
Early recognition of spinal tuberculosis and timely initiation of appropriate therapy are crucial to prevent irreversible neurological complications and disability.
Dr. Dinesh Kumar, Department of General Medicine, Tata Main Hospital, West Bokaro, Noamundi, Jharkhand, India. E-mail: drdineshnoa@gmail.com
Abstract
Introduction: Extrapulmonary tuberculosis (TB) can involve the spine, presenting as Pott’s disease. Patients typically develop back pain, and complications, such as psoas abscess and paraplegia may occur if diagnosis is delayed. A high index of suspicion and gadolinium-enhanced magnetic resonance imaging (MRI) are essential for early detection. Timely treatment helps prevent neurological deficits. We report the case of a 55-year-old afebrile man with progressive lower-limb weakness, unexplained weight loss, and an atraumatic vertebral fracture. MRI revealed classic cold abscesses consistent with Pott’s disease of the lumbar spine, along with bilateral psoas abscesses. The patient showed good clinical recovery with conservative management using anti-tuberculous therapy. Spinal TB is a common form of extrapulmonary TB and may present with back pain, deformity, paraparesis, or psoas abscess. MRI is the preferred imaging modality. Early identification is crucial to prevent disability. This report describes a lumbar Pott’s spine with bilateral psoas abscess presenting as progressive paraparesis.
Case Report: A 55-year-old male presented with a 4-month history of worsening lower-limb pain, numbness, and weakness, along with weight loss and poor appetite. He had no fever, trauma, or respiratory symptoms. Examination showed lower-limb muscle wasting with preserved distal movements. MRI revealed D12/L1 spondylodiscitis with Grade 1 vertebral collapse, peripheral epidural abscess, and bilateral psoas abscesses. Laboratory tests showed lymphocytosis and significantly elevated erythrocyte sedimentation rate. Histopathology demonstrated granulomatous inflammation with caseation, and Mycobacterium TB was confirmed on acid-fast bacillus smear and polymerase chain reaction. The patient was started on Category-2 anti-TB treatment (ATT) (H, R, Z, E with pyridoxine). Hepatotoxicity required temporary cessation of HRZ; later H and R were reintroduced, Z was discontinued, and levofloxacin was added. He was managed conservatively with a long Taylor brace and multidisciplinary care.
Conclusion: Progressive paraparesis with atraumatic vertebral collapse should raise suspicion for Pott’s spine with possible psoas abscess. Early MRI, microbiological confirmation, and timely individualized ATT – alongside careful monitoring for drug toxicity – are vital to prevent irreversible neurological damage. Conservative management can result in substantial recovery.
Keywords: Pott’s disease, spinal tuberculosis, bilateral psoas abscess, paraparesis
Tuberculosis (TB) affects individuals across all demographics, with spinal TB constituting 2% of all TB cases and 15% of extrapulmonary cases. It accounts for nearly 50% of cases involving osteoarticular TB, which primarily affects the hip and knee joints [1] Statistics from 2018 indicate that 57% of reported cases were in men over 15 years old, followed by women at 32% and children under 15 at 11% [2]. Individuals living with human immunodeficiency virus (HIV) face a 20–37 times higher risk of developing TB compared to those who are not infected [3]. Vertebral TB, the most prevalent form of skeletal TB, frequently occurs in the first three decades of life, although it can affect patients ranging from 1 to 80 years old [4]. Delay in diagnosis and treatment initiation can lead to severe and irreversible neurological complications, including paraplegia. Vertebral TB is paucibacillary, and the spread is mostly hematogenous, followed by lymphatic or contiguous spread. As the spine is a cancellous bone and is dense and vascular, it often acts as a nidus for hematogenous spread and, so, is a common site for TB. In the skeletal system, TB may affect bones, joints, and the synovial system. The damage to these structures is mediated through hyperemia-induced osteopenia, caseous necrosis, granuloma formation, and finally causes pathological fracture [5]. Symptoms suggestive of TB, such as fever, loss of appetite, and loss of weight, can be seen at presentation in only half of patients. A diagnosis is usually found three to 4 months after the start of symptoms. Spinal TB should be suspected if the following symptoms are present: Fever and weight loss; persistent localized back or neck pain for more than 1 month; spinal tenderness; spinal cord compression with nerve root pain, cauda equina syndrome, paraplegia, or paraparesis; paraspinal muscle wasting; spinal deformity; and kyphosis. Failure to thrive, inability or difficulty in walking, and use of hands to support the head or trunk can be found in children.
