the overall severity of the deformity and is commonly used to monitor response to treatment over time. In the Dimeglio scoring system, the examiner applies a gentle corrective force to assess the severity and flexibility of the deformity. The degree of equinus deviation in the sagittal plane, varus deviation in the frontal plane, derotation of the calcaneo-forefoot block, and forefoot adduction in the horizontal plane are each evaluated and scored from 0 to 4. In addition, the overall reducibility of the deformity, specifically equinus, varus, calcaneo-forefoot derotation, and forefoot adduction, is assessed as part of the scoring.
Management
Patients were managed conservatively by Ponseti’s method of serial manipulation and casting, followed by tendo-achilles tenotomy or by the controlled differential distraction method using JESS (Fig. 1).
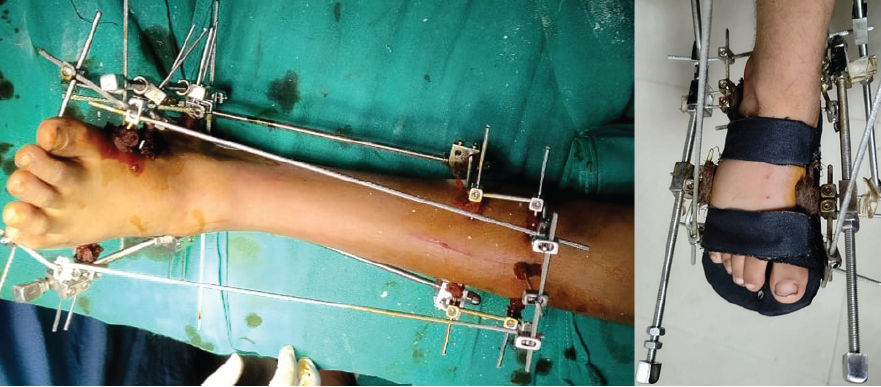
Figure 1: Joshi’s external stabilization system fixator applied in a patient with relapsed congenital talipes equinovarus.
Distraction begins on the 3rd post-operative day once the edema has subsided. Fractional distraction at a rate of 0.25 mm is applied at a single instance. Distraction on the medial side is done at twice the rate of the lateral side. This approach prevents crushing the articular cartilage and allows normal growth of the lateral epiphyseal plate, which might otherwise be affected by compression. For non-hospitalized patients, parents are instructed to perform distractions at a rate of 1 mm/day on the medial side and 0.5 mm/day on the lateral side. After correction is achieved, the fixator is kept in the same position for an additional 4 weeks to allow soft tissue stabilization and maturation in the corrected position, following which the entire assembly is removed in a single stage, and a plaster cast is applied for 3 weeks. Appropriate orthotic devices are crucial for maintaining correction and preventing recurrence during long-term follow-up. Once proper correction is achieved, it is maintained using Steenbeek foot abduction braces for patients under 6 years old, and ankle-foot orthoses for those over 6 years old (Fig. 2). Gait training is provided, and physiotherapy is recommended to strengthen the muscles. Manual stretching and light massage are also advised to maintain alignment and keep the foot flexible (Fig. 3 and 4).

Figure 2: Steenbeek foot abduction brace and ankle foot orthosis.
Gait training is provided, and physiotherapy is recommended to strengthen the muscles. Manual stretching and light massage are also advised to maintain alignment and keep the foot flexible (Fig. 3 and 4).

Figure 3: 9-month-old female with bilateral relapsed congenital talipes equinovarus managed conservatively by Ponseti technique.

Figure 4: 4-year-old male, with resistant congenital talipes equinovarus left foot which was managed by JESS application.
