
Sequential bilateral prosthetic knee infections may necessitate different surgical strategies within the same patient; individualized decision-making and multidisciplinary management are crucial to achieve infection control while preserving function whenever possible.
Dr. Abdulelah Khamis Alqawlaq, General Medicine Practice Program, Batterjee Medical College, Jeddah, Saudi Arabia. E-mail: 150170.abdulelah@bmc.edu.sa
Abstract
Introduction: Prosthetic joint infection (PJI) is one of the most serious complications of total knee arthroplasty (TKA). Bilateral sequential PJI is rare and presents unique therapeutic challenges.
Case Report: This case reports a 68-year-old male with diabetes, hypertension, and peripheral vascular disease who developed infections in both knee prostheses. His left knee was treated with debridement, prosthesis removal, and spacer insertion, ultimately resulting in arthrodesis. A few months later, his right prosthesis became infected. During the first-stage revision arthroplasty, the components were removed, and a spacer was inserted. His clinical course was complicated by Clostridioides difficile colitis secondary to prolonged antibiotic therapy. Following stabilization, a second-stage revision TKA was performed, achieving full extension and 120° of flexion intraoperatively. The patient subsequently began rehabilitation at home.
Conclusion: This case highlights the divergent outcomes of sequential bilateral PJI and underscores the need for individualized surgical decision-making, antimicrobial stewardship, and multidisciplinary care.
Keywords: Prosthetic joint infection, total knee arthroplasty, arthrodesis, staged revision, infections.
Prosthetic joint infection (PJI) following total knee arthroplasty (TKA) remains a serious complication, with an incidence of approximately 1% after primary surgery and even higher in revision cases [1,2]. Its TKA is still associated with a relatively small, but potentially devastating complication of PJI, occurring in approximately 1% after primary TKA and even more in cases of revision [1,2]. Management consists of debridement and implant retention, one-stage revision, and two-stage revision, and recent studies have compared the rates of reinfection and reoperation among them [3,4]. Although unilateral PJI was well established, bilateral infection was rare. Case reports of both concomitant and staged (primary and sequential infections) bilateral prosthetic knee infectious processes and their treatment plans have been reported [5,6]. In cases of non-reconstructable or multiply revised arthroplasty, arthrodesis is an alternative technique of salvage. Recent reviews have shown excellent infection control with the use of modular knee arthrodesis systems and mechanical methods of external fixation at the expense of joint mobility [7,8]. Nevertheless, reimplantation following staged revision remains the referential treatment in order to recover mobility when it is possible [6]. Furthermore, extended antibiotic treatment may be associated with complications, such as Clostridioides difficile infection, which can lead to complicated surgical plans with subsequent delays in surgery [6].
The patient was a 68-year-old male who had been diagnosed with type 2 diabetes, hypertension, and left leg peripheral arterial disease after a stent procedure in the left femoral artery. He first showed an infected left total knee prosthesis (Fig. 1).
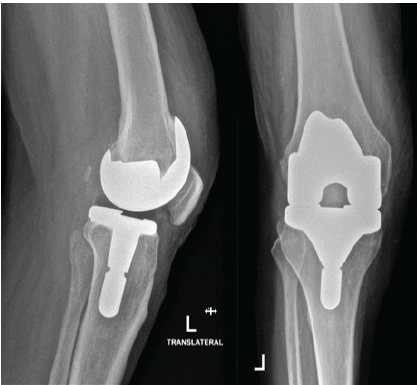
Figure 1. Left knee after total knee arthroplasty. Anteroposterior and lateral radiographs demonstrating the left knee following primary total knee arthroplasty prior to the onset of infection.
He underwent radical resection, the implant was removed, and a local cement spacer was implanted (Fig. 2).
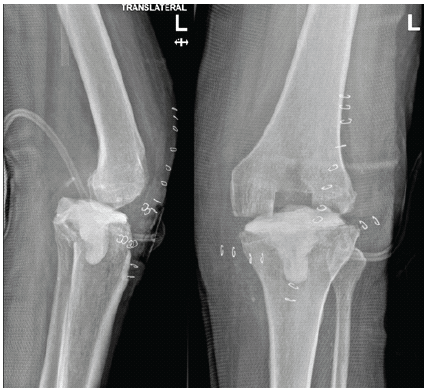
Figure 2. Left knee after implant removal and spacer insertion. Anteroposterior and lateral radiographs showing removal of the prosthetic components and placement of an antibiotic-loaded cement spacer as part of first-stage infection management.
