
• Gossypiboma is a preventable surgical event that has adverse consequences on patient health • It has legal implications on the hospital and may disrepute the surgeon • Strict practice of the WHO Surgical safety checklist plays a vital role in prevention • In cases presenting with early Surgical Site Infection: Retained gauze in the surgical field should be considered as a cause and rectified for faster recovery
Dr. Purushotham Lingaiah, Department of Orthopaedics, All India Institute of Medical Sciences, Mangalagiri, Andhra Pradesh, India. E-mail: puru@aiimsmangalagiri.edu.in
Abstract
Introduction: Inadvertent retention of surgical cotton gauze or cotton material in the surgical field is described as Gossypiboma. It is a rare event in orthopedic surgery, and hence the diagnosis is obscured in the setting of early surgical site infection (SSI) and is often initially mistaken with breach in the aseptic technique, improper autoclaved instruments, long duration of surgery, poor surgical environment, or decreased immunity of the patient.
Case Report: We present a case of SSI of the hip with impending sepsis in an elderly female with a missed diagnosis of retained cotton mop at the surgical site. Thorough evaluation of the post-operative radiographs helped arrive at the diagnosis. Debridement, removal of the mop, and antibiotic coverage, with watchful post-operative progress, were vital in healing of the wound.
Conclusion: Gossypiboma is a preventable surgical error. The aim of this study is to emphasize the importance of the surgical safety checklist, which largely contributes to safe patient care. Retained gauze piece must be considered in the evaluation of early SSI at the outset to prevent devastating consequences.
Keywords: Gossypiboma, surgical site infection, surgical safety checklist.
Accidentally retained surgical swabs/guaze piece or mops in the surgical field are a rare event in the present world. The rarity may be attributed to the diligent implementation of the World Health Organization (WHO) surgical safety checklist and/or underreporting of such cases [1]. Gossypiboma and textiloma are the technical terms used to describe this surgical complication [2]. This type of operative complication is more frequently seen in surgeries exposing large operative fields, such as abdominal and thoracic surgeries [3]. In Orthopedics, the most common sites are the hip and spine. Diagnosis of Gossypiboma is usually obscured in the majority of cases, as they remain asymptomatic for many years. In symptomatic cases, it is revealed as the occurrence of surgical site infection (SSI) secondary to a foreign body [4]. The diagnosis is mostly made by plain radiographs, computed tomography, and by ultrasound [5]. Thorough debridement, mop removal, and antibiotic coverage are key to complete recovery. Gossypiboma is largely preventable. In this report, the importance of the surgical safety checklist for prevention and vigilant evaluation of post-operative radiographs for early diagnosis are highlighted.
A 78-year-old female underwent surgery for an intertrochanteric fracture of the right femur for which internal fixation with a Proximal Femoral Nail was performed in a peripheral hospital. Review of operative notes stated that intra-operatively, there was an iatrogenic femur shaft oblique fracture treated with two stainless steel (SS) wire cerclages. Blood loss was approximately 1800 mL. On the 7th post-operative day, there was pus discharge from the middle surgical incision site. The proximal entry incision and the distal locking screw site incision were normal. The infected wound was debrided and left open. Intravenous (IV) antibiotic coverage was given. Patient presented to our institute 3 weeks later with the pouring pus open wound. The diagnosis of deep SSI was made. Wound examination showed infected granulation tissue (Fig. 1).

Figure 1: Open surgical site wound on the lateral aspect of the right thigh with infected granulation tissue.
The SS wire cerclage could be felt through the wound. Pus was sent for microbial culture and sensitivity. Patient was anemic (Hemoglobin – 7.1 g/dL), poorly nourished (Total proteins – 4.1, Serum albumin – 1.9), and hypertensive on medication. Her White blood cell counts were high normal; Erythrocyte sedimentation rate was high; and C-reactive protein level was elevated.
Pus culture from her previous hospital reports showed growth of Escherichia coli sensitive to Amikacin and Tigecycline. Plain radiograph of the thigh showed a tortuous, crumpled X-ray detectable thread, which was suggestive of abdominal mop (Fig. 2).
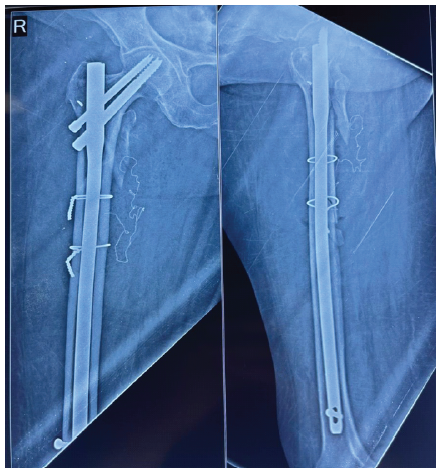
Figure 2: Post-operative plain radiograph showing tortuous X-ray detectable thread-like material medial to the proximal femur.
