
Ventromedial scapular osteochondroma is a rare but important cause of mechanical shoulder restriction, and complete excision leads to excellent functional recovery.
Dr. Jaydev Barapatre, Department of Orthopaedics, Jorhat Medical College and Hospital, Jorhat, Assam, India. E-mail: jaydevbarapatre@gmail.com
Abstract
Introduction: Ventromedial scapular osteochondroma is an uncommon cause of scapulothoracic impingement and shoulder restriction in children. Because of its deep anatomical location, diagnosis is often delayed, particularly in pediatric patients with minimal symptoms.
Case Report: A 9-year-old male presented with a gradually progressive, painless swelling over the left scapular region associated with difficulty in overhead shoulder movements for 1 year. Clinical examination revealed a firm, immobile bony mass over the posterior scapula with terminal restriction of shoulder abduction and forward elevation. Computed tomography demonstrated a pedunculated osteochondroma arising from the ventromedial surface of the scapula. The lesion was excised completely through a posterior approach. Postoperatively, the patient demonstrated marked improvement in shoulder range of motion with return to normal daily activities.
Conclusion: Timely surgical excision restores shoulder function and prevents progression of mechanical symptoms. Although rare, ventromedial scapular osteochondroma should be considered in the differential diagnosis of restricted shoulder mobility with unexplained scapular prominence in children, where it may mimic snapping scapula syndrome.
Keywords: Osteochondroma, scapula, ventromedial scapula, shoulder restriction, case report, pediatric orthopedics.
Ventromedial scapular osteochondromas may cause symptoms related to scapulothoracic articulation, including snapping, crepitus, pain, or mechanical restriction of shoulder movements. Because these symptoms are often attributed to muscular or postural causes, diagnosis is frequently delayed, especially in pediatric patients [1,2]. Awareness of this entity is therefore essential for orthopedic surgeons evaluating children with unexplained scapular swelling or shoulder dysfunction. Osteochondroma is the most common benign bone tumor, accounting for nearly one-third of all benign osseous neoplasms. It is characterized by a cartilage-capped bony projection that arises from the external surface of bone, maintaining continuity with the underlying cortex and medullary canal. These lesions typically develop during periods of skeletal growth and usually cease to enlarge after physeal closure. The majority of osteochondromas involve the metaphyseal regions of long bones such as the distal femur, proximal tibia, and proximal humerus. In contrast, involvement of flat bones is uncommon, with the scapula representing a rare site [3,4]. Scapular osteochondromas constitute a small fraction of cases, and lesions arising from the ventromedial surface are particularly rare. Previous reports have shown that scapular osteochondromas are most commonly present with mechanical symptoms related to scapulothoracic impingement, including restricted shoulder elevation, snapping scapula syndrome, or cosmetic deformity. Imaging plays a crucial role in confirming diagnosis and surgical planning [5]. Complete excision, including removal of the cartilage cap, has been consistently associated with excellent functional outcomes and low recurrence rates.
A 9-year-old male presented with a gradually progressive, painless swelling over the left scapular region for approximately 1 year, associated with increasing difficulty in performing overhead activities. There was no history of trauma, constitutional symptoms, or similar complaints among family members. The patient primarily reported mechanical restriction during shoulder elevation, without pain at rest.
Clinical examination
Inspection – A firm, immobile bony mass over the posterior aspect of the left scapula, with a visible winging-like prominence of the left scapula during rest, which became more pronounced during abduction. Palpation – A hard, non-tender, immobile mass was palpable deep to the medial border of the scapula. Range of motion – Terminal restriction was noted in forward elevation (150°) and abduction (140°). External and internal rotations were preserved. The presentation was consistent with pseudo-winging due to a scapulothoracic lesion (Fig. 1). Neurological status – distal neurovascular status and long thoracic nerve function were intact.

Figure 1: Pre-operative scapular prominence. Pre-operative clinical photograph of the patient in standing position, posterior view, showing a visible bony prominence over the left scapular region. The image demonstrates asymmetry of the left scapula during shoulder positioning prior to surgical intervention.
Investigations
Initial X-rays were suggestive but inconclusive due to the overlapping of the rib cage. Computed tomography of the left scapula demonstrated a well-defined, pedunculated bony lesion arising from the ventromedial surface, with continuity of cortical and medullary bone, consistent with an osteochondroma (Fig. 2). In view of the progressive mechanical symptoms and clear radiological correlation, surgical excision was considered the most appropriate management option.