The case presentation patient was a 55-year-old male who reported experiencing pain and weakness in his lower limbs over the previous 4 months, which progressively worsened despite treatment with analgesics. He had experienced numbness in his lower limbs for several days before his admission. There was no history of prior injury, and the patient was afebrile with no symptoms of chills. He did, however, experience general weakness, lack of appetite, drowsiness, apathy, and weight loss. There were no respiratory symptoms, such as a productive cough. Clinical examination revealed atrophy of the lower limb muscles, although he was still able to move his feet.
Imaging, including magnetic resonance imaging (MRI), confirmed a diagnosis of spondylodiscitis at the D12/L1 level, characterized by a Grade 1 collapse of both vertebral bodies, heterogeneous enhancement, a peripheral enhancing epidural abscess, and involvement of the psoas muscles, resulting in psoas abscess formation (Fig. 1 and 2).

Figure 1: Diagnosis of spondylodiscitis at the D12/L1 level, sagittal view.

Figure 2: Diagnosis of spondylodiscitis at the D12/L1 level, coronal view.
Laboratory investigations at different intervals of case management are shown in Tables 1, 2, 3, 4.
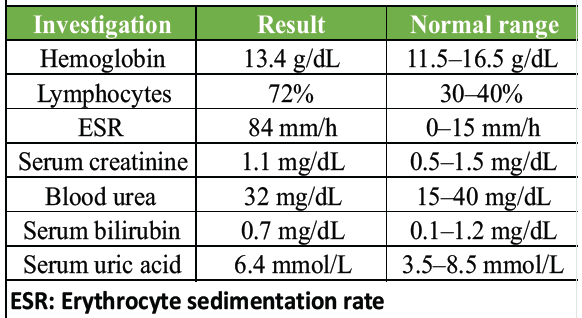
Table 1: At the start of treatment
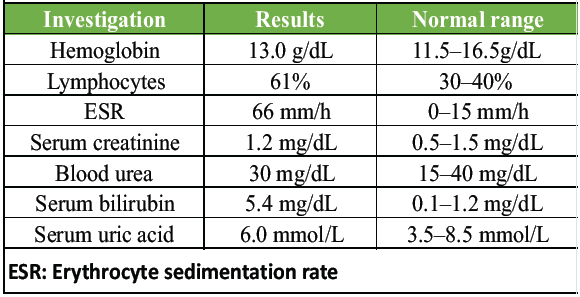
Table 2: After 1 week of starting the treatment
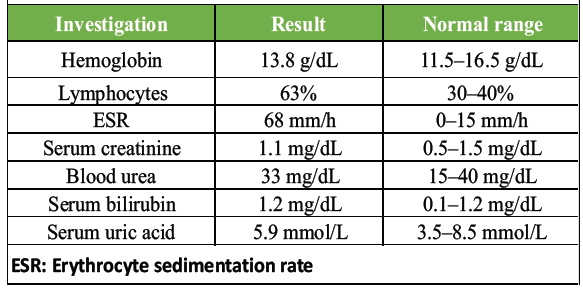
Table 3: After withholding anti-tuberculosis treatment for 1 week
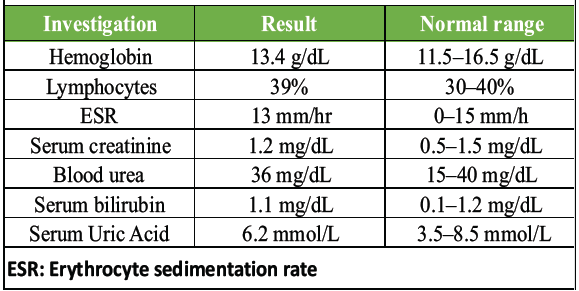
Table 4: After 1 month of treatment
Chest radiography revealed no abnormalities in the lungs, while the Mantoux test was returned positive. Both acid-fast bacilli and polymerase chain reaction tests from cultures of the abscess and surrounding soft tissues were positive for mycobacterium TB. Histological examination indicated granulomatous inflammation with central caseous necrosis, Langerhans giant cells, and epithelioid cells encircled by lymphocytes.