In the setting of immediate post-operative SSI and the X-ray finding, the diagnosis of retained mop/Gossypiboma was made. After optimization of her physiological parameters, the wound was debrided under anesthesia. The mop was removed. A thorough wound wash was given. The dead space and the surgical site were then filled with Stimulan (absorbable calcium sulfate antibiotic carrier) mixed with Vancomycin and Amikacin (Fig. 3). The wound was closed under a deep and a superficial suction drain.

Figure 3: Radiograph showing stimulan beads filled in the void after mop removal.
Outcome
Intra-operative pus culture showed E. coli sensitive to Amikacin and Meropenem. Accordingly, IV antibiotics were started. A high-protein diet was started. The drain output on post-operative day 1 was 200 mL, which gradually decreased over a week. Drain was removed on post-operative day 7. Daily wound inspection was found to be dry and healthy. No evidence of re-infection was seen. Inflammatory markers done every 3rd day showed a decreasing trend (Table 1).
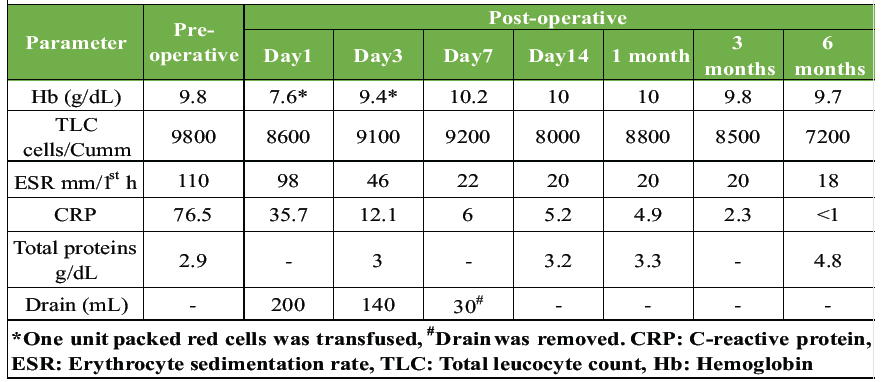
Table 1: Inflammatory and nutrition parameters
Patient was afebrile. She was ambulated with partial toe-touch. IV antibiotics were continued for 2 weeks and then oral antibiotics were given for 4 weeks.
Follow-up
Sutures were removed on post-operative day 15. Regular follow-up at 4 weeks, 2, 3, 6, and 12 months did not show any clinical, biochemical, or radiological signs of infection (Fig. 4 and 5).

Figure 4: Well-healed surgical site at 1-year follow-up.
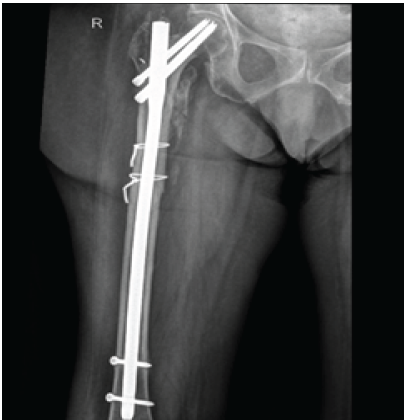
Figure 5: Radiologically healed fracture with no signs of infection at 1 year follow-up.
Inadvertent retention of surgical cotton gauze or cotton material in the surgical field is described as Gossypiboma [1]. It is a rare event in orthopedic surgery and hence the diagnosis is obscured in the setting of early SSI and is often initially attributed to breach in the aseptic technique, improper autoclaved instruments, long duration of surgery, poor surgical environment, or decreased immunity of the patient. Gossypiboma is an unwanted surgical complication that not only has deleterious effects on the health of the patient but also brings disrepute to the surgeon and the hospital [6]. Although the National Quality Forum of the United States of America and the patient safety guidelines issued by the Health Department of the United Kingdom have declared that the presence of a retained surgical sponge to be a “never event” and should be avoided at all cost, it is not completely eliminated [7,8]. Several risk factors are associated with Gossypiboma, such as obesity, intraoperative surgical protocol modification, emergency surgery, severe blood loss, long duration of surgery, and non-counting of swabs during surgery [9]. In our case, factors, such as high-volume blood loss and long duration of surgery were present. After analysis of initial surgery notes, it was hypothesized that mops would have been placed to achieve hemostasis while the iatrogenic shaft fracture was being fixed and the post-operative radiographs were not thoroughly assessed. The rarity of Gossypiboma in Orthopedic Surgery makes a low index of suspicion in cases of early SSI leading to persistent infection. Gossypiboma can present in two ways: The aseptic fibrous type, which remains asymptomatic and is detected accidentally during the evaluation of an unrelated symptom, and the exudative type, which is characterized by abscess formation and early presentation [10]. Aseptic type, being a commoner type has been documented in literature [10,11,12,13,14]. A review is presented in the tabulated form, which shows the modes of presentation, diagnostic modalities, and management (Table 2). In our case, the presentation was clearly an exudative type with persistent pus discharge. The infection, however, was confined to the local site with no systemic complication.