A prolonged course of delayed wound healing, superficial cast-related sores, and progressive loss of motion occurred in the post-operative period. The mild anterior dislocation was evident on X-ray, and Ilizarov fixation was initially suggested. However, due to persistent infection, poor soft-tissue envelope, significant bone loss, delayed wound healing, and the patient’s multiple comorbidities, including diabetes and peripheral vascular disease, reimplantation was deemed high risk. After multidisciplinary discussion, knee arthrodesis was selected as a definitive salvage procedure to achieve infection control and limb stability. The patient subsequently underwent knee arthrodesis using external fixation, with successful fusion and resolution of infection. Final radiographs confirmed solid fusion of the left knee without evidence of recurrent infection (Fig. 3).

Figure 3. Left knee after arthrodesis. Anteroposterior radiograph demonstrating successful left knee arthrodesis with solid fusion following definitive salvage management for persistent prosthetic joint infection.
Several months later, he developed pain and swelling of the orthopedic knee prosthesis (Fig. 4).
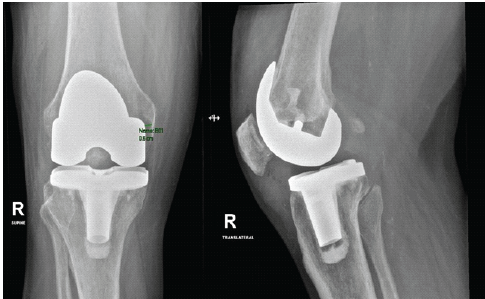
Figure 4. Infected right total knee arthroplasty with implant loosening. Anteroposterior and lateral radiographs demonstrating loosening of the right knee prosthesis consistent with prosthetic joint infection.
Reoperation was performed under spinal anesthesia for first-stage revision arthroplasty. When the quadriceps tendon was opened along a midline incision, pus was noted. Sampling was performed from different localizations, including suprapatellar, infrapatellar, capsular, and tibial localizations. The femoral and tibial components were removed using osteotomes and copious irrigation. A cemented antibiotic spacer was inserted (Fig. 5) with vancomycin powder, and the wound was closed over a suction drain.
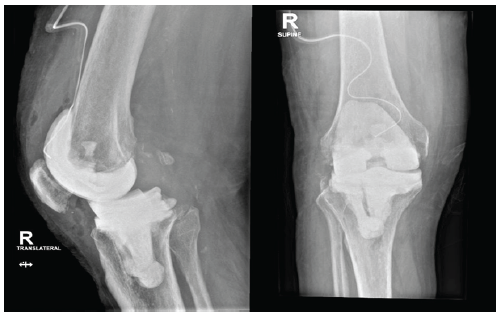
Figure 5. Right knee after first-stage revision with spacer insertion. Anteroposterior and lateral radiographs were obtained following removal of the infected prosthesis and insertion of an antibiotic-loaded cement spacer during first-stage revision arthroplasty.
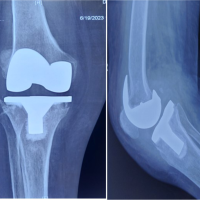
Postoperatively, he developed fever, abdominal pain, and diarrhea then later diagnosed as having Pseudomonas colitis induced by C difficile, attributed to long-term broad-spectrum antibiotic exposure. Managed by modifying his regimen to oral vancomycin, levofloxacin, and linezolid after infectious disease consultation. Despite systemic complications, the right knee remained stable, with preserved extension and flexion up to 90°. After stabilization, he underwent second-stage complex revision TKA (Fig. 6).
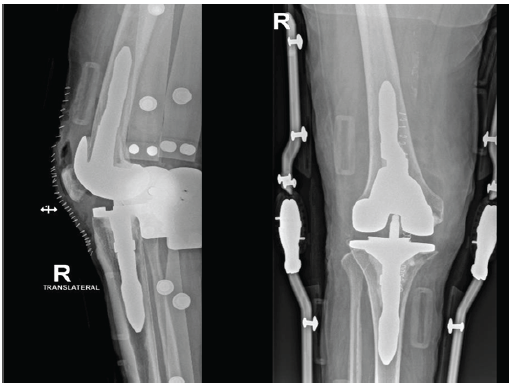
Figure 6. Right knee after second-stage revision total knee arthroplasty. Anteroposterior and lateral radiographs demonstrating successful second-stage revision with stemmed prosthetic components following eradication of infection.