Figure 2: Computed tomography of ventromedial scapular osteochondroma. Pre-operative computed tomography scan of the left scapula with three-dimensional reconstruction, demonstrating a well-defined pedunculated bony outgrowth arising from the ventromedial surface of the scapula, consistent with osteochondroma, obtained during pre-operative evaluation.
Surgical treatment
Under general anesthesia, the patient was placed in a prone “chicken-wing” position (arm internally rotated and backward) to distract the scapula from the chest wall. A longitudinal incision was made along the medial border of the scapula. The trapezius and rhomboids were retracted. The lesion was identified on the costal surface. An en bloc excision was performed at the base of the stalk using an osteotome. Special care was taken to excise the entire cartilaginous cap to minimize the risk of recurrence. The excised specimen was consistent with osteochondroma on gross examination (Fig. 3, Fig. 4). The post-operative period was uneventful.

Figure 3: Excised osteochondroma specimen showing length. Gross specimen photograph of the excised osteochondroma placed on the operative table, demonstrating the cartilaginous cap and underlying bony stalk immediately after surgical removal. The specimen is oriented to demonstrate the longitudinal dimension 4 cm of the lesion.

Figure 4: Excised osteochondroma specimen showing breadth. Gross specimen photograph of the excised osteochondroma placed on the operative table, demonstrating the cartilaginous cap and underlying bony stalk immediately after surgical removal. The specimen is oriented to demonstrate the transverse dimension 2.4 cm of the lesion.
Follow up
Histopathology confirmed the diagnosis of a benign osteochondroma with no evidence of malignant transformation. At 6-week follow-up, the surgical wound had healed satisfactorily, with restoration of scapular contour and significant improvement in shoulder range of motion. Post-operative radiographs confirmed complete excision of the lesion (Fig. 5), and clinical evaluation at 6 weeks showed restoration of scapular contour (Fig. 6), the patient returned to routine activities without restriction.
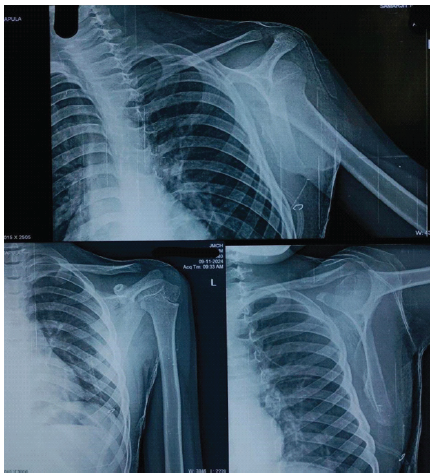
Figure 5: Immediate post-operative shoulder radiograph. Immediate post-operative radiograph of the left shoulder in anteroposterior view, obtained following surgical excision, confirming complete removal of the scapular lesion with restoration of normal scapular contour.