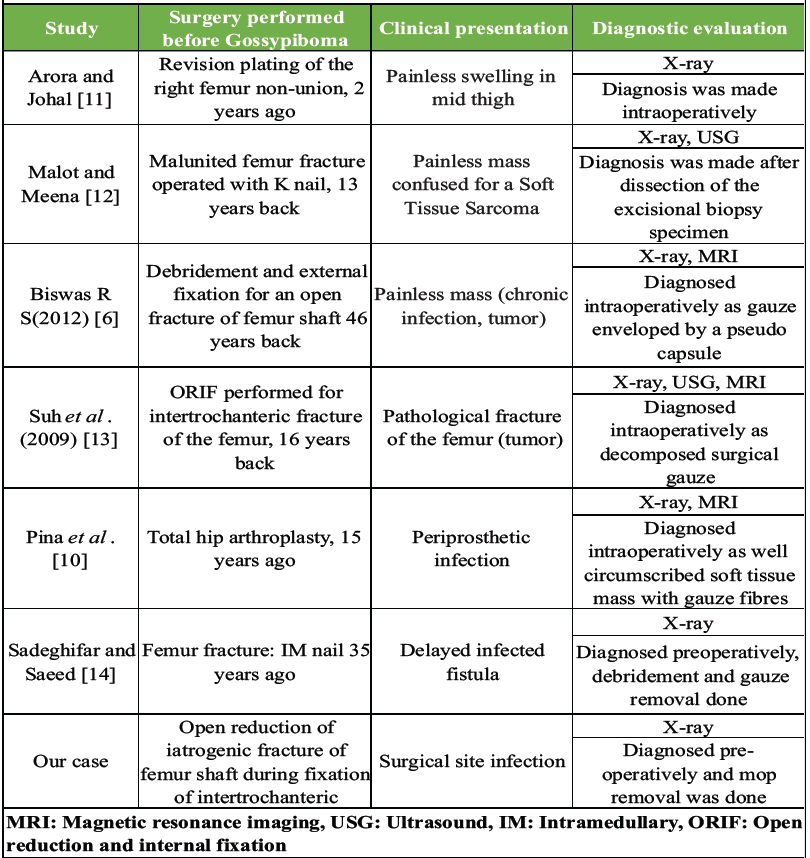
Table 2: Review of previously reported cases of Gossypiboma in the thigh after orthopedic surgery
Gossypiboma can have serious ethical and medicolegal implications. It is considered as a medical negligence and the whole team, which includes the surgeons, the anesthetist team, nurses, and support staff, should feel responsible for not adhering to standard operative guidelines [15]. Hence, all attempts must be made to avoid the consequences of this surgical complication. Proper pre-operative planning, intra-operative alertness, and post-operative inspection before closure of the wound can be immensely helpful in prevention. Strict compliance to the WHO Surgical safety checklist is a simple and effective way to avoid complications. Despite all measures, this event may still occur. Every hospital/Institute should develop patient safety guidelines in operation theatres to completely eliminate this preventable complication.
Gossypiboma is a preventable surgical event that has adverse consequences on patient health and legal implications on the hospital. Strict practice of the surgical safety checklist plays a vital role in its prevention. In cases presenting with early SSI, retained gauze or foreign material in the surgical field should be considered as a cause and rectified for faster recovery.
Retained gauze after surgery is a preventable complication and may be asymptomatic for a very long period, but can become a complication post-operatively at any time. Hence, if diagnosed immediately after the surgery or at any other time, the gauze should be removed.