The patient was initiated on anti-TB treatment (ATT) Category 2, which included isoniazid (H), ethambutol (E), rifampicin (R), pyrazinamide (Z), and pyridoxine supplements. A long Taylor brace was also applied. After a few days, liver function tests showed abnormalities, leading to the discontinuation of HRZ, while E was continued. H and R were later reintroduced gradually without hepatotoxicity. Z was permanently stopped as it was suspected to be the cause of liver damage. Subsequently, levofloxacin (L) was added to the HREL regimen.
In addition to medical management, the patient received conservative care, with a multidisciplinary team approach involving specialists in infectious diseases, orthopedic surgery, and rehabilitation therapy. The patient exhibited significant improvements in both symptoms and functional outcomes. This case emphasizes the importance of early recognition and treatment of tuberculous spondylitis to mitigate complications and prevent disability.
Management strategies
Management of spinal TB should be conducted through a multidisciplinary approach. Medical therapy using anti-tuberculous medications forms the foundation of treatment, typically employing a multidrug regimen that includes HRZ and E over an extended duration. Two months of HRZE (the intensive phase) should be followed by 10 months of HRE (the continuation phase). The duration of treatment is 12 months, which can be extended to 18 months as needed.
Follow-up
Regular follow-ups for patients with spinal TB are crucial to assess the need for surgical intervention. The following protocol should be adhered to during follow-ups. Patients with neurological deficits should have their condition staged and graded at each visit. Patients without neurological deficits should be monitored weekly for any signs of neurological compromise. Repeat X-rays of the spine should be conducted every 3 months. A repeat contrast-enhanced MRI should be performed after 6 months if there are concerns about an inadequate response to treatment.
Following 6 months of treatment, further evaluation is warranted only if there are concerns regarding inadequate therapeutic response, although this is not necessary in most cases.
At the conclusion of treatment (12 months), an assessment should be carried out to evaluate healing before therapy is terminated. If findings reveal inactive, burnt-out infections, such as bony or fibrous ankylosis or thin-walled cysts without enhancement, there is no need to continue with ATT. After the treatment ends, follow-ups should occur every 6 months for a minimum of 2 years.
Fig. 1 shows a sagittal view in a diagnosis of spondylodiscitis at the D12/L1 level. It is characterized by a Grade 1 collapse of both vertebral bodies, heterogeneous enhancement, a peripheral enhancing epidural abscess, and involvement of the psoas muscles, resulting in psoas abscess formation.
Fig. 2 shows a coronal view in a diagnosis of spondylodiscitis at the D12/L1 level. It is characterized by a Grade 1 collapse of both vertebral bodies, heterogeneous enhancement, a peripheral enhancing epidural abscess, and involvement of the psoas muscles, resulting in psoas abscess formation.
TB can impact any part of the body, including bones, with the spine being the area most frequently affected. Vertebral TB typically involves the lower thoracic and upper lumbar regions, while cervical spine infections are more perilous. The most prevalent symptom of vertebral TB is chronic back pain, which is often vague and can lead to diagnostic delays[6]. An exceptional level of scrutiny is necessary for early detection, as the presentation is subacute and non-specific. Failure to diagnose promptly can result in severe, irreversible outcomes, such as paraplegia, which are notably more common among patients with involvement of the upper and mid-thoracic spine due to the narrowest dimension of the spinal canal at T3–T10 [7].
TB may also present as a pseudo abscess, which can be classified into primary and secondary types depending on the underlying cause. Primary psoas abscesses usually arise from lymphatic or hematogenous dissemination from an undetected source and are more common in immunocompromised individuals, such as those having diabetes, HIV, kidney failure, or other conditions that suppress the immune system. The predominant organism implicated in this form is Staphylococcus aureus (88%), followed by Streptococcus and Escherichia coli.
Secondary psoas abscesses stem from an infection site near the psoas muscle and typically arise due to either peritoneal inflammatory processes or spinal conditions. While Crohn’s disease is the leading cause of secondary psoas abscesses globally, Pott’s disease is the most frequent cause in developing countries, such as India, particularly following the rupture of thoraco-lumbar abscesses.