Intraoperatively, the surgical field was clean, and the spacer was removed with minimal bone loss. Copious lavage was performed. Definitive components (Johnson and Johnson Attune system, femur size 5, tibia size 4 with stem, liner 5×7) were implanted. The medial and lateral collateral ligaments were stable, no patellofemoral maltracking was observed, and the intraoperative range was full extension and flexion up to 120°. Closure was completed in layers, and the distal neurovascular status was intact. Postoperatively, his vital signs were stable, pain was controlled, and the diarrhea gradually improved. He was discharged with a multidisciplinary home health plan, including orthopedic follow-up, weekly laboratories, and daily physiotherapy (Table 1).
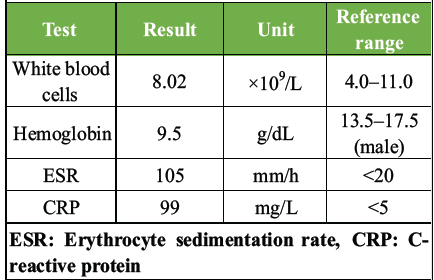
Table 1: Inflammatory and hematologic laboratory findings at presentation.
Follow up at 2 weeks, he maintained stable wound healing and clean, achieved flexion of 80 degrees with no pain, and continued rehabilitation.
At 12 months following the second-stage revision TKA of the right knee, the patient remained clinically stable with no evidence of recurrent PJI. There were no episodes of wound dehiscence, sinus tract formation, or hospital readmission related to infection. Serial inflammatory markers demonstrated sustained normalization, with C-reactive protein and erythrocyte sedimentation rate remaining within reference ranges throughout follow-up. Functional outcome at final follow-up was assessed using validated knee arthroplasty scoring systems. The Knee Society Score demonstrated a knee score of 82 and a function score of 70. The Oxford Knee Score was 34 out of 48, reflecting satisfactory knee-related quality of life. On physical examination, the patient achieved full extension (0°) and flexion up to 110°. He was able to ambulate independently indoors without assistive devices and used a single cane for longer outdoor distances. Stair climbing was possible with handrail support, and activities of daily living were performed independently. Pain levels were significantly improved compared to the pre-operative period. At 12 months, the patient reported a Visual Analog Scale pain score of 1 out of 10 at rest and 3 out of 10 during activity. Overall, patient satisfaction with the reconstructed right knee was high, particularly when compared with the functional limitations associated with the contralateral arthrodesed knee.
Regarding the left knee, the arthrodesis remained solid and painless at 12 months. Radiographs confirmed maintained fusion without evidence of mechanical failure or recurrent infection. Although the absence of knee motion resulted in expected functional limitations, the patient reported acceptable stability and pain-free weight bearing. Radiographic evaluation of the right knee at final follow-up demonstrated well-aligned prosthetic components without radiolucent lines, subsidence, or signs of loosening. Stem fixation remained stable, and no mechanical complications were identified. No recurrence of C. difficile infection was observed during the follow-up period. The patient completed post-operative infectious disease surveillance and antimicrobial therapy without further gastrointestinal or systemic complications.
This case is notable for the occurrence of sequential bilateral PJI, a rare clinical entity. This patient required two divergent management strategies, which were the left knee progressing to arthrodesis after implant removal, whereas the right knee was reconstructed through staged revision. The staged approach for the right knee aligns with recent meta-analyses supporting its use as a benchmark strategy for chronic PJI, despite ongoing debate about the relative benefits of one- versus two-stage revisions [7]. Arthrodesis, while sacrificing mobility, remains a reliable salvage option when reimplantation is contraindicated, with modern reviews confirming high fusion and infection-control rates [7,8]. The coexistence of both salvage formulations in the same patient is rarely documented in the literature, though recent bilateral PJI case reports point to the complexity and necessity of individualized decision-making in such scenarios [9]. Moreover, this patient’s antibiotic-associated C. difficile colitis is one of the challenges of balancing aggressive infection control against systemic risks, a complication increasingly recognized in arthroplasty populations receiving prolonged antibiotic therapy [9,10]. This case reinforces the importance of individualized, multidisciplinary management in elderly multimorbid patients with bilateral PJI, involving orthopedics, infectious disease, nephrology, vascular surgery, hematology, and rehabilitation medicine.
Sequential bilateral prosthetic knee infections are rare and may necessitate different surgical solutions within the same patient. This case demonstrates that arthrodesis remains a reliable salvage option when reconstruction is not feasible, while staged revision arthroplasty can successfully restore function when local and systemic conditions allow. The report reinforces the importance of individualized surgical planning, antimicrobial stewardship, and multidisciplinary management, and adds to the limited orthopedic literature addressing divergent strategies in bilateral PJI.