This study was conducted at a tertiary care center, in which a total of 228 patients were registered in the pediatric orthopedic clinic as CTEV during the study period from June 2022 to July 2024. Among these patients, 25 patients were included in the study for having recurrence in the form of relapse, residual, or resistant CTEV. Majority of the patient had poor compliance with the bracing protocol and had poor family educational status. The mean age of all cases was 44.60 months (range 9 months–8 years), with the mean age of patients managed with conservative means being 19.53 months (range 9 months–3 years) and those by operative methods being 65.5 months (range 18 months–8 years). Of the 25 patients, 16 were male and 9 were female, with 24 and 9 feet in both groups, respectively (M:F::1.7:1). 8 cases were bilateral and 17 cases were unilateral, of which 10 were right sided and 7 were left sided. The most common deformity was equinus (29/33 feet), followed by forefoot adduction (21/33 feet), hindfoot varus (18/33 feet), and cavus (15/33 feet). Out of a total of 33 feet, 19 feet were classified as relapsed CTEV (59%), 9 as residual CTEV (28%), and 5 as resistant CTEV (13%). 13 feet were managed by Ponseti method with repeat tenotomy (45.45%) while rest 15 cases were managed by JESS application (54.55%). Among the patients managed conservatively, cast slippage as a complication was noted in 5 patients, plaster sore was noted in 1 patient, and a superficial skin laceration occurred during cast removal with plaster cutter in 1 patient. In the patient group managed with JESS fixator, 4 patients had a metatarsophalangeal joint flexion deformity, 2 had an incidence of pin tract infection, and 1 had a unicortical fracture. All these complications were managed conservatively.
The incidence of congenital CTEV is about 1–2/1,000 live births, making it the most common congenital foot deformity [4]. There is still debate surrounding its causes, pathology, and treatment. Clubfoot not only poses cosmetic issues but also leads to physical disabilities, psychological distress, and financial strain on patients and their families. In developing countries, the early diagnosis and treatment of clubfoot are often delayed due to a lack of proper medical services and general unawareness. The urgency to begin treatment is frequently overlooked, resulting in many neglected cases. In addition, treatment compliance is a significant challenge in these regions. Regular follow-up visits are essential, but ignorance, a lack of adequately trained professionals, and limited transportation options contribute to a high number of recurrent cases [1]. Relapsed, residual, and resistant cases of CTEV present significant challenges for orthopedic practitioners worldwide. Only a few research articles have been published on relapse, residual, and resistant clubfoot. Thus, there is a lack of consensus regarding the management protocol of such cases. Khan and Kumar [8] evaluated the efficacy of the Ponseti technique in 25 neglected clubfeet in children older than 7 years (mean age, 8.9 years). The mean follow-up period was 4.7 years. The observed 85.7% of feet were fully corrected, with recurrence in 24% of feet. In 1989, Joshi [9] reported excellent outcomes in 60% of feet and good outcomes in 25% of feet in a study involving 90 feet using JESS. Lohia et al [10] in 2015 conducted study where a total of 50 feet with recurrent CTEV were divided into two groups where group I had children treated with Subtalar release and group II had children treated with controlled differential distraction with JESS. In Group I, 68% (17 feet) achieved excellent results and 32% (8 feet) had good results. In Group II, 64% (16 feet) achieved excellent results and 36% (9 feet) had good results out of 25 feet. All patients achieved a plantigrade foot by the end of treatment. Dhawan and Rana [11] studied a total of 30 children (34 feet) who were evaluated after correction with differential distraction using the JESS. The mean pre-operative Pirani score was 5 and mean post-operative Pirani score was 0.8. The overall results of the use of JESS fixators in the study were very encouraging with more than 90% with excellent Pirani scores. Rao M. et al. [12] (2022) conducted a study where a total of 44 feet (42 patients) were put on JESS for deformity correction and were followed for a minimum period of 14 months. The mean pre-correction Dimeglio score was 10.72 (8–13) and mean post-correction Dimeglio score was 3.34 (2–4). In the study, 40 patients showed satisfactory result and 2 patients showed unsatisfactory results. Anwar and Arun [13] reported 59.7% excellent and good results in clubfoot in which JESS fixators were used. The basic principle of external fixation in our study was the same as that advocated by Ilizarov. Tension and stress applied to the tissue within physiological limits stimulate histogenesis of tissues, while controlled differential distraction gradually corrects the deformities. JESS enables correction through soft tissue distraction. By means of controlled differential distraction, the JESS lengthens both the medial and lateral columns differently. This prevents injury to the articular surfaces, removes the preexisting contractures in the soft tissues, and realigns the joints [7,9]. Our study had a mean duration of JESS application was 7.05 weeks with a maximum duration of 13 weeks and minimum duration of 4 weeks, this was comparable to the study done by Lohia et al. [10], mean duration of 9.2 weeks, Rao et Al. [12] had a mean fixator duration of 4.06 weeks, while Gupta R et al. [14], mean fixator duration of 11.42 week, In our study, the mean pre-correction Pirani score was 4.11 which was reduced to 0.55 after correction with JESS with P < 0.001. Similarly, the mean pre-correction Dimeglio score was 13.22 which was reduced to 2.88 with P <0.001. Hence, our study shows that controlled differential distraction using JESS fixator is an effective method in the management of relapse, resistant, and residual CTEV.