The psoas abscess discussed here was a secondary type. Secondary psoas abscesses due to Pott’s spine are uncommon, develop gradually, and present non-specifically, as observed in this case. The clinical symptoms tend to be ambiguous, which can delay diagnosis and lead to irreversible harm. The classic triad of symptoms – fever, flank pain, and limited hip movement – occurs in only 35% of instances [8]. Symptoms, such as progressive back pain over several weeks, with or without accompanying muscle spasms or rigidity, may prompt a clinician to consider a spinal origin for the abscess.
MRI serves as the most sensitive imaging modality for diagnosing spinal TB, typically revealing spinal deformity, damage to the vertebral bodies and adjacent intervertebral discs, and cold abscesses in the surrounding tissues [9][10].
Tuli and Kumar have described the sequence of staging in Pott’s paraplegia as follows
The patient is unaware of any neurological deficit
· The physician notes plantar extensor response and/or ankle clonus, and the patient does not require walking support
· The patient recognizes the neurological deficit but can walk with assistance. The gait appears clumsy
· The patient is unable to walk and exhibits paralysis in extension, while sensory deficits are under 50%.
The patient cannot walk, lacks sensation or control over urine and or stools, shows paralysis in flexion, is flaccid, possesses sensory deficits exceeding 50%, and shows involvement of the sphincter function.
Surgical intervention becomes necessary in cases of neurological compromise, spinal instability, or unsuccessful medical treatment. Possible surgical procedures include decompression, debridement, instrumentation, and spinal fusion, which aim to alleviate spinal cord compression, remove infected tissue, and restore spinal stability. It is essential to conduct post-operative rehabilitation and ongoing monitoring to ensure a positive functional outcome and to prevent the recurrence of the disease.
Limitation
While this case provides valuable insight into the silent progression of Pott’s disease, it has several limitations. First, this report describes a single patient, which limits the generalizability of the clinical presentation, diagnostic approach, and treatment outcomes to a broader population. Second, because the patient was managed successfully with conservative anti-tuberculous therapy and bracing, there is no comparison with surgically managed cases, limiting conclusions regarding the relative efficacy of conservative versus operative treatment in similar presentations.
The follow-up duration was short to intermediate, and although significant clinical and neurological improvement was observed, longer follow-up would be required to fully assess long-term spinal stability, progression of deformity, recurrence of abscess formation, or late-onset neurological deterioration.
Finally, the insidious and atypical presentation without fever contributed to a diagnostic delay, which is a known challenge in spinal TB. This limitation makes it difficult to determine whether earlier diagnosis and intervention could have resulted in faster or more complete neurological recovery. The absence of fever – a classic teaching in medical education regarding infectious diseases – likely contributed to initial diagnostic uncertainty and delayed investigation. However, as emphasized in the literature, fever is absent in approximately 50% of spinal TB cases, particularly in insidious presentations
TB of the spine, or Pott’s disease, remains a significant health challenge worldwide, particularly in regions with a high prevalence of TB. Early recognition of clinical symptoms, coupled with appropriate diagnostic evaluation and multidisciplinary management, is essential for optimizing patient outcomes and reducing disease morbidity and mortality. The psoas abscess is clinically difficult to diagnose because of its rarity and non-specific clinical presentation.
The management of spinal TB presents various challenges, such as ensuring treatment adherence and addressing the development of multidrug-resistant strains. Preventing long-term consequences associated with spinal TB, including spinal deformations and neurological impairments, remains a significant challenge. Future research should prioritize enhancing diagnostic precision, innovating treatment approaches, and identifying the socioeconomic factors contributing to TB transmission and its overall impact.
This case emphasizes that afebrile, gradually progressive paraparesis with chronic back pain, unexplained weight loss, and atraumatic vertebral collapse should strongly prompt consideration of tuberculous spondylodiscitis with possible psoas abscess, even in the absence of pulmonary involvement or classical systemic symptoms. Early MRI of the dorso‑lumbar spine and timely microbiological/histopathological confirmation are crucial to detect epidural and psoas abscesses before irreversible cord damage occurs. With prompt, individualized anti-tubercular therapy, careful monitoring for drug‑induced hepatotoxicity, spinal bracing, and multidisciplinary conservative care, significant neurological and functional recovery is achievable, helping to prevent permanent disability.