References
- 1. WHO. Surgical Safety Checklist and Implementation Manual. Available from: https://www.who.int/patientsafety/safesurgery/ss_checklist/en [Last accessed on 2015 Oct 10]. [Google Scholar] [PubMed]
- 2. Cima RR, Kollengode A, Garnatz J, Storsveen A, Weisbrod C, Deschamps C. Incidence and characteristics of potential and actual retained foreign object events in surgical patients. J Am Coll Surg 2008;207:80-7. [Google Scholar] [PubMed]
- 3. Rappaport W, Haynes K. The retained surgical sponge following intra-abdominal surgery. A continuing problem. Arch Surg 1990;125:405-7. [Google Scholar] [PubMed]
- 4. Akhaddar A, Baallal H, Elktaibi A. Abscess due to textiloma (gossypiboma: Retained surgical cottonoid). Surg Neurol Int 2018;9:70. [Google Scholar] [PubMed]
- 5. Singh S, Chanu SM, Sharmila V, Yugandhar S, Reddy PA. Surgical safety spotlight: Gossypiboma – rare but real. J Patient Saf Infect Control 2023;11:57-9. [Google Scholar] [PubMed]
- 6. Biswas RS, Ganguly S, Saha ML, Saha S, Mukherjee S, Ayaz A. Gossypiboma and surgeon- current medicolegal aspect – a review. Indian J Surg 2012;74:318-22. [Google Scholar] [PubMed]
- 7. National Quality Forum. Serious Reportable Events in Healthcare – 2011 Update. Washington DC: National Quality Forum; 2011. [Google Scholar] [PubMed]
- 8. Department of Health. The ‘Never Events’ List 2011/12. London: Department of Health; 2011. [Google Scholar] [PubMed]
- 9. Gawande AA, Studdert DM, Orav EJ, Brennan TA, Zinner MJ. Risk factors for retained instruments and sponges after surgery. N Engl J Med 2003;348:229-35. [Google Scholar] [PubMed]
- 10. Pina G, Pereira D, Borralho N, Sousa M. Gossypiboma and total hip arthroplasty — a rare accidental finding following a periprosthetic infection. J Orthop Case Rep 2021;11:76-9. [Google Scholar] [PubMed]
- 11. Arora RK, Johal KS. Gossypiboma in thigh- a case report. J Orthop Case Rep 2014;4:22-4. [Google Scholar] [PubMed]
- 12. Malot R, Meena DS. Gossypiboma of the thigh mimicking soft tissue sarcoma: Case report and review of literature. J Orthop Case Rep 2012;2:21-4. [Google Scholar] [PubMed]
- 13. Suh DH, Yoon JR, Kang KB, Han SB, Kim HJ, Lee SJ. A gossypiboma-induced pathological fracture of the proximal femur. Clin Radiol 2009;64:1132-5. [Google Scholar] [PubMed]
- 14. Sadeghifar AR, Saeed AR. Infected textiloma, 35 years after the operation for femur fracture, an extermly rare occurance. Arch Bone Jt Surg 2013;1:41-3. [Google Scholar] [PubMed]
- 15. Wan W, Le T, Riskin L, Macario A. Improving safety in the operating room: A systematic literature review of retained surgical sponges. Curr Opin Anaesthesiol 2009;22:207-14. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Effect of Intrawound Vancomycin Powder as an Adjunct to SystemicAntibiotic Prophylaxis on Surgical Site Infection Following Open TibialFracture Fixation: A Randomized Prospective Study
May 1, 2026 Effect of Intrawound Vancomycin Powder as an Adjunct to SystemicAntibiotic Prophylaxis on Surgical Site Infection Following Open TibialFracture Fixation: A Randomized Prospective Study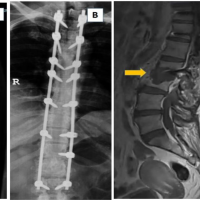 March 10, 2024 Distal Junctional Failure due to Spondylodiscitis in a Patient with Long Posterior Fixation for Ossified Longitudinal Ligament and Ossified Ligamentum Flavum
March 10, 2024 Distal Junctional Failure due to Spondylodiscitis in a Patient with Long Posterior Fixation for Ossified Longitudinal Ligament and Ossified Ligamentum Flavum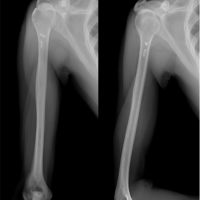 August 10, 2022 Rare Case of Non-tuberculous Mycobacterial Infection following Repair of Pectoralis Major Avulsion: Case Report and Review of Literature
August 10, 2022 Rare Case of Non-tuberculous Mycobacterial Infection following Repair of Pectoralis Major Avulsion: Case Report and Review of Literature June 13, 2021 Gossypiboma and Total Hip Arthroplasty-A Rare Accidental Finding Following a Periprosthetic Infection
June 13, 2021 Gossypiboma and Total Hip Arthroplasty-A Rare Accidental Finding Following a Periprosthetic Infection