The JESS fixators are particularly effective in young children because their tissues respond better to applied stress and have a greater remodeling potential compared to older patients with more rigid bony and soft tissue deformities. Unlike conventional surgery, the JESS frame minimizes scarring, preserves foot length, and produces a soft, flexible, plantigrade foot even after correcting significant deformities [7,9]. For children over 1 year old, the JESS fixator is preferred over the Ilizarov fixator due to its simpler application, lighter weight, shorter learning curve, reduced inventory needs, and lower cost. However, a drawback is that patients cannot walk while the fixator is in place. Post-correction casting is advised to protect osteopenic bones during pin-tract healing and to allow for gradual weight bearing. Complications, if rarely encountered, can be managed conservatively in most cases.
Limitations
Despite the comprehensiveness of the study, it does have certain limitations. There was no provision for randomization of patients for allotment in conservative or operative groups. This limits the comparisons that can be made regarding both management techniques. The relatively small sample size is acknowledged as a limitation; however, it reflects the rarity of idiopathic relapsed, residual, and resistant CTEV and provides valuable preliminary data to guide future larger studies.
Congenital idiopathic clubfoot, the most common congenital foot deformity, is typically treated with the Ponseti method, involving manipulation and serial casting. While effective for most cases, recurrence rates can reach up to 47%, especially in stiffer, more severe clubfeet with smaller calf muscles. Post-correction splinting, worn at night for three to 4 years, is crucial to prevent relapses, but premature discontinuation often leads to recurrence. Recurrences mainly affect the heel and are more easily managed with casting and manipulation. Management requires a comprehensive approach, including early treatment, consistent follow-up, and careful monitoring. In many cases, relapse can be addressed by repeating Ponseti’s method. Other surgical options for managing relapse, residual, and resistant clubfeet include tibialis anterior tendon transfer, postero-medial soft tissue release, TURCO’s procedure, and external fixators like the Ilizarov Ring fixator or JESS. Our study concluded that relapse and recurrent deformities are often caused by insufficient bracing and follow-up, and both Ponseti’s method and JESS fixator are effective treatments depending on the child’s age. However, our study had limitations, such as a small sample size, lack of radiographic follow-up, and a short follow-up duration of about 18 months. The study’s strength lies in its adherence to standard treatment protocols and regular assessment.
Despite advancement in our understanding of CTEV, relapsed, residual and resistant cases do occur. While both conservative and operative modalities have demonstrated excellent results, early identification, proper treatment and compliance to post corrective splinting is essential to the successful management of these cases.