References
- 1. Available from: https://www.clinicsinsurgery.com/open-access/spinal-tuberculosis-a-case-report-7035.pdf. [Last accessed on Dec 2025 12]. [Google Scholar] [PubMed]
- 2. Global tuberculosis report 2019. https://www.who.int/publications/i/item/9789241565714. [Last accessed on Dec 2025 12]. [Google Scholar] [PubMed]
- 3. Gupta RK, Lucas SB, Fielding KL, Lawn SD. Prevalence of tuberculosis in post-mortem studies of HIV-infected adults and children in resource-limited settings: a systematic review and meta-analysis. AIDS. 2015 Sep 24;29(15):1987-2002. doi: 10.1097/QAD.0000000000000802. PMID: 26266773; PMCID: PMC4568896. https://pubmed.ncbi.nlm.nih.gov/26266773/ [Google Scholar] [PubMed] [CrossRef]
- 4. Tuli SM: Epidemiology and prevalence. In: Tuli SM, editor. Tuberculosis of the Skeletal System. New Delhi, India: Jaypee Brothers Medical Publications. 2004, 1:12. [Google Scholar] [PubMed]
- 5. Jain AK, Dhammi IK. Tuberculosis of the spine: a review. Clinical Orthopaedics and Related Research®. 2007 Jul 1;460:39-49. https://pubmed.ncbi.nlm.nih.gov/17438468 [Google Scholar] [PubMed]
- 6. Garg RK, Somvanshi DS. Spinal tuberculosis: a review. J Spinal Cord Med. 2011;34(5):440-54. doi: 10.1179/2045772311Y.0000000023. PMID: 22118251; PMCID: PMC3184481. https://pubmed.ncbi.nlm.nih.gov/22118251/ [Google Scholar] [PubMed] [CrossRef]
- 7. Turgut M: Spinal tuberculosis (Pott’s disease): its clinical presentation, surgical management, and outcome. A survey study on 694 patients. Neurosurgical Review. 2001, 24:8-13. [Google Scholar] [PubMed]
- 8. Vijay Goni, Babu Ram Thapa, Sameer Vyas, Nirmal Raj Gopinathan, Sakthivel Rajan Manoharan, Vibhu Krishnan: Bilateral Psoas Abscess, Atypical Presentation of Spinal Tuberculosis. Archives of Iranian Medicine. 15:253-56. [Google Scholar] [PubMed]
- 9. Sharif HS, Morgan JL, Al Shahed MS, Al Thagafi MYA: Role of CT and MR imaging in the management of tuberculous spondylitis. Radiologic Clinics of North America. 1995:787-804. [Google Scholar] [PubMed]
- 10. Rasouli MR, Mirkoohi M, Vaccaro AR, Yarandi KK, Rahimi-Movaghar V. Spinal tuberculosis: diagnosis and management. Asian Spine J. 2012 Dec;6(4):294-308. doi: 10.4184/asj.2012.6.4.294. Epub 2012 Dec 14. PMID: 23275816; PMCID: PMC3530707. https://pubmed.ncbi.nlm.nih.gov/23275816/ [Google Scholar] [PubMed] [CrossRef]




Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Surgical Management of Pott’s Paraplegia in a 27-Week Pregnant Woman with Continuation of Pregnancy: A Case Report
May 1, 2026 Surgical Management of Pott’s Paraplegia in a 27-Week Pregnant Woman with Continuation of Pregnancy: A Case Report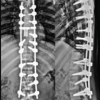 April 1, 2026 Multifocal Non-contiguous Spinal Tuberculosis: A Report of 3 Surgically-Treated Patients
April 1, 2026 Multifocal Non-contiguous Spinal Tuberculosis: A Report of 3 Surgically-Treated Patients March 1, 2026 Acute Cauda Equina Syndrome Due to Primary Lumbar Spinal Hydatid Cyst: A Rare Case
March 1, 2026 Acute Cauda Equina Syndrome Due to Primary Lumbar Spinal Hydatid Cyst: A Rare Case December 1, 2024 Management of Thoracolumbar Spinal Tuberculosis by Decompression and Posterior Stabilization with Pedicle Screw Fixation
December 1, 2024 Management of Thoracolumbar Spinal Tuberculosis by Decompression and Posterior Stabilization with Pedicle Screw Fixation