Sequential bilateral PJI should be managed with patient-specific strategies rather than uniform treatment. Careful patient selection, including assessment of host comorbidities, soft tissue condition, bone loss, and infection severity, is essential in determining the optimal surgical approach. In high-risk patients, strategies to reduce post-operative infection include pre-operative optimization of comorbidities, meticulous surgical debridement, appropriate antimicrobial therapy, and close multidisciplinary management, allowing staged revision in one knee and arthrodesis as a salvage option in the other when clinically indicated.
References
- 1. Weinstein EJ, Stephens-Shields AJ, Newcomb CW, Silibovsky R, Nelson CL, O’Donnell JA, et al. Incidence, microbiological studies, and factors associated with prosthetic joint infection after total knee arthroplasty. JAMA Netw Open 2023;6:e2340457. [Google Scholar] [PubMed]
- 2. Sarfraz A, Bussey-Sutton C, Ronan EM, Khury F, Bosco JA, Schwarzkopf R, et al. Incidence of PJI in total knee arthroplasty patients following expanded gram-negative antibiotic prophylactic protocol. Microorganisms 2025;13:1002. [Google Scholar] [PubMed]
- 3. Xie C, Pan W, Wang S, Yan X, Luo H. . Single-stage versus two-stage revision for periprosthetic joint infection after knee arthroplasty: A systematic review and meta-analysis. Knee 2024;46:12-20. [Google Scholar] [PubMed]
- 4. DeBoer AM, Van Roekel NL, Parkulo TD, Moua GY, Vang S, Marston SB. Comparison of single- versus two-stage revision knee arthroplasty for the treatment of periprosthetic knee joint infections. J Arthroplasty 2025;40:S514-9. [Google Scholar] [PubMed]
- 5. Alharbi YM, Alhumaidi IM, Alamri AJ, Jamal RS. Bilateral knee prosthetic joint infection: A case report. Int J Commun Med Public Health 2025;12:1488-92. [Google Scholar] [PubMed]
- 6. Burger P, Botros M, Quartuccio KS, Munsiff SS, Myers T. Bilateral Capnocytophaga canimorsus periprosthetic joint infections in an immunocompromised patient: A case report and literature review. Arthroplasty Today 2025;32:101664. [Google Scholar] [PubMed]
- 7. Büyükdoğan K, Öztürkmen Y, Goker B, Oral M, Atay T, Özkan K, et al. Early results of a novel modular knee arthrodesis implant after uncontrolled periprosthetic knee joint infection. BMC Musculoskelet Disord 2023;24:889. [Google Scholar] [PubMed]
- 8. Mercurio M, Gasparini G, Cofano E, Zappia A, Familiari F, Galasso O. Knee arthrodesis for periprosthetic knee infection: Fusion rate, complications, and limb salvage-A systematic review. Healthcare 2024;12:804. [Google Scholar] [PubMed]
- 9. Angerett N, Ferguson C, Kahan M, Fitz D, Hallock R. Cefadroxil-induced clostridium difficile infection following total knee arthroplasty. Arthroplasty Today 2022;18:52-6. [Google Scholar] [PubMed]
- 10. Deckey DG, Boddu SP, Verhey JT, Doxey SA, Spangehl MJ, Clarke HD, et al. Pre-operative Clostridioides difficile infection is associated with increased risk of periprosthetic joint infection. J Arthroplasty 2024;39:1011-8. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 May 10, 2024 Uncommon Pathogen: Achromobacter xylosoxidans Infection Following Total Knee Arthroplasty
May 10, 2024 Uncommon Pathogen: Achromobacter xylosoxidans Infection Following Total Knee Arthroplasty June 1, 2026 Efficacy of Tranexamic Acid in Reducing Blood Loss and Transfusion Requirements in Primary Total Knee Arthroplasty: A Prospective Comparative Study
June 1, 2026 Efficacy of Tranexamic Acid in Reducing Blood Loss and Transfusion Requirements in Primary Total Knee Arthroplasty: A Prospective Comparative Study June 1, 2026 A Comparative Study between Local Infiltration of Ropivacaine Cocktail and Post-operative Epidural Bupivacaine in Post-operative Analgesia in Primary Total Knee Arthroplasty
June 1, 2026 A Comparative Study between Local Infiltration of Ropivacaine Cocktail and Post-operative Epidural Bupivacaine in Post-operative Analgesia in Primary Total Knee Arthroplasty June 1, 2026 Short-term Clinical and Radiologic Outcomes, and Survivorship Following Primary Total Knee Arthroplasty Using a Novel High-Flexion System among Indian Patients
June 1, 2026 Short-term Clinical and Radiologic Outcomes, and Survivorship Following Primary Total Knee Arthroplasty Using a Novel High-Flexion System among Indian Patients