Figure 6: Six-week post-operative clinical outcome. Post-operative clinical photograph of the patient in standing position, posterior view, taken 6 weeks after surgery, showing resolution of scapular prominence with satisfactory cosmetic appearance and restoration of shoulder function.
Osteochondromas involving the scapula are rare, and ventromedial lesions are particularly uncommon due to the flat anatomy and extensive muscular coverage of this region; these lesions represent benign developmental lesions that may arise at atypical skeletal sites with characteristic histopathological features confirming their non-neoplastic nature [6,7]. The clinical presentation of ventromedial scapular osteochondroma may mimic other causes of scapulothoracic dysfunction, including snapping scapula syndrome, scapulothoracic bursitis, or muscular imbalance. As seen in our case, clinical presentation often mimics “pseudo-winging.” While plain radiographs (specifically the “Scapular Y” view) can identify the lesion, three-dimensional computed tomography is particularly useful for defining the stalk’s orientation and its proximity to the thoracic cage, which is vital for safe surgical clearance. In our patient, excision of the ventromedial lesion led to resolution of pseudo-winging and unrestricted overhead activity, mirroring outcomes reported in previous pediatric cases. The “chicken-wing” positioning is crucial for access. We recommend a posterior approach along the medial border as it provides the safest corridor to the ventromedial surface while minimizing damage to the serratus anterior and long thoracic nerve. This case emphasizes the need to consider ventromedial scapular osteochondroma in children presenting with unexplained scapular swelling or shoulder movement restriction. Complete excision of the cartilage cap is critical to avoid recurrence [8,9,10]. Longer follow up is planned to monitor recurrence and functional outcomes. A review of the PubMed/Medline literature indicates that symptomatic scapular osteochondromas are most effectively managed with complete surgical excision. Complete removal of the cartilage cap is essential to prevent recurrence. Various surgical approaches have been described, with the choice guided by lesion location and surgeon preference.
This case demonstrates ventromedial scapular osteochondroma as a rare but clinically significant cause of mechanical shoulder restriction in children. The report highlights the diagnostic challenge posed by its deep anatomical location and non-specific presentation, which can lead to delayed recognition. Our findings emphasize that early diagnosis using appropriate cross-sectional imaging, followed by complete surgical excision including the cartilage cap, results in excellent functional and cosmetic outcomes. This case contributes to existing orthopedic literature by reinforcing the need for a high index of suspicion in pediatric patients with unexplained scapular prominence and restricted shoulder motion, thereby advancing clinical understanding of this uncommon pathology and its optimal surgical management.
Ventromedial scapular osteochondroma is an uncommon cause of mechanical shoulder restriction in children. This case underscores the need for early consideration of ventromedial scapular osteochondroma in children presenting with unexplained scapular prominence and restricted shoulder movement, as recognition of this rare lesion allows timely referral for surgical management, thereby reducing symptom duration and avoiding repeated or unnecessary investigations.
References
- 1. Kitsoulis P, Galani V, Stefanaki K, Paraskevas G, Karatzias G, Agnantis NJ, et al. Osteochondromas: Review of the clinical, radiological and pathological features. In Vivo 2008;22:633-46. [Google Scholar] [PubMed]
- 2. Singh S, Sharma V, Jain V. Osteochondroma of the scapula presenting as scapulothoracic impingement: Clinical features and surgical outcomes. J Clin Orthop Trauma 2021;18:120-4. [Google Scholar] [PubMed]
- 3. Fageir MM, Edwards MR, Addison AK. Osteochondroma of the scapula presenting as snapping scapula syndrome. J Shoulder Elbow Surg 2009;18:e1-3. [Google Scholar] [PubMed]
- 4. Kumar R, Madewell JE, Swischuk LE. Benign bone tumors of childhood. Radiographics 1990;10:1029-49. [Google Scholar] [PubMed]
- 5. Wiater JM, Flatow EL. Long thoracic nerve injury. Clin Orthop Relat Res 1999;368:17-27. [Google Scholar] [PubMed]
- 6. Albrecht S, Crutchfield JS, SeGall GK. On spinal osteochondromas. J Neurosurg 1992;77:247-52. [Google Scholar] [PubMed]
- 7. Dorfman HD, Czerniak B. Bone Tumors. St Louis: Mosby; 1998. [Google Scholar] [PubMed]
- 8. Unni KK, Inwards CY. Dahlin’s Bone Tumors: General Aspects and Data on 10,165 Cases. Philadelphia, PA: Lippincott Williams and Wilkins; 2009. [Google Scholar] [PubMed]
- 9. Heck RK. Benign bone tumors and nonneoplastic conditions. Instr Course Lect 2002;51:455-64. [Google Scholar] [PubMed]
- 10. Resnick D. Diagnosis of Bone and Joint Disorders. 4th ed. Philadelphia, PA: Saunders; 2002. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor
July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor July 1, 2026 Beyond the Biopsy: Macrodystrophia Lipomatosa Unmasked After False Osteochondroma Diagnosis
July 1, 2026 Beyond the Biopsy: Macrodystrophia Lipomatosa Unmasked After False Osteochondroma Diagnosis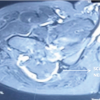 July 1, 2026 Large Posterior Proximal Femur Osteochondroma Presenting in Adulthood – Diagnostic Challenges and Management Strategy: A Case Report
July 1, 2026 Large Posterior Proximal Femur Osteochondroma Presenting in Adulthood – Diagnostic Challenges and Management Strategy: A Case Report December 1, 2025 A Heavy Burden on the Back: Surgical Excision of a Massive Scapular Osteochondroma – A Case Report
December 1, 2025 A Heavy Burden on the Back: Surgical Excision of a Massive Scapular Osteochondroma – A Case Report