References
- 1. Werler MM, Yazdy MM, Mitchell AA, Meyer RE, Druschel CM, Anderka M, et al. Descriptive epidemiology of idiopathic clubfoot. Am J Med Genet A 2013;161A:1569-78. [Google Scholar] [PubMed]
- 2. Dobbs MB, Rudzki JR, Purcell DB, Walton T, Porter KR, Gurnett CA. Factors predictive of outcome after use of the Ponseti method for the treatment of idiopathic clubfee. J Bone Joint Surg Amt 2004;86:22. [Google Scholar] [PubMed]
- 3. Eidelman M, Kotlarsky P, Herzenberg JE. Treatment of relapsed, residual and neglected clubfoot: Adjunctive surgery. J Child Orthop 2019;13:293-303. [Google Scholar] [PubMed]
- 4. Ponseti, I. V. Congenital Clubfoot : Fundamentals of Treatment. Oxford ; Oxford University Press, 1996. Print. NLM ID: 9603828 [Book]</p> [Google Scholar] [PubMed]
- 5. <p>5. Ponseti IV, Campos J. The classic: Observations on pathogenesis and treatment of congenital clubfoot. 1972. Clin Orthop 2009;467:1124-32. [Google Scholar] [PubMed]
- 6. Shah MZ, Khan A, Khan MS. Early experience with ilizarov for correction of resistant clubfoot. Pakistan Journal of Health and Medical Sciences Vol. 14, NO. 2, APR – JUN 2020. URL: https://pjmhsonline.com/2020/apr-june/595.pdf [Google Scholar] [PubMed]
- 7. Joshi: Treatment of CTEV by Joshi’s External Stabilizat… – Google Scholar. Available from: https://scholar.google.com/scholar_lookup?title=treatment%20of%20ctev%20by%20joshi%27s%20external%20stabilization%20system%20(jess)&author=b.b.%20joshi&publication_year=1999 [Last accessed on 2024 Aug 17]. [Google Scholar] [PubMed]
- 8. Khan SA, Kumar A. Ponseti’s manipulation in neglected clubfoot in children more than 7 years of age: A prospective evaluation of 25 feet with long-term follow-up. J Pediatr Orthop B 2010;19:385-9. [Google Scholar] [PubMed]
- 9. Joshi: Treatment of CTEV by Joshi’s External Stabilizat… – Google Scholar. Available from: https://scholar.google.com/scholar_lookup?title=Treatment%20of%20CTEV%20by%20Joshi%27s%20external%20stabilization%20system%20(JESS)&author=B.B.%20Joshi&publication_year=1999 [Google Scholar] [PubMed]
- 10. Lohia LK, Meena S, Kanojia RK. Comparative study of complete subtalar release and Joshi’s external stabilization system in the management of neglected and resistant idiopathic clubfoot. Foot Ankle Surg 2015;21:16-21. [Google Scholar] [PubMed]
- 11. Dhawan M, Rana N. Management of neglected, recurrent, and resistant congenital talipes equinovarus by controlled differential fractional distraction using the Joshi’s external stabilization system. Curr Med Res Pract 2019;9:176-81. [Google Scholar] [PubMed]
- 12. Rao M, Sahu C. Study of resistant, relapsed and neglected congenital talipes equinovarus treated by differential distraction using Joshi’s external stabilization system. Int J Med Sci Curr Res 2021;4:554-61. [Google Scholar] [PubMed]
- 13. Anwar MH, Arun B. Short term results of Correction of CTEV with JESS Distractor [Google Scholar] [PubMed]
- 14. J.Orthopaedics 2004;1(1)e3; URL: http://www.jortho.org/2004/1/1/e3 [Google Scholar] [PubMed]
- 15. Gupta, R., Kumar, K., & Jugran, P. (2019). A prospective study of neglected and resistant clubfoot cases treated using Joshi’s external stabilization system. International Journal of Research in Orthopaedics, 5(2), 227–231. https://doi.org/10.18203/issn.2455-4510.IntJResOrthop20185498. [Google Scholar] [PubMed] [CrossRef]






Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Clinical and Ultrasonographic Outcomes of Percutaneous Achilles Tenotomy Using an 18-Gauge Needle in Idiopathic Clubfoot: A Prospective Study
June 1, 2026 Clinical and Ultrasonographic Outcomes of Percutaneous Achilles Tenotomy Using an 18-Gauge Needle in Idiopathic Clubfoot: A Prospective Study March 1, 2026 Bilateral Clubfoot in Nail-Patella Syndrome: A Rare Syndromic Case Successfully Treated with the Ponseti Method
March 1, 2026 Bilateral Clubfoot in Nail-Patella Syndrome: A Rare Syndromic Case Successfully Treated with the Ponseti Method November 1, 2025 Easy Cast Removal in Idiopathic Congenital Talipes Equinovarus: A Study on Modified Ponseti Technique using an Interposed Polythene Sheet
November 1, 2025 Easy Cast Removal in Idiopathic Congenital Talipes Equinovarus: A Study on Modified Ponseti Technique using an Interposed Polythene Sheet July 1, 2025 An Observational Study on Pre-natal Diagnosis of Congenital Talipes Equinovarus
July 1, 2025 An Observational Study on Pre-natal Diagnosis of Congenital Talipes Equinovarus